
記住我
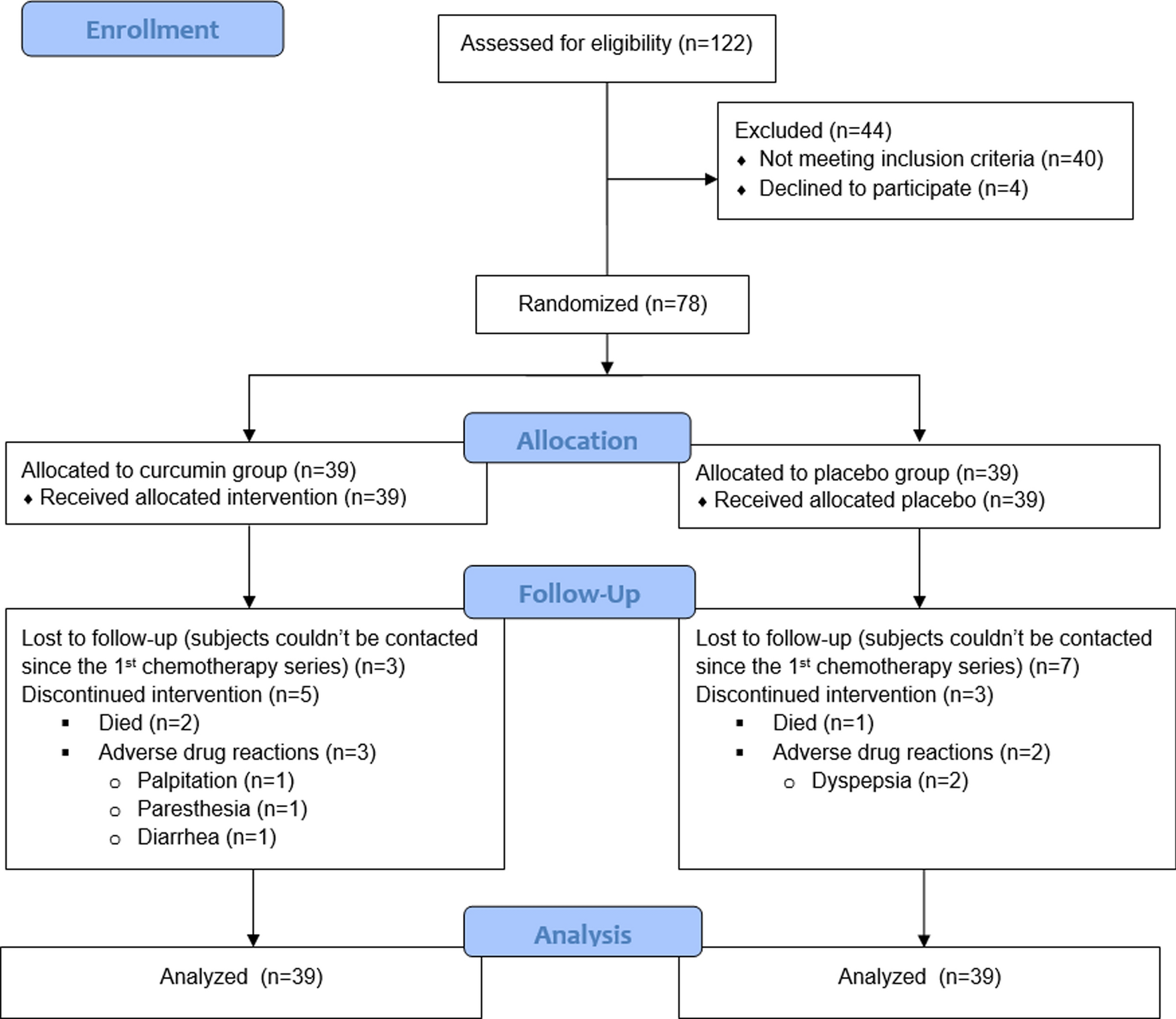







Steps of subjects’s selection can be seen in Fig. 1. A total of 122 subjects were evaluated according to the eligibility criteria in order to participate in this study. Among these, 40 people did not meet the eligibility criteria, 3 people refused to participate, and 1 person was not allowed to participate by the doctor in-charge of the patient. Thus, 78 people met the eligibility criteria and were randomized 1:1 to 39 people each allocated to each of the group (curcumin extract and placebo). Among all subjects, none refused the administered treatment. In the course of treatment, 3 and 7 subjects receiving curcumin extract and placebo respectively lost contact because they could not be contacted since the first series of chemotherapy. Furthermore, 2 and 1 person died in the curcumin extract and placebo groups, respectively, while 3 subjects in the treatment group suffered from unwanted drug responses including palpitations, paresthesias, and diarrhea (1 person each). Meanwhile, as many as 2 people on the placebo group had diarrhea. All subjects who experienced an undesirable drug response stopped participating in this study (dropped out), nevertheless, the data that had been obtained were still subjected to statistical analysis (ITT).
