
記住我

Medication-related harm is a leading cause of avoidable healthcare harm.1 In England, it is estimated that adverse drug events (ADEs) contribute to or cause almost 2000 deaths per year and cost in excess of £180 m ($225 m) per year.2 The incidence of ADEs in hospitalized children and young people is estimated to be 3 times higher than that seen in adults.3 The extent of avoidable harm associated with medicines for children is estimated between 1% and 2% of patients.4 In the United Kingdom, adverse drug reactions are common, affecting up to 1 in 4 patients admitted to hospital.5 Children are vulnerable to drug-related problems in hospital. Thirty-five percent of patients are affected by drug-related problems while in hospital, with dosing and formulation issues being most prevalent.6 Many interventions have been proposed to mitigate these ADEs, but their effectiveness has been limited.7 Complex technological interventions such as computerized physician order entry and “smart” infusion systems are advocated to reduce ADEs but neither have demonstrated a clinically meaningful reduction in harmful ADEs.8,9 Only those studies where bundles of interventions were tested produced significant reductions in the incidence of prescribing errors.10 In a systematic review of interventions to reduce prescribing errors, 80% (56/70) of interventions were administrative controls—designed to influence human behavior, for example, implementation of guidelines and policies, and only those interventions involving expert consultation involving clinical pharmacists generated statistically significant improvements. Harm was not evaluated and has not been studied clearly in the pediatric population.11
Health care has been described as a complex, dynamic, adaptive system.12 Within a rapidly changing situation, multiple components interact in unpredictable ways. These responses require rapid changes in plan. Cause-and-effect analyses (e.g., root cause analysis)13 of ADEs lead to “…simple explanations for complex events.”14 Wong et al15 (2009) reviewed the literature of pediatric medication errors and identified several target interventions around education and training, electronic prescribing and clinical pharmacy services. However, these interventions were based on supposition from epidemiological studies and there was no robust insight into systems-based contributory factors. This is a weakness that runs through epidemiological and interventional studies to reduce pediatric medication errors, with very few theoretical studies exploring causation of these events.16 Subsequently, there is a need to understand how components within a system interact to identify potentially modifiable factors to further minimize ADEs for hospitalized children and young people.17
There are many methods for representing complex systems and their interactions. Predictive models such as failure mode and effect analysis decompose tasks into their component actions, to understand the causes and consequences of failure.18 These methods have been used to explore medication errors in neonatal and pediatric units.19–21 However, linear methods are vulnerable to outcome and operator bias, which undermines their utility in large-scale complex systems.22 In addition, such linear processes seek only to understand one part of a larger system and have limited application to system design.23
Given the complexity of healthcare systems and the ubiquity of medication within them, a whole-system perspective is needed. To facilitate this, there is a need to use multiple methods to represent the system and identify the contributory factors to negative outcomes therein. Leveson24 defines constraints as those elements of the system that enable it to function—the “laws of behavior.” Furthermore, Vicente25 posited that these constraints can also introduce restrictions on action which result in unexpected (or “emerging”) conditions and result in unexpected outcomes. It is thus possible to decompose these constraints and conditions into a “work domain” to present the system in its static state, without the impact of operators or events.26 It is therefore useful to represent the medication system to identify the objectives of the system and how they are intended to be achieved, to identify potential contributory factors to adverse events. This is an approach that has a long history in healthcare human factors and in the UK setting has been used in elderly care homes and in the exploration of medication safety incidents in community pharmacies.27–29
This study aimed to explore the sociotechnical system surrounding medicines management in pediatric inpatient settings, using work domain analysis (WDA)25 to describe potential gaps that may compromise medication safety for children and young people.
