
記住我
The physiology of female reproduction is a complex and delicate interplay between neuroendocrine signals involving the hypothalamic-pituitary-ovarian (H-P-O) axis. Elements that disturb the balance of these interactions can cause metabolic and reproductive disorders.
Alterations in the proper functioning of the H-P-O axis signals are frequent in overweight or obesity [1].
Leaving aside the role that excessive adiposity can play in the delicate moment of the onset of puberty [2], further repercussions can be certainly seen in adulthood, with an impaired reproductive sphere [3]. The presence of adiposity can interfere with the physiological functioning of the H-P-O axis both directly, by disrupting the pituitary luteinizing hormone (LH) pulse amplitude and its average release without changing its frequency and determining an impaired luteal phase [4], either indirectly, through major adiposity-related alterations, such as insulin and leptin resistance and Low-Grade Chronic Inflammation (LGCI) [4].
One of the most prevalent disorders of the reproductive age encompassing all these alterations with a close link between H-P-O axis and metabolic perturbations is the Polycystic Ovary Syndrome (PCOS).
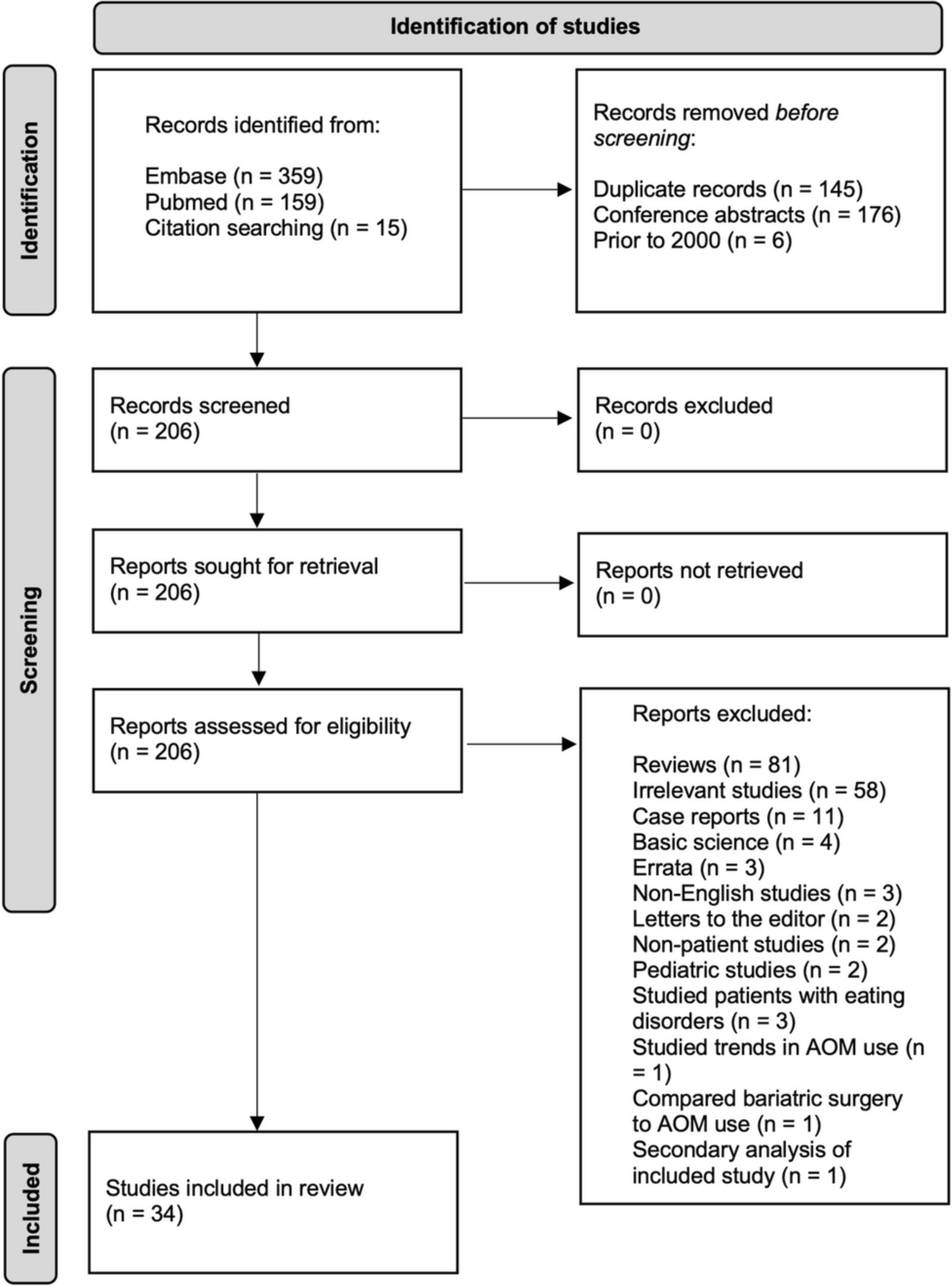
The purpose of this review is to address the major alterations related to adiposity and its interaction with the H-P-O axis in PCOS, focusing on insulin resistance (IR), leptin resistance, and LGCI. Furthermore, our aim goes beyond the consideration of currently available hormonal treatments, but aims to provide an overview of nutraceutical and/or pharmacological therapeutic strategies for the adjuvant treatment of inflammation and metabolic alterations typical of PCOS, in order to enable a more comprehensive and synergistic treatment. Substances such as Polyunsatured Fatty Acids (PUFAs) and Polyphenols will be reviewed on the one hand and anti-inflammatory molecules, Glucagon-like Peptide 1 (GLP-1) analogs, and Sodium-Glucose Transport Protein 2 (SGLT2) inhibitors on the other (Fig. 1).
Fig. 1