Fig. 1
A diagram of subjects’ selection process
Subjects’ baseline characteristicsThe basic characteristics of the research subjects can be seen in Table 1. Subjects in the placebo group had a tendency to be older, although not significant. The level of education has a relatively homogeneous distribution between groups with most of them having a high school education background. Meanwhile, some of the subjects in both groups had a diagnosis of cervical carcinoma stages 2 and 3. Meanwhile, approximately one third of the subjects in both groups had just undergone the second series of chemotherapy. The cumulative doses of the chemotherapy regimens of carboplatin and paclitaxel between the two groups were relatively homogeneous.
Table 1 Subjects’ baseline characteristicsThe scores of each AFI component 1–5 and 7–13 were not significantly different between groups of subjects receiving curcumin compared to placebo. Meanwhile, the mean score of AFI 6 was significantly higher in the group of subjects receiving curcumin (73.28 vs. 59.26; 95% CI 4.80–23.25; p = 0.003). Meanwhile, the initial data for the Stroop and MoCA-Ina tests were relatively homogeneous between groups.
Effect of curcumin extract on cognitive function and subjects’ effectiveness in performing daily activities subjectivelyThe role of curcumin extract on cognitive function and subjects’ effectiveness in performing daily activities were subjectively evaluated and compared with placebo. The patient’s cognitive function and independence in performing daily activities were evaluated using the AFI questionnaire. Groups of subjects receiving both curcumin extract and placebo were evaluated for differences in median and IQR AFI scores of each component at the end of the study period (after therapy) and baseline (baseline) [within group analysis]. Then the group of subjects who received curcumin extract was compared with the group of subjects who received placebo regarding the difference in the AFI scores of each component between the two (between group analysis).
Evaluation of the AFI component in the group receiving the curcumin extract showed a significant difference between the component 11 and 13 AFI scores, namely an increase in the median [IQR] of both components at the end of the treatment period compared to the baseline (AFI 11 median = 7.00, Z=-1.188, p = 0.235; AFI 13 median = 51, Z=-4.983, p < 0.001). This indicates that subjects receiving curcumin extract felt an increased frequency of errors in daily activities and mood changes to become irritable or irritable at the end of the study period. Meanwhile, the group receiving placebo also experienced a significant increase in AFI scores of components 12 and 13 at the end of the study period compared to baseline (AFI 12 median = 4.00, Z = − 1.966, p = 0.049; AFI 13 median = 9.00, Z = − 4.899, p < 0.0001). This also indicates worsening memory function and changes in the subject’s mood to become irritable and irritable at the end of the period compared to the beginning of the study.
The placebo group experienced an increase in AFI scores components 1, 2, 4–8 at the end of the treatment period than at the beginning of the study, but the placebo group also experienced an increase in AFI scores 10 to 13 which was inversely proportional to cognitive function and fluency in performing daily activities. This indicates an inconsistency in the subject’s personal perception of cognitive function and its impact on daily activities. Meanwhile, the group of subjects receiving curcumin showed a decrease in AFI scores of components 1, 5, 6, 7, 9 at the end of the treatment period compared to the beginning of the study, while the group also showed an increase in AFI scores of components 10, 11, and 13. This indicates that subjects receiving curcumin extract had a decreased perception of cognitive function and effectiveness in performing daily activities after receiving therapy.
According to between group analysis, there was no significant difference in median and IQR between groups receiving curcumin extract versus placebo for all components of the AFI score (Table 2). Thus, the personal perception of cognitive function in the two groups of subjects is relatively comparable and tends to worsen with increasing cycles and doses of chemotherapy.