METHODSThis study was part of a larger qualitative study exploring medication safety processes in three acute children’s healthcare services in the north of England. The study was conducted between October 2020 and May 2022 and was approved by the Health Research Authority Leeds West Research Ethics Committee (19-YH-0430). Sites were selected using a maximal variation purposive sampling strategy based on their characteristics:
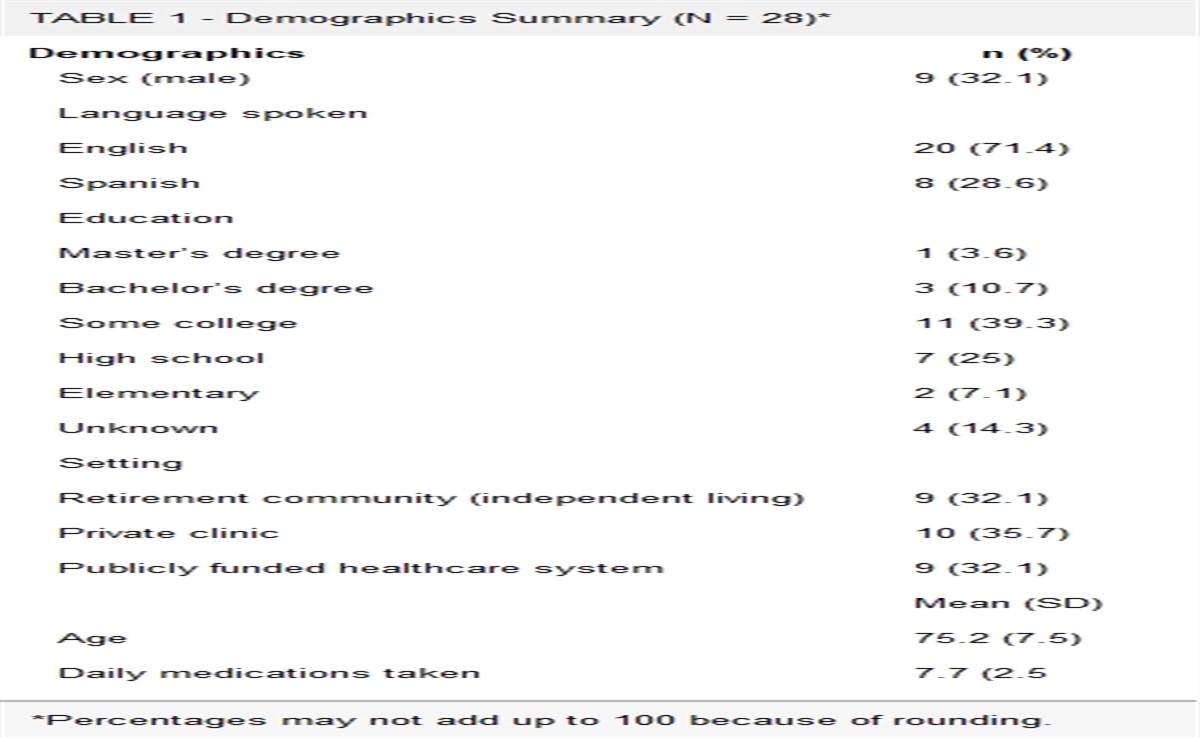
Diversity of organizations from an independent children’s hospital to a tertiary children’s hospital as part of a larger multispeciality hospital group, to a small district general hospital. Relative population diversity (social, cultural, and economic) and; Geographical relationship with other study centers. For example, the 2 children’s hospitals were selected to be geographically remote from each other to isolate the effect of cultural mixing, while the district general hospital was selected for the number of tertiary centers it had referral arrangements with to capture as broad a range of practice influences as possible.The characteristics of each site are presented in Table 1 hereinafter. The WDA was undertaken using document analysis (DA) and ethnographic observation at each site
TABLE 1 - Characteristics, Location, and Size of Study Sites Location Hospital Unit Size GH1 A small town in the northwest of England; pop 55,000. District general (245 beds) neonatal unit closed before initiation. 12 beds, and a 6-bed assessment area. CH1 A postindustrial city on the northwest coast of England; pop. 500,000 Standalone tertiary children’s (270 beds).Documents were selected in collaboration with local site collaborators (K.W., A.G., and S.M.), using agreed inclusion criteria: that they were policy or procedural documents relevant to medication processes; that they had evidence of organizational approval; and were within their expiry date. These documents included the medicines policies, medication errors policy, incident reporting policies, medicines management committee terms of reference, and other general medication-related policies. Between 15 and 20 documents were included from each site. Documents were analyzed by the lead researcher (A.S.) and a chartered ergonomist (D.P.) deductively using the following 5 levels of WDA as described by Naikar30 and the CWA prompts from Read and Salmon23: functional purposes, values and priority measures, purpose-related functions, object-related processes, and physical objects. An initial draft WDA was created using the CWA Tool v0.9.31 This was then reviewed and amended iteratively by 3 subject matter experts (SMEs) at each site (including a pharmacist, a nurse, and a pediatrician) for accuracy and completeness. The final WDA was agreed when no more changes were suggested by the SMEs.
