
記住我

Huge efforts to improve patient safety have been made worldwide since the Institute of Medicine estimated that 44,000–98,000 patients die every year in the United States as a result of medical error in 19991; however, adverse events (AEs) are still a leading cause of death and injury, and a recent report estimated that a medical error could be the third leading cause of death in the United States.2 Children are generally vulnerable to AEs and preventable AEs, yet such events have received relatively few evaluations in children compared with in adults. Children differ from adults in many ways with regard to medical care because of their unique safety issues, including requiring weight-based medication dosing especially when they are young, their inability to adequately communicate their complaints, and their physical and developmental characteristics.3,4 Previous reports of adverse drug events (ADEs) have showed high incidence rates of ADEs in pediatric settings.5 Although limited data exist in children, previous reports estimated that AEs of morbidity and mortality for pediatric inpatients account for more than 4400 deaths per year,6 and the rates of AEs have not improved.7 Such data are mostly from Western countries, and reports of their epidemiology, especially outside Western countries, are scarce. These results should not be extrapolated to other settings globally without basic data from other parts of the world.8 Thus, we conducted the Japan Adverse Events (JET) study, a dual-center, cohort study in several settings in Japan. The JET study in pediatrics was conducted in a historical cohort study fashion to investigate the incidence and nature of AEs in pediatric inpatients in Japan to improve pediatric patient safety.
METHODS Study Design and PatientsWe conducted this JET Study in the pediatric inpatient setting in 2 tertiary care teaching hospitals in Japan. One hospital was a children’s hospital (hospital A), and the other hospital (hospital B) cared for both adult and pediatric patients, with the pediatric units separated from adult units. Hospital A had an electronic medical record system with alert systems for prescriptions such as drug-drug interactions or duplicate prescriptions. Hospital B did not have an electronic medical record system, but it had a computerized order entry system for simple drug prescriptions, blood tests, and radiographs.
At hospital B, some pediatric patients were admitted to a regular intensive care unit (ICU), but most pediatric inpatients were admitted to general pediatric wards, neonatal ICUs (NICUs), or pediatric ICUs (PICUs). At both hospitals A and B, a few patients older than 18 years were also cared for by pediatricians and admitted to the pediatric wards. They generally had complex long-term medical conditions, such as congenital diseases (e.g., metabolic disease or cerebral palsy) or multiple disabilities. In this study, such patients older than 18 years were defined as overaged pediatric patients and patients who were 18 years old or younger were defined as pediatric patients.
The target population was pediatric inpatients who were discharged from any study wards at hospital A or hospital B during the 2 months of March and April of 2013 with a length of hospital stay between 24 hours and 12 months. Study wards consisted of 11 pediatric wards that included both internal medicine and surgical wards, 8 ICUs, which included general ICUs, PICUs, a high-care unit, growing care units, NICUs, and 8 psychiatric wards. In this study, patients who were hospitalized on psychiatric wards were excluded because their medical care and patients’ characteristics are considerably different from nonpsychiatric patients, and we decided to analyze their data separately. Thus, the remaining subjects excluding patients hospitalized on the psychiatric ward were stratified by wards, which were classified as surgical wards, internal medicine wards, and ICUs, and 60% of patients from each stratum were randomly selected as the study population. Because we determined that 1100 to 1200 patients would be necessary considering previous studies,5,9 as well as the feasibility of case reviewing, we decided to select 60% patients from each stratum to achieve that 1100 to 1200 patients would be included in this study.
The main units of evaluation were patient-days and number of admissions. The institutional review boards of the 2 participating hospitals and Hyogo Medical University approved the study. Because all data were obtained as part of routine daily practice, informed consent was substituted with opt-out methods according to the institutional review board requirements, and there were no refusals from the patients during the study period and thereafter.