PCOS physiopathology and therapeutic options for the management of metabolic and inflammatory aspects. VAT: Visceral Adipose Tissue; SAT: Subcutaneous Adipose Tissue; Red arrows: Adiposity pattern; Orange dotted arrows: Low-grade chronic inflammation pattern; Blue arrows: Hyperandrogenism pattern; Green arrows: Therapeutic options
H-P-O axis and Polycystic Ovary SyndromeThe H-P-O axis is responsible for allowing procreation by cyclically producing gonadotropic and steroid hormones [5].
Starting from the hypothalamus, gonadotropin-releasing hormone (GnRH) triggers the release by the pituitary gland of the two gonadotropins, follicle-stimulating hormone (FSH) and luteinizing hormone (LH), which, in turn, exert their action peripherally on the ovaries to stimulate follicular growth and lead to the production of estradiol and, after ovulation, progesterone [1]. When estradiol reaches a constant threshold in terms of concentration (generally greater than 200 pg/mL) and duration, for at least 24–48 hours, it provides positive feedback that increases the frequency and decreases the amplitude of GnRH pulses, thus triggering the increased pituitary release of LH for ovulation [1]. Then, through a negative feedback mechanism, estradiol, together with inhibin B, acts on the hypothalamus suppressing FSH release [6]. One of the most common endocrine and metabolic disorders of the reproductive age in women is the PCOS which is considered part of ovulation disorders involving dysfunction of the H-P-O axis and is often accompanied by alterations in glucose metabolism, hyperinsulinaemia, hyperleptinemia, cardiovascular diseases, infertility and psychiatric disorders [5, 7, 8••].
The diagnosis of PCOS is made by the presence of at least 2 of the Rotterdam criteria [9] including oligo-ovulation or anovulation, clinical and/or biochemical signs of hyperandrogenism and polycystic appearance of the ovaries on ultrasound examination. The etiopathogenesis of PCOS is still not entirely clear, since there are numerous hypotheses but none of them are really established and indisputable. Genetic factors or multiple environmental drivers such as lifestyle, obesity, other endocrinological disorders such as dysthyroidism or impaired adrenal function, and endocrine disruptors are mentioned among the possible causes of PCOS [9].