Ethnographic ObservationsObservations of medication processes (prescribing, dispensing, administration, monitoring) were undertaken by the lead researcher (A.S.) as an open observer, independent of clinical care provision. He was not employed by any of the participating organizations, and his status as a pharmacist was only shared with participants in the field if asked. Ward staff were made aware of the presence of a researcher studying medicines safety with posters and short communications in the week before arrival. Furthermore, he wore clinical attire matching those of other members of staff. The total-observer posture was taken,32 making no interventions or suggestions, and he maintained an innocuous position in the ward permitting view of work. He was open about his purpose with all staff but careful to stress that there was no evaluation or judgment of their individual work or practice. Observations were structured around medication processes, and the work of a nurse, a pharmacist, and a physician was observed in each site. A convenience approach was used with activities and interactions observed as and when they occurred (hence the relatively prolonged observation period.) The timing of these observation sessions was predefined with site gatekeepers with the intention of capturing as much routine medicines work as possible. Contextual enquiry was used to clarify observation and interpretation.33
For the WDA, observation sessions were carried out over a 5-day period in each site, for no more than 4 hours per day. To facilitate observer entry, a 1-week non-observation period took place at each site immediately before the first observation period, during which the observer became embedded in the clinical area. No personal or protected data were collected through this study; therefore, a pragmatic consent process in line with British Psychological Society guidelines was used to minimize burden on participants.34 Participants (staff, patients, and their carers) provided verbal consent to observation, which was verified regularly. All field notes were written in gender neutral language, and no identifying details research sites were included. Field notes were kept electronically on a secure tablet device and were typed up into a detailed narrative shortly after each visit. Once field notes were typed up, they were destroyed. Only the observer had access to the detailed observation notes, but these were shared with members of the research team for analysis.
Data AnalysisObservations were analyzed deductively by the lead observer, to relate observed events and issues to contributory factors within the system that could be derived from the WDA. Data from observations were encoded to the WDA taxonomy proposed by Read et al.23 A data dictionary was also created to support the population of the different levels of the WDA. To support reflexivity, the researcher maintained a diary of thoughts and questions and underwent regular debriefing with members of the research team. Overviews of the data were also shared and discussed with site research teams at regular intervals to provide participant validation of the WDA.
RESULTSData from 2 observation periods (60 hours) over 3 months in each site were included in the WDA. The activity during one night shift, and 2 weekend days were observed. A total of 72 documents were also analyzed. The final abstraction hierarchy is presented in Figures 1 and 2 and the abstraction-decomposition space in Table 2. The data dictionary is presented in Supplementary File 1, https://links.lww.com/JPS/A573, to define the terms and identify the objects and artifacts that make up each element.
 FIGURE 1:
FIGURE 1: Abstraction hierarchy. Lines connecting component represent “means-ends” links.
 FIGURE 2:
FIGURE 2: Lower 2 domains of the abstraction hierarchy allowing clear view of the “means-ends” links between objects and processes.