DefinitionsThe primary outcome of the study was AEs, defined as an injury resulting from a medical intervention or an event resulting in unintended harm to the patient because of an act of commission or omission of medical care, rather than the underlying diseases or condition of the patient.10 For example, excess bleeding due to an operation or a hospital-acquired infection was considered an AE. Medical errors, defined as failure of a planned action to be completed as intended or use of a wrong plan to achieve an aim, were also identified.1 Errors also included failure of an unplanned action that should have been completed (omission).11 Some AEs are associated with a medical error and are considered preventable (preventable AEs), whereas some AEs are not associated with a medical error and are considered nonpreventable. Preventable AEs include ameliorable AEs that would be difficult to prevent, but the symptom of that AE could be ameliorated with appropriate care. An event with potential for harm due to a medical error but that did not result in injury was considered a potential AE. Medical care was categorized into the following 7 categories: drug, operation, exam and procedure (exam/procedure), judgment, nursing, rehabilitation, and management.
Data Collection and Review ProcessAccording to the standard methodology, we have developed training manuals with definitions of incidents such as AEs, errors, and potential AEs, description of the incidents’ identification process and examples of incidents.12 Reviewers were trained in advance in a standard manner using the manuals and were also trained by pilot reviewing using the actual practice data. The results of exercise and pilot reviewing were evaluated in terms of accuracy, and reviewers received the feedback.12–15 The trained reviewers consisted of a board-certified pediatrician and pediatric research nurses. Trained reviewers were based at each participating hospital and reviewed all medical charts and medical documents along with operation records, laboratory results, incident reports, safety reports, and prescription queries by pharmacists. They collected the characteristics and administrative data for all enrolled patients in the cohort. They then identified all potential incidents, such as AEs, potential AEs, and medical errors, as well as the details of the potential incidents. Data collected for potential incidents included the detailed settings of related medical care (i.e., the name of the operative procedure, the surgical site, operation time, the method of anesthesia, and its urgency if the related medical care was an operation) and the details of symptoms if the potential incidents were AEs, and the details of errors such as error stage, person in charge, and causes if the potential incidents were errors.
Independent physician reviewers, consisting of board-certified pediatricians, a board-certified primary care physician, and a board-certified intensivist, evaluated all potential incidents collected by the trained reviewers and classified them as AEs, potential AEs, medical errors, and exclusions. The physician reviewers rated AEs and potential AEs according to the severity of injuries or potential injuries to the patient using a 4-point scale, as well as their preventability using a 5-point scale. Categories of severity were fatal, life-threatening, serious, and significant. Fatal AEs resulted in death; life-threatening AEs caused such issues as transfers to ICUs or any other units for intensive care, or unplanned tracheal intubation; serious AEs included altered mental status, increased creatinine, or a decreased in blood pressure, and significant AEs included rash, diarrhea, or nausea, for example. Reviewers evaluated AEs as preventable or ameliorable if they were due to an error.
If a medical error was found, related medical care and the error stages in the process where it occurred were classified. The error stages were classified into judgment, order, preparation or dispensing, administration, equipment failure, or monitoring. When disagreement affected the classification of an incident, the physician reviewers reached consensus through discussion.
Statistical AnalysesContinuous variables are presented as medians with interquartile ranges (IQRs), and categorical variables are shown as numbers and percentages. Interrater reliabilities were calculated using κ statistics. The incidence per 1000 patient-days, the rates per 100 admissions, and the 95% confidence intervals (CIs) were calculated as a whole and by age category (neonates, infants, preschoolers, school-aged children, teenagers, or overaged pediatric patients). All analyses were carried out using JMP Pro 15.2.1 (SAS Institute, Inc, Cary, NC) software.