In particular, as an hallmarks of the disease, in comparative studies between women with PCOS and healthy controls it has been described an impairment (much more often a decrease) in LH pulse amplitude not always accompanied by an increase in LH pulse frequency, with similar FSH levels between the two groups [4]. This dysbalancing in LH pulse amplitude and frequency would appear to be caused by an alteration in the pulsatile secretion of GnRH by the hypothalamus [5].
The primum movens of altered GnRH secretion is not yet entirely clear and the complexity of its regulation is directly proportional to the complexity of the mechanism. It has been observed that insulin is one of the elements that can disrupt the proper functioning of the H-P-O axis, being able to increase the frequency and amplitude of the secretion of GnRH and LH pulses through the upregulation of GnRH gene expression in hypothalamic GnRH neurons by activation of the MAPK pathway [10].
The persistently rapid pulsatility of GnRH, which promotes greater pituitary synthesis of LH than that of FSH resulting in increased LH concentrations and LH:FSH ratio (normal value <2) is typical of this disorder. This represents a physiological stimulus for androgen synthesis by theca cells and the cause of hyperandrogenism in PCOS [11] because in the ovaries, LH dose-dependently regulates the activity of cytochrome P450c17, the enzyme that limits the rate of sex steroid synthesis in theca cells. But, as in a vicious circle, androgens themselves have been shown to increase the frequency of GnRH pulses through inhibition of negative feedback from sex steroids on LH secretion, which eventually leads to increased LH and androgen levels [12].
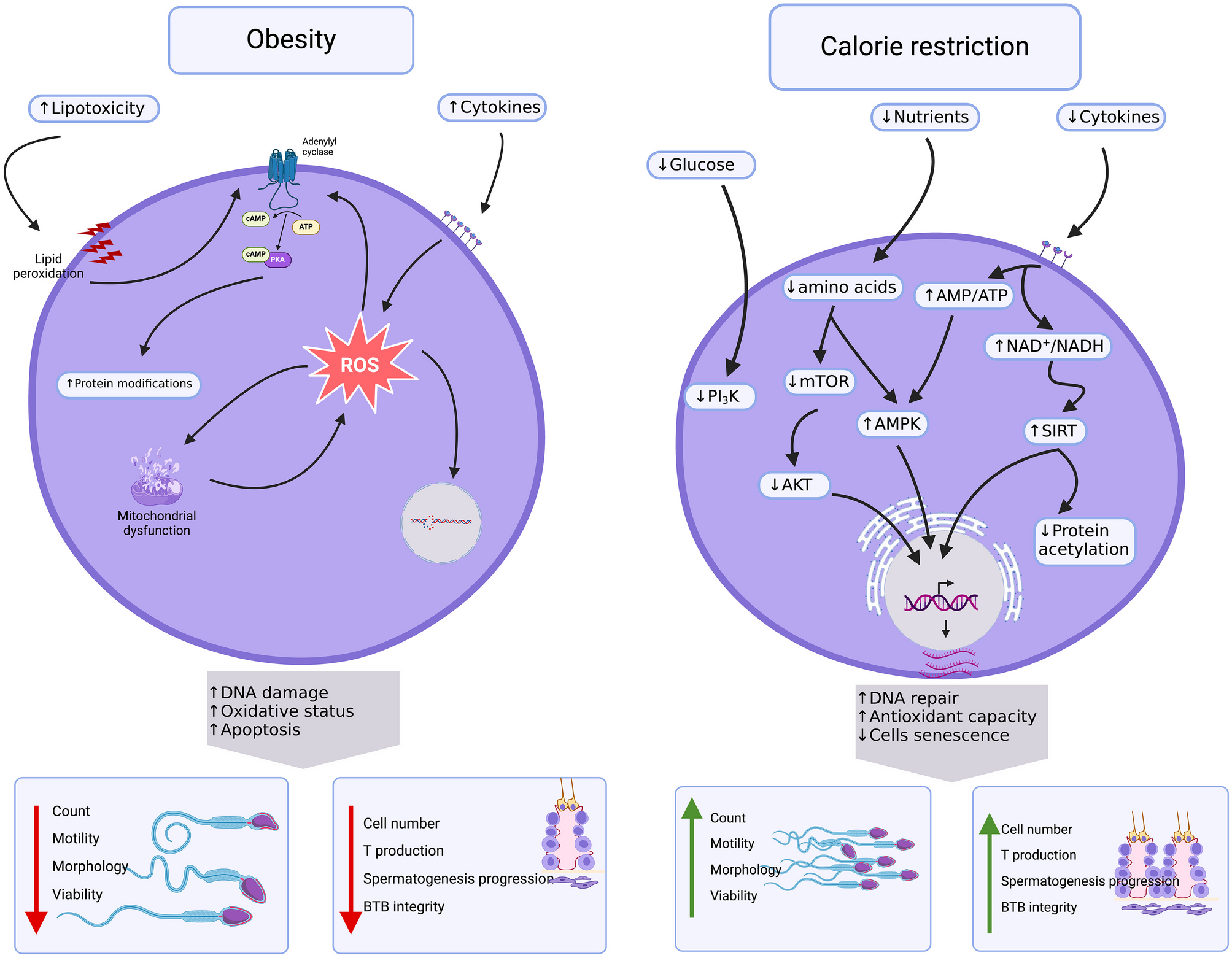
Among the most important metabolic consequences of hyperandrogenism in PCOS is reported an altered body fat distribution, as excess androgen masculinizes the fat distribution pattern, promoting visceral fat accumulation and increasing its thickness [13] (Fig. 2).
Fig. 2
Impaired hypothalamic GnRH secretion and its main physiological and metabolic consequences in PCOS
All this leads to harmful metabolic consequences for PCOS patients, as increased visceral adiposity is a risk factor for the development of metabolic syndrome and cardiovascular diseases [14].
Adiposity and Alterations of the H-P-O axisAlthough the underlying pathological mechanisms are not exactly known, the association between obesity, particularly visceral obesity, and ovulatory disorders secondary to neuroendocrine alterations of the H-P-O axis is now well established [15].