TABLE 2 - Abstraction-Decomposition Space Organization Ward (Including Nursing Staff and Parents Medical Team Pharmacy Dept. Functional purpose Safe, secure, and efficient use of medicines Patient-centered use of medicines Values and priority measures Length of stay Adherence to policies, guidelines, and standards Incident occurrence Cost efficiency Purpose-related functions Clinical governance Administration of medicines to patients Prescribing medicines for patients Cost/budget monitoring Monitoring of medication effects Object-related processes Reviewing and updating reference sources Monitoring Staff planning Shift handover Care scheduling Consultation and review Obtaining medicines Obtaining medicines Verification Verification Medicines reconciliation Quality assurance Quality assurance Physical objects Computer terminals Prescriptions Incident reports Clinical staff Patients, parents, and carers Pharmacy staff Guidelines and policies Other reference sources Patient’s own medicines Patient’s own medicines Ward supplied medicines Ward supplied medicines Staff rosters Keys Keys Storage solutions Storage solutions Administration equipmentCells filled in gray do not apply to this level of abstraction.
Both the contents of the source documents and SMEs agreed that there were 2 overarching purposes of the systems: patient-centered use of medicines, and the safe, secure, and efficient use of medicines.
Values and Priority MeasuresDocumentary analysis suggested seven methods of monitoring the overall functioning of the system classified into three groups—service delivery, professional integrity, and patient outcomes. However, discussion with SMEs identified that these were more appropriately labeled according to monitoring parameters used by the organizations; thus, “incident occurrence,” “adherence to policies and guidelines,” “cost efficiency,” and “length of stay” appear in the second level of the WDA.
Purpose-Related FunctionsSix purpose-related functions were identified from both the documents and SMEs. “Clinical governance” included the routine assessment of performance of the work system using audit and spontaneous reports (incidents and complaints). “Cost and budget monitoring” encapsulated the mechanisms of the organizations to contain costs associated with medicines. There are then 4 separate headings relating to the clinical use of medicines related to the process described by Sutherland et al5—prescribing, administration, supply, and monitoring of medicines for patients. These are presented in the third level of the WDA.
Object-Related ProcessesEleven elements were identified as object-related processes (Table 3).
TABLE 3 - Summary of Object -Related Processes and Their Characteristics Reviewing and updating references sources The work required to maintain and ensure that medication references and procedures were up to date and reflected best practice. Monitoring Assessment of patient response to medicines but also the routine work to ensure compliance with local policy and procedure. Staff planning The process of skill mix determination through staff rosters. Care scheduling The processes required to plan the work to be done during a shift, including the allocation of patients to medical and nursing staff. Shift handover The process of passing on information about patients-of-concern and to identify actions that needed to be followed up during the shift. Medicines reconciliation The activities around obtaining and validating the medication history of each patient. Verification The physical process of checking to ensure that the medication prescribed is safe and appropriate for the patient and is undertaken by all members of the care team. Obtaining medicines The process involved in accessing medicines at ward level, from home and from the pharmacy department. Consultation and review The ongoing process of prescribing review and follow up during clinician, nursing and pharmacy rounds. Quality assurance The process of assessing the physical quality and utility of medicines and medicines information in the clinical area. Getting the medicine into the patient The processes involved in physically administering the medicine to a child under their care.The 14 objects identified in the system are summarized in Table 4 covering devices, people, and other resources.
TABLE 4 - Summary of Physical Objects and Their Characteristics Devices Computer terminalsWorking with SMEs in each site, the connections between elements at each level of the abstraction hierarchy were mapped. These means-ends connections supported the identification of dependencies of the functions of the system with the processes and objects within. For example, it would not be possible to administer medication (a purpose-related function) without access to appropriate information resources (an object-related process) and medication administration equipment (a physical object). We have also identified that although parents and caregivers are explicitly excluded from the system at the functional purposes level, it is challenging to administer medicines safely to children without them (Fig. 3).
 FIGURE 3:
FIGURE 3: Extract from the WDA showing means-ends relationships of parent/carer within the system.
Contributory FactorsThese means-ends links facilitated the visualization of processes and their constituent actions and resources. Thus we identified three potential systemic contributory factors to ADEs.
1) Resource limitations (inaccessible devices, materials, staff, and knowledge):It was noted during observations that some tools required to undertake tasks were often difficult to access. The keys to medication storage cupboards are emblematic to this, with frequently observed calls from nursing staff for the keys. Two sites had instituted technological interventions to improve access to medication—one site used an automated dispensing cabinet and another an audible tag that could be activated from the nurses’ station. However, these interventions were incomplete because there was still a need for physical keys for refrigerators and the controlled drugs cabinet. Keys, being physical artifacts, were sometimes broken or misplaced, which further added to the frustrations of staff seeking access to medicines.