Table 2 Subgroup analysis of each AFI components between treatment and control groupEffects of curcumin extract on selective attention and subjects’ executive functionFurthermore, an analysis was carried out regarding the role of curcumin extract on subjects’ selective attention and executive function which were evaluated objectively using the Stroop test. The groups of subjects who received both curcumin extract and placebo were evaluated for differences in median and IQR of final (after treatment) and baseline (baseline) IG scores [within group analysis]. Then the group of subjects who received curcumin extract was compared with the group of subjects who received placebo regarding the difference in GI scores between the two (between group analysis). Based on Table 3, it was known that there was a statistically significant difference between the median initial and final IG scores in the group receiving curcumin extract. IG experienced a significant increase (∆ median = 8.57) indicating an improvement in selective and executive attention function in subjects who had CICI but consumed curcumin extract (Z = − 4.503; p < 0.0001). Furthermore, there was also an improvement in the IG score of the placebo group at the end of the examination compared to the baseline condition, namely an increase of 2.46 points (∆ median), but not statistically significant (Z= − 1.762; p = 0.078).
Table 3 IG Score Profiles at beginning and end of study period between treatment and control groupBetween group analysis showed that the median difference in IG scores (∆ median = 5.76) was significantly higher in the group receiving curcumin extract (median [IQR] = 4.70 [9.74]) compared to placebo recipients (median [IQR]) = − 1.06 [6,2]; Mann–Whitney U = 268.5; p < 0.0001). This indicates that the administration of curcumin extract in patients with CICI provides a protective and curative effect on selective attentional and executive functions significantly compared to placebo.
Effects of curcumin extract on overall cognitive functionGlobal cognitive function was evaluated based on the MoCA-Ina score. Comparison of MoCA-Ina scores was carried out before and after therapy (within group analysis) in each treatment group and the difference in the mean difference in MoCA-Ina scores between groups at the end of the study period (between group analysis). Based on Table 4, there was an improvement in the MoCA-Ina score at the end of the treatment period compared to the baseline (baseline). The difference in the mean improvement of MoCA-Ina scores in the group receiving curcumin extract was 1.53 points, which was statistically significant (Z = − 2.99; p < 0.003). Meanwhile, improvements in MoCA-Ina scores were also found in the placebo group, although with a smaller difference in scores, namely 0.72 points and statistically significant (Z = − 2.05; p = 0.04).
Table 4 MoCA-Ina profile scores at the beginning and end of the study period between treatment and control groupFurthermore, an intergroup analysis was conducted with respect to the difference in the mean MoCA-Ina scores between the groups receiving curcumin extract and placebo. The results obtained that the difference in the mean MoCA-Ina scores was higher in the curcumin receiving group (1.54 ± 3.09) than the placebo (0.72 ± 1.99) with a mean difference between groups of 0.82 points but not statistically significant (Mann–Whitney U 615.5, p = 0.142).
Subgroup analysis showed a non-significant difference between the mean differences of each component of MoCA-Ina between treatment groups. Similarly, based on subgroup analysis of each component of MoCA-Ina in each treatment group (within group analysis). In general, the results were not much different between before and after the treatment period with a few exceptions. The group receiving curcumin extract experienced improvements in naming function (∆ mean ± SD = 0.18 ± 0.51; Z = - 1.072; p = 0.038) and memory delay (∆ mean ± SD = 0.56 ± 1.21; Z = − 2.654; p = 0.008) which was statistically significant after the treatment period. Meanwhile, in the placebo group, there was a statistically significant improvement in orientation function between before and after the treatment period (∆ mean ± SD = 0.31 ± 0.69; Z = − 2.588; p = 0.01).
Effect of curcumin extract on neuronal damage, inflammatory, and oxidative stress biomarkersThe administration of curcumin extract significantly decreased the median GFAP, IL-6, and Isoprostane in the treatment group, while in the control group, the median GFAP, IL-6, and Isoprostane tended to increase. In the treatment group, the median difference in the largest decreases was obtained sequentially, namely IL-6, isoprostane, and GFAP. Meanwhile, in the control group, the median difference in the largest increases was obtained sequentially, namely isoprostane, IL-6, and GFAP (Table 5).
Table 5 Median changes of GFAP, IL-6, and Isoprostane at the beginning and end of the study period between treatment and control group
留言 (0)