Women with a surplus of visceral adipose tissue also have increased ovarian androgen production, likely caused by elevated insulin levels that often occur with obesity [16]. The exceeding overactive androgens are aromatized into estrogens at high rates in the periphery, causing negative feedback on the H-P-O axis and affecting gonadotropin production [17]. Moreover, as in a self-feeding cycle, high androgen levels in PCOS lead to visceral fat deposition, resulting in IR and hyperinsulinemia, further stimulating ovarian and adrenal androgen production. This turns into menstrual abnormalities and ovulatory dysfunction [18].
It has also been shown in several studies that women with PCOS have significantly higher amounts of body fat and less lean body mass than controls with the same age, weight and Body Mass Index (BMI). A similar situation is found in a murine model of PCOS, in which affected mice had a higher proportion of fat deposition from 6 months of age and a higher rate of metabolic and reproductive abnormalities than healthy controls [19].
The main negative effects of over-adiposity on the H-P-O axis are exerted directly, through a decreased pituitary LH pulse amplitude and mean LH release without changing its frequency, impairing luteal phase [4], or indirectly mainly through metabolic changes coexisting with obesity such as hyperinsulinemia and hyperleptinemia, that exerts pro-inflammatory activities, stimulating immune cells and also fueling insulin resistance [20] and LGCI. Indeed, increased body fat is often associated with visceral adiposity and IR, allowing adipose tissue to be identified as a source of cytokines [21] causing LGCI and dysovulatory infertility.
Low-Grade Chronic InflammationAs mentioned above, although PCOS recognizes a multifactorial etiology, one of the key players involved in its pathogenesis is certainly LGCI, which, in this case, acts at both the systemic and ovarian levels and would appear to play a cause-and-effect role in the disease, representing an important link to the metabolic perturbations that accompany PCOS [8••].
In the framework of systemic inflammation, previous studies have reported that significantly higher concentrations of inflammatory cells with increased whole leukocyte lineage and dysregulation between regulatory T cells and T cells have been detected in the peripheral blood of PCOS patients [22]. In several studies, in addition to alteration in leukocyte counts, high levels of pro-inflammatory molecules, such as Interleukin-6 (IL-6), Tumor Necrosis Factor-α (TNF-α), C-reactive protein (CRP), high-sensitivity CRP, and low levels of anti-inflammatory molecules namely Transforming Growth Factor-β (TGF-β) and Interleukin-10 (IL-10) have been found in both serum and follicular fluid of women with PCOS as compared with healthy controls [23, 24].