Knowledge and expertise were also often accessible only to people who knew who to contact or where to look. Despite there being telephone systems and radio pagers in all sites, practitioners were dependent on personal cell phones and messaging platforms. Some participants spoke of “...phoning a friend…” when lacking experience or knowledge, while others demonstrated how official hospital contact lists were often out of date; thus, they relied on personal contacts and the recommendations of others.
Medication information was available on hospital computer systems, but many practitioners relied on their memory or that of those around them. “Pharmacy” would typically be contacted only as a last resort. It was often stated that information was impossible to find at the point of need and thus it was easier to just ask someone else. However, “pharmacy” was often poorly accessible at all sites, usually only by telephone or radio pager, and even then connected to a pharmacist who may not have been working in that ward on that day. Pharmacy services were highly dependent on wider service pressures within the pharmacy itself with ward cover reduced or removed on some days. Thus, the pharmacy service was not clearly a part of the ward ecosystem except in the context of medicine supply. In those sites with electronic prescribing, pharmacist activity was carried out in offices or remote areas of the ward. At times of staffing pressures, services could be provided remotely, which had been introduced as a new policy during the COVID-19 pandemic. Across all sites, pharmacy service provision was focused on the verification of prescriptions, ordering of medicines, and processing discharge orders.
2) Cognitive demands on the operators in the system:All participating wards in this study were acute admissions units, with high patient turnover. Nursing roster were all broadly comparable with a fixed ratio of staff to beds. During the study, one site decreased its nursing ratio from 1:4 to 1:6 to cope with high absence rates. This increased the workload on nursing staff resulting in them being unable to keep track of their patients in different areas of the ward, and missing information or tasks determined by medical teams.
Wards were busy and dynamic environments with multiple teams working on their own tasks and toward their own objectives and no team functioned together—medical, nursing, pharmacy, and parent groups were autonomous and independent. Medical staff were responsible for the vast majority of prescribing, and nursing staff operationally were responsible for administration and pharmacy services responsible for supply. Monitoring of medication effects was not allocated to any specific group of actors and was rooted in subjective clinical assessments of “improvement” in patient condition, to which all actors contributed. This led to distraction and interruption as members of teams reached out for additional information, advice, and opinion. Because of the disjointed goals and objectives of each team, these interruptions were inevitable because tasks could not be completed without them. Communication within teams was conducted in formal handover settings, but between team communication was transactional and informal.
Medication-related tasks were undertaken on an ad hoc basis according to when medicines were due. Nursing staff treated these individually prescribed medication times as fixed time points, and deviation was discouraged. In some sick patients, nursing staff would group tasks together. For example, a patient on frequent nebulizations would receive their treatment at the same time as observations and blood tests needed to be taken, to make their work more efficient.
Organizationally, all medicines administration had to be undertaken by registered staff (primarily nurses), or in 2 sites, parents could administer medication when assessed as competent to do so and under nursing supervision. This nursing-centric approach to medication administration created problems for families, particularly those on established medicine regimens. Some parents with children admitted to the wards reported that medicine doses were missed or delayed because they were prescribed at times that did not reflect the family schedule at home. However, some accepted that disruption was inevitable when their child came into hospital. Two of the 3 sites had parent self-medication policies, but in one site, this was an assessment involving mental capacity and psychiatric safety as well as the technical competency to administer medicines, which required the approval of a doctor, a nurse, and a pharmacist. Given the high patient turnover and the sensitivity of the information assessed, the policy was often unused. The other site used a more pragmatic approach asking parents to self-certify their competence to administer their child’s medicines and asking nurses to confirm that there were no safeguarding concerns.
