
記住我





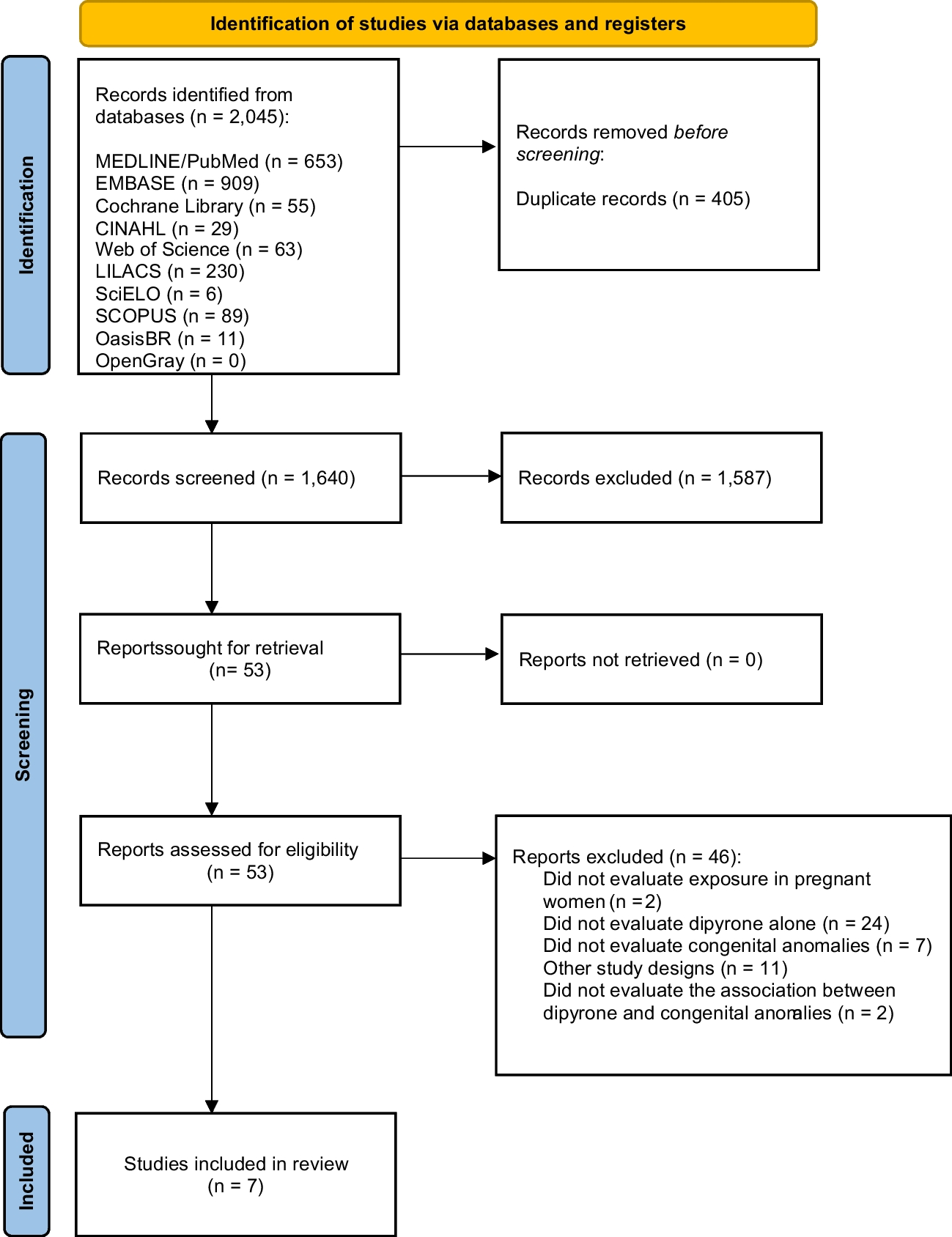


A flow diagram showing the study selection process is provided in Fig. 1. Ten articles were considered eligible for inclusion in the systematic review. These included eight single-arm cohort studies and two RCTs [2, 13, 22,23,24,25,26,27,28,29]. The basic characteristics of the included studies are summarized in Table 1. Furthermore, most of these studies were conducted in Europe [2, 22, 23, 25, 27], North America [13, 28, 29], or both [24]; only one was conducted in Asia [26].