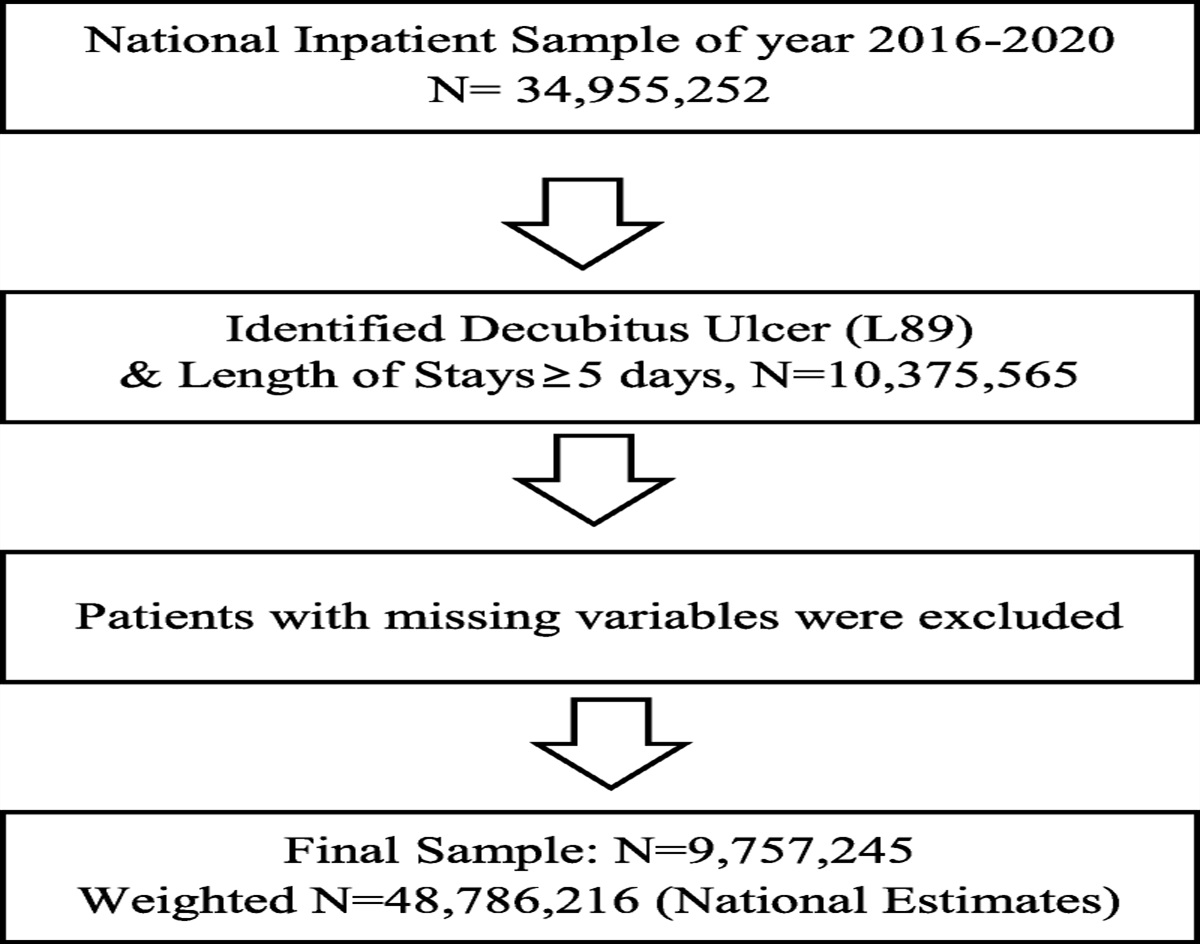
RESULTSWe included a total of 1126 patients with 12,624 patient-days on the study wards. The median age was 3 (IQR, 1–7) years, and preschoolers accounted for approximately half of all patients. Fifty-seven percent (639/1126) were male. The median hospital stay was 5 (IQR, 3–10) days (Table 1). One-third of the patients had an operation at least once during hospitalization, and 42% of patients had congenital malformations (Table 1). Physician reviewers had moderate to excellent agreement, with κ statistics of 0.55 for preventability to 0.98 for severity.