“Because if the parents are doing it, it’s one thing less for me to worry about… they know what they’re doing because they do this every day at home.” Nurse, CH2
3) Adaptation and inadherence to safety critical processes:There was often suggestion that interventions to support medicines safety were ineffective because there was no underpinning consideration of how operators undertake their tasks in reality. This was evident through the way independent second checking of medicines administration was conducted. All sites had stated policies mandating the completion of these checks on administration. However, it was often the case that medicines were administered by parents in the absence of nurse supervision. Medicines were routinely “signed for” at the completion of preparation rather than on completion of administration. Nursing staff would routinely violate independent checking policies because the medications they were checking were either items that had been administered previously in the shift or were perceived as to not be dangerous or risky. Independent second checks required a second nurse to check prescribing, calculations, and manipulated volumes, which took time and were perceived to be of low value.
“Why am I going to spend all that time, doing all those checks on something that I’ve given two or three times in the last 2 days, that hasn’t changed…?” Nurse, CH1
All research sites had acknowledged the resource burden in mandating independent second checks and had introduced limited lists of “single check” items, where the product could be legitimately checked by a single nurse. However, these were often applied inconsistently and defined arbitrarily. In one site, only round doses of 5 mL of an oral liquid medication could be administered without a single check, while in another, the type of device used for a salbutamol inhaler determined whether the product required a second check.
One site had introduced an electronic barcode verification system to support a closed loop medicines administration system in an attempt to reduce medication errors. This involved linking orders in the Computerised Physician Order Entry (CPOE) system to barcodes on the product being administered. Barcodes on the product and on the patient’s wristband were scanned at the point of administration to ensure that the right drug was given to the right patient at the right time. This barcode system was consistently overridden, because nursing staff did not perceive it fitting with their routine tasks.
“We know we need to do these checks, but we just don’t have time and there are so many problems with it—wristbands, medicines from home, infection control…” Nurse, CH1
On the other hand, staff also admitted that they did not know why they were being asked to use it. There was a perception that it was being used as a management tool to monitor adherence to second checking policies. Furthermore, there were significant technical limitations to the system. Barcode devices were frequently inoperable or commandeered for other tasks such as scanning enteral feeds and default software updates initiating at inconvenient times. Furthermore, many medicines for children and young people did not have barcodes on the final vessel for the medicines, but they were on the outer packaging. These outer boxes were often discarded.
DISCUSSIONThis study has developed a representation of the complex medication safety systems in place for hospitalized children and young people. This representation has identified disconnection between organizational goals and values regarding medication safety, and the tasks and equipment needed to achieve those goals. It has also offered insights into elements of the system that might be amenable to intervention to improve safety that include a more flexible approach to medication double checking, the involvement of families in the medication administration process, and the optimization of the skill mix and workforce in the clinical area by reconsidering the role and function of pharmacy professionals.
Abebe et al35 undertook a similar study in a single pediatric ambulatory care program in the United States, focusing on the work of parent carers to keep medicines safe for their children. Their findings identified similar components to those in our findings, with cognitive elements and management of resources central to safe medication practice for children at home. Our study extends this topic by applying WDA to a multicenter exam of pediatric medicines management. Our study has also provided further insights into how medication errors may evolve because of the way processes are implemented and provide insight into why previous interventions may be less effective than expected in empirical study. Our study supports the position that the representation of a complex system is useful for subsequent systems design because of its theoretical foundations and the involvement of all within the system.36,37
System Reflections on Medication SafetyThe ability to deliver many of the functions and tasks is assumed to be the singular responsibility of the organization, but there is a reliance on external networks and parents for much information and expertise about the management of some medicines. Communication networks are informal and transactional, which may lead to failures of communication and decision making and lead to medication errors.38 We have identified that the professional groups in this system do not work together unlike that seen in high-performing areas such as emergency departments and maternity units where teams are allocated to the same environment.39,40 Thus, there may be an environmental aspect of medicines safety, which this representation of the safety system may not be able to identify. However, we have been able to identify a key role for families as a key resilience aspect of the safety system, yet at the higher levels of the system they are often excluded. This should be explored in more depth to consider how the work of parents can be safely acknowledged and supported, in the same way as the work of families in other care settings is being acknowledged and harnessed.41
All participating sites had ongoing campaigns to reduce interruptions in medication processes. Interruptions are associated with procedural and clinical errors but probably where communication is impaired.42,43 Therefore, we posit that the lack of effective teamwork in the acute pediatric ward is the systemic cause of these interruptions and distractions, which leads to degradation of system safety. We suggest that consideration be given to the structure and function of the wider care team in these settings, with a view to exploring how skill mix may improve safety outcomes. For example, there has been evidence that pharmacist participation in ward rounds may lead to reduced medication errors44–47 but the framework for this participation in the UK setting is unclear.48 All research into pharmacist impact on medication errors is through a lens of retrospective prescribing interventions rather than proactive clinical activity; thus, there are also economic and workforce considerations to acknowledge around staffing and outcome measures.