Fig. 1
Flow chart of the literature search
Table 1 Basic characteristics of included clinical trialsThe mean or median baseline PCDAI was above 30 in four treatment arms of three studies, signifying moderate to severe disease [22,23,24]. The mean or median baseline PCDAI was between 10 and 30 in five studies, indicated mild disease on average [2, 13, 26, 28, 29]. Two studies did not report baseline disease severity [25, 27].
The two RCTs comprised four treatment arms, with all patients the randomly assigned at week 4 after induction treatment [24, 26]. In one of these RCTs, the efficacy of different maintenance treatment doses (high doses, 40 mg or 20 mg for body weight ≥ 40 kg or < 40 kg, respectively, and low doses, 20 mg or 10 mg for body weight ≥ 40 kg or < 40 kg, respectively) were investigated [24], whereas the efficacies of proactive (trough concentrations measured at weeks 4 and 8 and then every 8 weeks until week 72) and reactive monitoring (physicians were informed of trough concentrations after loss of response) were compared in the other [26].
The therapeutic dose of ADA varied widely among the included studies. Most subjects received standard adult ADA induction (160/80 mg) via subcutaneous injection, every other week (eow). A maintenance dose of 40 mg was used in 8 of the 12 treatment arms. Furthermore, in one treatment arm, a higher maintenance dose (80 or 40 mg for body weights ≥ 40 kg or < 40 kg eow, respectively) was used, while a lower maintenance dose was used in one of the therapeutic arms in the RCT study described above (20 or 10 mg for body weights ≥ 40 kg or < 40 kg eow, respectively).
The subjects in three studies were IFX-naïve [26,27,28]. Additionally, participants in two studies had previously received IFX treatment, which was discontinued due to loss of efficacy or related adverse events [2, 25]. In the remaining five studies, some subjects experienced IFX failure prior to ADA therapy [13, 22,23,24, 29].
Quality assessmentThe methodological quality of the two RCTs is summarized in Figs. 2 and 3. One of the RCTs was a phase 3, multicenter, randomized, open-label induction followed by a double-blind maintenance trial, in which subjects were randomly assigned (1:1) high-dose or low-dose ADA. Furthermore, in this study, subjects were stratified according to their week-4 responder status and prior exposure to IFX [24]. The other study was a multicenter RCT, with equal randomization (1:1 ratio), and aims to determine whether proactive therapeutic drug monitoring (TDM) is superior to reactive TDM in children with CD under scheduled monitoring of clinical and biologic measures. Therefore, based on the study design, it was not possible to fully blind the method [26].
Fig. 2
Risk of bias graph (RCTs)
Fig. 3
Risk of bias summary (RCTs)
Obtaining an objective evaluation of the endpoint was impossible due to the absence of activity comparison in the single-arm studies. In two of the included studies [22, 29], follow-up was less than 1 year, and in another [29], it was only 24 weeks. Furthermore, 12 out of 115 (10.4%) subjects were lost to follow-up in one study [13], and 3 out of 53 (5.6%) were lost to follow-up in another study [25]. The sample size was less than 100 in 6 studies [2, 22, 23, 25, 27, 28]. Regardless, it is acceptable to evaluate items that clearly state the purpose of the research, consistency of the results, methods for the collection of expected data, appropriateness of endpoint indicators to reflect the purpose of the study, and objectivity of the endpoint evaluation. As shown in Table 2, the quality of clinical trials ranged from moderate to high.
Table 2 Assessment of study quality (single-arm studies)Funnel plots were used to assess the potential publication bias in the reporting of remission maintenance (Fig. S2). The pooled results showed no evidence of a significant publication bias. Additionally, the Egger test was performed to evaluate the publication bias in the reporting remission maintenance. We obtained P = 0.633, which corroborated no significant publication bias (Fig. S3).
Outcomes of interestThe detailed outcomes of each study are presented in Table 3. The calculation of the pooled weighted proportions indicated that 59% (95% CI 25–61%) of the participants achieved induction of remission, 60% (95% CI 6–35%) achieved induction of response, 57% (95% CI 55–79%) achieved maintenance of remission, and 63% (95% CI 30–87%) achieved maintenance of response (Figs. 4, 5, 6, 7).