In particular, it has been described that IL-6, together with TNF-α, might be involved in this process, all the more so in the presence of PCOS-related metabolic perturbations, although the data in the literature in this regard are inconsistent [25]. Indeed, in some cases, in normal weight or slightly overweight women with PCOS, IL-6 and TNF- α levels were found to be elevated compared to both healthy and obese control women [26,27,28,29], suggesting that increased circulating pro-inflammatory cytokines might be a feature of the PCOS pathology.
On the other hand, some other studies have associated the pro-inflammatory profile that occurs in PCOS [25, 30] with adiposity or obesity that could be indicated as the major determinant of serum inflammatory markers [31]. Furthermore, in another work, IL-6 and TNF-α circulating levels have been demonstrated to positively correlate with insulin resistance in obese women with PCOS [32].
Increased circulating levels of IL-6 lead to the activation of a subset of pro-inflammatory T-helper 17 (Th17) cells that, by increasing IL-21 expression, stimulate the release of the inflammatory cytokines IL-17A and IL-17F. TNF-α, at the same time, has the ability to directly stimulate the expression of IL-6 and cooperate with IL-23 to promote the expression of IL-17A [32]. IL-17A and IL-17F might be involved in the onset of the inflammatory profile in PCOS possibly by acting in synergy with TNF-α leading to the increase of IL6 production and contributing to an inflammation-related oxidative stress [32].
IL-6 also regulates CRP synthesis in the liver and is closely associated IR, obesity, cardiovascular disease [31] and increased androgen levels [33]. This increase in circulating pro-inflammatory cytokines well describe the systemic inflammation state driven by PCOS, and influenced by the associated metabolic dysfunction. At the local level, although mild ovarian inflammation is physiological in folliculogenesis during ovulation, when excessive, it can cause defects in oocyte quality, oligo-anovulation, and therefore cause infertility [34].
In a study by Xiong et. Al, by immunohistochemical staining of the ovaries of women with PCOS, an infiltration of large numbers of macrophages and lymphocytes was demonstrated, consistent with a condition of LGCI [35].
Ghowsi et al. demonstrates, in rats with PCOS, a higher representation of visceral fat and percentage of total fat compared with controls and higher mRNA expression of IL-6 and TNF-α within the visceral adipose tissue [36].
In fact, an important site of production of these inflammatory cytokines is precisely the adipose tissue [37] and in particular that with abdominal localization.
Furthermore, TNF-α plays a role in the pathogenesis of obesity-associated IR by blocking insulin receptor tyrosine kinase phosphorylation [38]. It also impairs glucose transport by reducing the activity of insulin-induced glucose transporter type 4 (GLUT-4) [39].
The above observations reinforce the idea that systemic and local inflammation links obesity, insulin resistance, and as a consequence, diabetes, which are very frequent metabolic alterations in PCOS [40], although further investigation is needed both at basic and clinical levels to dissect the cellular and molecular role of the inflammatory molecule in PCOS.
Insulin-ResistanceInsulin is a 51-amino acid protein produced in pancreatic β-cells. It is the prototypical hypoglycemic molecule and promotes glucose uptake by insulin-sensitive organs and tissues. Given its hypoglycemic role, its secretion is stimulated by plasma levels of glucose produced following ingestion of food or, directly, by specific amino acid [41].
Conditions such as obesity or PCOS itself are associated with hyperinsulinemia and IR when, despite normal pancreatic function, the insulin produced fails to carry out its action and accumulates in the plasma [42].
IR has been described to be intrinsic to PCOS, independently of adiposity [43].