The adaptation or omission of safety processes in the name of task completion is not new in this field. Efficiency-thoroughness trade-offs are endemic throughout health care, and we have shown that efficiency-thoroughness trade-offs were imposed by organizational factors including workload, skill mix, and lack of resources.49,50 Our study has also shown that medicine safety work is reliant on human-based checks and a great deal of human resource is expended in these processes. However, the effectiveness of checks to prevent ADEs is disputed with mandated independent checks often violated, while spontaneous checks as a result of nursing uncertainty were associated with a reduction in medication error incidence and severity.42 Similarly in our observations, most of the medication administration checks observed were primed with only true independent checks for calculations or where a nurse actively sought a second opinion because they had doubts. However, nurses would state categorically that they “believed” that these checks were critical to administer medicines safety, yet they felt unable to adhere to them because of systemic limitations related to workload and overall system operability. There was a concerning culture in all sites toward reliance on the second check model to catch all errors, without considering the dynamic and distraction-rich environment, which in turn led to personal blame and guilt associated with medication errors.
Future Research ConsiderationsThis study has identified potential systemic interventions that warrant further exploration and development. After stakeholder consultation among participants in the larger study, the authors are agreed that these should be considered in order of priority laid out hereinafter.
1) There is a clear role for parents and carers in the system. Children (unlike adults) are admitted to hospital with advocates who are expected to competently make decisions about their child’s care but are not formally permitted to continue providing care to their child. While this study has not explored this phenomenon in great depth, it does demonstrate the importance of parents and carers as a source of resilience for the healthcare system. The concept of family-centered care is gaining increasing importance in neonatal care, but this has not translated into acute pediatric care.51 We recommend that additional exploration of the role and perceptions of parents around medicines safety for their children in hospital and consideration of the concerns and opportunities in healthcare services for involving them on a more equitable and formal basis be undertaken. 2) The use of independent second checks as the sole control against medication errors reaching patients. We recommend that alternatives to these weak administrative controls be considered and evaluated, including the following: Nurse-triggered checks for medicines that they lack familiarity with or have concerns about. Encouraging participation or inclusion of parents in the checking of medicines for their children while in hospital. Further consideration of the utility and effectiveness of barcode medication administration systems with reference to pediatric medicines and practice in UK hospitals as it is possible that the current evidence base is skewed toward U.S. service models.52 3) The role of pharmacy services in this system seems to be focused on supply processes—the verification of medication histories, prescriptions, and the ordering medication supplies. There is no apparent involvement of pharmacy teams in formal communication processes on the ward and the pharmacist as a safety mechanism seems to be retrospective and based in intervention. Pharmacists in the United Kingdom are unique in the global setting in that they have the opportunity to be independent prescribers and can develop more advanced skills and roles, which in this setting was not available or used.53,54 There is a still a physician-centric approach to medication-related problems. We propose further study of the role of the pharmacy professional in a more proactive setting, making use of the unique regulatory framework for pharmacists in the United Kingdom including prescribing and “advanced practice” elements. Strengths and LimitationsThis is the first multicenter observational study of medication safety in children’s inpatient services to focus on systems and processes, rather than ADEs as outcomes. The use of sustained observation ensured that rich, deep data were obtained. Where we differ from previous research is that we have presented a systematic representation of medicines management processes using robust methods that can be used by researchers and practitioners to potentially support onward service redesign, which no other study has presented in this field before. Furthermore, our multicenter design and careful selection of units in hospitals of differing sizes and organizational structure offer a degree of generalizability in our findings across the NHS that could not be offered from single-center qualitative or quantitative studies. Our inclusion of the wider healthcare team in the analysis and validation of these findings also provides some assurance of the veracity of our findings.