Table 3 The detailed outcomes at the end of treatmentFig. 4
Forest plot of induction of remission
Fig. 5
Forest plot of induction of response
Fig. 6
Forest plot of maintenance of remission
Fig. 7
Forest plot of maintenance of response
The most frequently reported adverse event was infection. A total of 134 (15.1%) patients developed infections. Furthermore, injection-related reactions were reported in 39 patients (4.4%) and 45 (5%) SAEs occurred in 885 patients. The most frequently reported SAEs were serious infections (30 patients); other SAEs included a meningitis secondary to a sinusitis (1 patients), pancreatitis (1 patients), severe neurological symptoms (3 patients), severe psoriasis (5 patients), and severe vasculitis (3 patients). Furthermore, two deaths were reported in one study. Other common adverse effects included neurological symptoms, neutropenia, vasculitis, and allergic and psoriasiform skin lesions.
Sensitivity and subgroup analysisThe calculation of the pooled weighted proportions indicated high heterogeneity among studies. Thus, further sensitivity and subgroup analyses were conducted to investigate important confounding factors (sensitivity analysis, see Fig. S4). The results of the subgroup analysis according to the baseline PCDAI score, study design, prior IFX exposure, and maintenance dose are presented in Fig. S5.
Induction of remissionIn the sensitivity analysis of remission induction, excluding any single arm did not significantly alter the heterogeneity among the studies. The subgroup analysis results also suggested that the proportion of patients with remission induction was significantly higher in children with PCDAI < 30 at baseline than in those with ≥ 30 (0.76 [0. 57–0.95] vs. 0.34 [0.20–0.49]). Furthermore, subgroup analysis in terms of whether the patients had previously received IFX treatment revealed no significant difference between the subgroup of IFX-exposed patients and the subgroup of some subjects without prior IFX treatment (0.38 [0. 24–0.52] vs. 0.45 [0.17–0.74]). However, ADA was significantly effective in the subgroup of IFX-naïve patients (0.94 [0.90–0.98]), suggesting a possible risk of bias.
Maintenance of remissionIn the sensitivity analysis of remission maintenance, we noted that excluding any single study did not significantly change the heterogeneity among the studies. Subgroup analysis further revealed that children with PCDAI < 30 at baseline showed a significantly higher proportion of maintenance of remission than those with score ≥ 30 (0.69 [0. 59–0.80] vs. 0.39 [0.24–0.54]). Additionally, whether the patients were from non-RCTs or RCTs resulted in no significant difference in the subgroup analysis results (0.61 [0.53–0.70] vs. 0.52 [0.24–0.80]). Moreover, there was no significant difference in the proportion of patients in the 40 mg doses cohort and ≥ 40 mg arm (0.58 [0.42–0.74] vs. 0.65 [0.46–0.85]); however, the < 40 mg arm achieved a lower proportion of maintenance remission 0.34 (0.25–0.44). Our results also indicated no significant difference between the subgroup in which all patients experienced IFX failure and the subgroup in which some patients experienced IFX failure (0.66 [0. 42–0.91] vs. 0.46 [0.29–0.63]). However, ADA was significantly more effective in the subgroup with IFX-naïve patients (0.75 [0.65–0.86]).
Maintenance of responseIn the sensitivity analysis, excluding any single study did not significantly alter the heterogeneity among the studies. Additionally subgroup analysis revealed no significant difference between the two cohorts with PCDAI scores > 30 and < 30 at baseline (0.61 [0. 31–0.91] vs. 0.68 [0. 0.57–0.78]). We also noted that the rate of maintenance response was greater in non-RCTs than RCTs (0.72 [0.56–0.88] vs. 0.35 [0.22–0.48]). In the ADA dose subgroup analysis, we noted that the response rate increased in a dose-dependent manner (0.42 [0.32–0.52] vs. 0.57 [0.35–0.78] vs. 0.91 [0.80–1.03]) for < 40, 40, and ≥ 40 mg, respectively). There was no significant difference between the subgroup in which some patients experienced IFX failure and the subgroup in which all patients prior to IFX treatment (0.63 [0.37–0.88] vs. 0.52 [0.24–0.79]). However, ADA was significantly more effective in the IFX-naïve subgroup (0.84 [0.72–0.97]).
留言 (0)