A possible mechanism for IR in women with PCOS appears to be related to excessive serine phosphorylation of the insulin receptor. Specifically, serine phosphorylation of the insulin receptor substrate-1 (IRS1) and insulin receptor substrate-2 (IRS2), leads to inhibition of insulin signaling. Furthermore, the auto-phosphorylation of insulin receptor induces a decreased expression of GLUT-4, which is the insulin-sensitive glucose transport protein. Hyperinsulinemia results in an increased risk for many diseases including, type 2 diabetes (T2D), hypertension, dyslipidemia, endothelial dysfunction (ED), atherosclerosis, and cardiovascular diseases [44]. Hyperinsulinemia also can cause reduced production of Sex Hormone Binding Globulin (SHBG) by the liver and, consequently, leads to increased levels of circulating steroid hormones, such as estrogen and androgens [45]. A possible mechanism leading to increased androgen levels comes through the binding of insulin to its receptors on theca cells, inducing an increase in LH activity at the ovarian level, which, in turn, stimulates androgen production and secretion [46]. So much so that in PCOS, hyperinsulinemia is often associated with high LH levels and biochemical hyperandrogenism, which, in turn, triggers adipose tissue dysfunction [47]. Although insulin resistance is associated with hyperandrogenism and anovulation, an excess of androgens is recognized among the possible causes of insulin resistance in PCOS [48].
Beside peripherally, insulin can also contribute to the development of PCOS through its actions at the central level. Indeed, insulin can influence the activity of hypothalamic Proopiomelanocortin (POMC) producing neurons in the arcuate nucleus that present insulin receptors, as well as leptin receptors [49]. In fact, transgenic mice lacking the insulin receptor and the leptin receptor in POMC neurons have been shown to induce the PCOS phenotype, indicating that insulin and leptin may be potent regulators of POMC neurons, further contributing to the development of PCOS [19].
Thus, IR, hyperandrogenism, hyperleptinemia, LGCI and adipose tissue hypertrophy and dysfunction may cooperate in the vicious cycle that contributes to the etiopathogenesis of PCOS [50].
In addition, we should taking into account that in PCOS, IR can induce an inflammatory response that increases nuclear factor-κB (NF-κB) activation, oxidative stress and altered release of TNF from circulating mononuclear cells (MNCs). It has been clarified that oxidative stress has an important role in LGCI and can be significantly augmented in PCOS by expression of pro-inflammatory cytokines [51]. Moreover, considering insulin also as an adipogenic factor, by increasing body fat mass stimulates leptin expression and secretion. In turn, leptin inhibits pancreatic β-cell functions through direct and indirect actions of central neuronal pathways [52].
Leptin-ResistanceLeptin, first identified in 1994, belongs to the adipokine family and is a 16 kDa peptide hormone encoded by ‘ob’ gene [34]. This hormone plays a pivotal role in regulating food intake and energy homeostasis by acting on the Central Nervous System (CNS) and signaling that adequate energy store are available for the reproduction [53, 54].
Actually, compelling findings have well established that leptin is an extremely versatile hormone which regulates not only body weight and energy homeostasis, but is also involved in immune and neuroendocrine functions and in several other physiological processes such as inflammation, thermogenesis and angiogenesis and reproductive functions [55, 56].
Leptin performs its action by binding to specific leptin receptors (LEPRs), members of the class I cytokine receptor superfamily, with six known isoforms which differ from each other in the size of the intracellular domain and in the tissue expression level [57,58,59].
LEPR-b, which contains a long intracellular domain, is expressed at high levels in many human brain structures such as hypothalamic nuclei and the cerebellum and is the major isoform responsible for signal transduction of this adipokine [60, 61].
The signaling pathway primarily implicated in leptin signaling is that of JAK/STAT, which involves the activation of Janus kinase 2 (JAK2) and leads to inhibition of the synthesis of many orexigenic neuropeptides, while stimulating the production of some anorexigenic neuropeptides [62]. In detail, this adipokine acts at the level of the arcuate nucleus of the hypothalamus, inhibiting the synthesis of neuropeptide Y (NPY), a neurotransmitter that promotes appetite, and of the oressizing Agouti-related peptide (AgRP); moreover, it also inhibits the production of the hormone concentrating the melanin (MCH) and orexins, powerful appetite promoters [62]. In addition, leptin by binding LEPR-b stimulates neurons to synthesize POMC, the precursor of melanocyte-stimulating hormone-α (α-MSH); the latter is an anorexigenic neuropeptide that decreases food intake. Furthermore, leptin stimulates neurons to synthesize the CART (cocaine-amphetamine-regulated transcript), another molecule capable of inhibiting appetite [62].