An important limitation is that this study used a single observer across all 3 sites. The observer is an experienced pharmacist with knowledge of medicines safety processes, and it is difficult to control for their own subjectivity in the analysis. However, parental and professional perspectives were included in the analysis, and local subject matter experts validated the WDA. The generalizability of our findings outside of the NHS in England may be limited because of the English focus of our study. No internal comparison between sites was undertaken, but the data could be reanalyzed as a comparative study and will be deposited in a suitable repository.
Finally, we must acknowledge that the SARS-nCoV2 pandemic may have influenced some of the observed findings, particularly around service provision and accessibility to some professional services, and the way families were nursed and occupied in the ward environment. Now that all pandemic restrictions have been removed, it is still the case that most patients in children’s services are isolated, social distancing of patients is still in operation and restrictions on ward round sizes and access to patient spaces continue to be in place.
CONCLUSIONSMany interventions in the system intended to support medicines safety are poorly designed around existing processes. Furthermore, the exclusion of families and other caregivers from the system may contribute to medication-related problems, but this requires further investigation.
We have identified a complex adaptive system where the demands of the organization conflict with the work that needs to be done. Our analysis has identified important systemic contributory factors for ADEs. Pharmacy professionals and families are important parts of the system, but their input is limited. Controls against ADE in clinical areas are checks of information retrieval and entry, and of medication administration. A lack of team working creates an interruption rich environment. Control processes are vulnerable to interruption and resource limitations. Furthermore, the way information and equipment for medication processes is presented predisposes the system to workarounds and the evolution of informal networks.
Interventions that include families and patients at their core, further research into the utility and benefit of medication administration checks, and the study of adapting the skill mix in the ward environment to make better use of the skills and knowledge of the wider healthcare team.
ACKNOWLEDGMENTSThe authors thank the medical, nursing, and pharmacy staff and families and patients who welcomed the researcher into their wards during the COVID-19 pandemic and all the work that involved. Specifically, the authors thank Dr Kirsten Wolfssohn, Natalie Keenan, Gaby Seddon, and Catherine Bell for facilitating the observer’s entry into their wards and for supporting data collection and validation of the WDA.
REFERENCES 1. Panagioti M, Khan K, Keers RN, et al. Prevalence, severity, and nature of preventable patient harm across medical care settings: systematic review and meta-analysis. BMJ. 2019;366:l4185. 2. Elliott RA, Camacho E, Jankovic D, et al. Economic analysis of the prevalence and clinical and economic burden of medication error in England. BMJ Qual Saf. 2021;30:96–105. 3. Kaushal R, Bates DW, Landrigan C, et al. Medication errors and adverse drug events in pediatric inpatients. JAMA. 2001;285:2114–2120. 4. Hodkinson A, Tyler N, Ashcroft DM, et al. Preventable medication harm across health care settings: a systematic review and meta-analysis. BMC Med. 2020;18:313. 5. Sutherland A, Phipps DL, Tomlin S, et al. Mapping the prevalence and nature of drug related problems among hospitalised children in the United Kingdom: a systematic review. BMC Pediatr. 2019;19:486. 6. Rashed AN, Neubert A, Tomlin S, et al. Epidemiology and potential associated risk factors of drug-related problems in hospitalised children in the United Kingdom and Saudi Arabia. Eur J Clin Pharmacol. 2012;68:1657–1666. 7. Maaskant JM, Vermeulen H, Apampa B, et al. Interventions for reducing medication errors in children in hospital. Cochrane Database Syst Rev. 2015;CD006208. 8. van Rosse F, Maat B, Rademaker CM, et al. The effect of computerized physician order entry on medication prescription errors and clinical outcome in pediatric and intensive care: a systematic review. Pediatrics. 2009;123:1184–1190.
留言 (0)