In addition to its function in hunger/satiety control, numerous associations have demonstrated the involvement of leptin in reproduction. Specifically, in humans, subjects lacking leptin or functional LEPRs do not reach pubertal maturity and have low serum levels of both FSH and LH [63] indicating the existence of a critical leptin concentration threshold for the onset of the menstrual cycle and the functioning of the reproductive system in women [55, 64].
It also acts as a key regulator and stimulator of the H-P-O axis modulating GnRH secretion in the arcuate hypothalamic neurons in a dose-dependent manner [55]. The regulation of GnRH function in turn regulates gonadotropin secretion and, as GnRH neurons in the preoptic area do not express LEPR-b, GnRH-producing cell bodies are not directly influenced by leptin but by other neuropeptides whose production is influenced by leptin such as NPY, PMOC and kisspeptin, which is an hypothalamic peptide encoded by the KISS1 gene with a key role in regulation of the H-P-0 axis [55, 65]. Specifically, this peptide is widely reported as a key factor in the regulation of LH and FSH secretion and its levels were found to be higher in women with PCOS leading to enhanced H-P-O axis activity, thereby causing irregular menstrual cycles and excessive androgen release in PCOS population [66].
Besides, leptin exerts also effects on the adenohypophysis causing a dose-related increase in LH, FSH and prolactin release through nitric oxide synthase activation [67]. In this regard, several trials have reported that inhibition of LH secretion by dietary restriction was reversed with leptin administration, demonstrating a positive association between LH secretion and leptin [68, 69] and supporting the hypothesis that leptin acts as permissive factor in the development of puberty [70].
LEPRs have been identified in granulosa, theca and interstitial cells of the human ovary. The expression of these receptors in granulosa cells, which synergize with glucocorticoids to promote steroidogenesis, indicates that leptin exerts a direct regulatory action in ovarian folliculogenesis. Furthermore, it has been shown to modulate LH-stimulated estradiol production in the ovary [71].
Circulating concentrations of leptin are generally <10 ng/ml [72] and are influenced by several factors; one of the most important is definitely the amount of adipose tissue. In fact, it has been shown that subjects with obesity have higher leptin levels than subjects of the same age and gender who have a normal weight [73, 74]. Despite an increased level, however, this leptin fails to perform its action adequately; this leads to hypothesize a condition of leptin-resistance, which also involves its receptor. So much so that it has been shown that a chronic increase in leptin levels in the central nervous system leads to a decrease in the expression of LEPRs and in signal transduction [75].
In the pathogenesis of PCOS the role of leptin, and particularly leptin resistance, is not entirely clear but it has been hypothesized that in this disorder the simultaneous presence of insulin resistance and leptin resistance and the interaction between these two hormones is the main one to play an important pathogenetic role.
Confirming this, Hill et al. [19] showed that deletion of leptin and insulin receptors in POMC neurons of female mice resulted in weight gain, insulin resistance, elevated testosterone concentrations, elevated LH concentrations, increased ovarian follicle degeneration, and impaired fertility, all characteristics associated with PCOS.
Furthermore, high leptin concentration in the ovary, is able to suppress estradiol production and interfere with the correct development of dominant follicles and oocyte maturation, predisposing to anovulation. Accordingly, in conditions with excess energy store or metabolic disturbance, as obesity and/or PCOS, leptin has an inhibitory effects on the gonads and induces H-P-O dysfunction [76].
The disturbance of H-P-O axis is suspected to be the main culprit in the development of PCOS and future studies investigating the relationships between leptin and other hormonal and metabolic factors such as LH and IR are needed to debate the role of leptin in the etiopathogenesis of PCOS.
留言 (0)