TABLE 1 - Patients’ Characteristics Patients (N = 1126) Male, n (%) 639 (57) Age, median (IQR), y 3 (1–7) Age category, n (%) 1. Neonates (<1 mo) 82 (7.3) 2. Infants (≥1 m, <1 y) 190 (17) 3. Preschoolers (≥1 y, <7 y) 545 (48) 4. School-aged children (≥7 y, <13 y) 202 (18) 5. Teenagers (≥13 y, <19 y) 87 (7.7) 6. Overaged pediatric patients (≥19 y) 20 (1.8) Genetic disorder, n (%) 188 (17) Congenital malformation, n (%) 469 (42) Allergy (drug), n (%) 66 (5.9) Allergy (food), n (%) 211 (19) Operation during hospitalization, n (%) 391 (35) Scheduled admission, n (%) 719 (64) Ward, n (%) 1. Pediatric general ward 976 (87) 2. NICU/GCU 82 (7.3) 3. ICU 68 (6.0) Division, n (%) 1. Internal medicine 597 (53) 2. Surgery 384 (34) 3. Neonatal intensive care 82 (7.3) 4. Intensive care 63 (5.6) Length of hospital stay, median (IQR), d 5 (3–10)The on-site trained reviewers identified 2699 potential incidents during the study period. Of these potential incidents, physician reviewers judged that there were 953 AEs in 412 patients (37%) (Fig. 1), for an incidence of 75.5 (95% CI [CI], 70.7–80.3) per 1000 patient-days, and a rate per 100 admissions of 84.6 (95% CI, 79.3–90.0). Of the 412 patients who had AEs, 105 (25%) had 3 or more AEs. The detailed examples of AEs are shown in Table 2.
 FIGURE 1:
FIGURE 1: Definitions of adverse events and medical errors.
TABLE 2 - Example Cases of Adverse Events in This Study Case Type of Adverse Event Category of Medical Care Severity Hypotension and fainting due to calcium blocker Nonpreventable Drug Serious Diarrhea during administration of antibiotics Nonpreventable Drug Significant Abrupt hypoxia (percutaneous oxygen saturation around 60%) due to the rupture of a balloon during balloon atrial septostomy Preventable Operation Life-threatening Arrhythmia after cardiac operation Nonpreventable Operation Significant Abrupt dyspnea due to unplanned extubation Preventable Exam/procedure Life-threatening Dyspnea due to sedation for magnetic resonance imaging Preventable Exam/procedure Serious Delayed diagnosis and treatment for hypotension due to anemia Preventable or ameliorable Judgment Life-threatening Neonate’s finger injury in neonatal intensive care unit when nurse shut the door of incubator Preventable Nursing Serious Pressure ulcer Preventable or ameliorable Nursing Significant Unplanned emergent operation for delayed diagnosis of intussusception Preventable Management Life-threatening Patient with acute lymphatic leukemia developed influenza during hospitalization for chemotherapy Preventable Management Life-threateningThe incidence of AEs was the highest in overaged pediatric patients and the lowest in neonates. The incidences in infants, preschoolers, school-aged children, and teenagers were relatively similar, but their incidence gradually decreased in the older age categories (Table 3). The patients who had congenital abnormalities were likely to have experiences of AEs during their hospitalization compared with patients who did not have congenital anomalies (49% versus 37%).
TABLE 3 - Adverse Events and Preventable AEs by Age Category No. Patients Total Patient Days AEs Preventable AEs Proportion of Preventable AEs (%) No. Events Incidence Rate* Rate† No. Events Incidence Rate* Rate† Total 1126 12,624 953 75.5 84.6 218 17.3 19.4 22.9 Age category 1. Neonates (<1 mo) 82 2798 127 45.4 154.9 50 17.9 61.0 39.4 2. Infants (≥1 mo, <1 y) 190 2049 183 89.3 96.3 42 20.5 22.1 23.0 3. Preschoolers (≥1 y, <7 y) 545 3840 321 83.6 58.9 77 20.1 14.1 24.0 4. School-aged children (≥7 y, <13 y) 202 2719 224 82.4 110.9 37 13.6 18.3 16.5 5. Teenagers (≥13 y, <19 y) 87 1066 80 75.0 92.0 7 6.6 8.0 8.8 6. Overaged pediatric patients (≥19 y) 20 152 18 118.4 90.0 5 32.9 25.0 27.8*Per 1000 patient-days.
†Per 100 admissions.
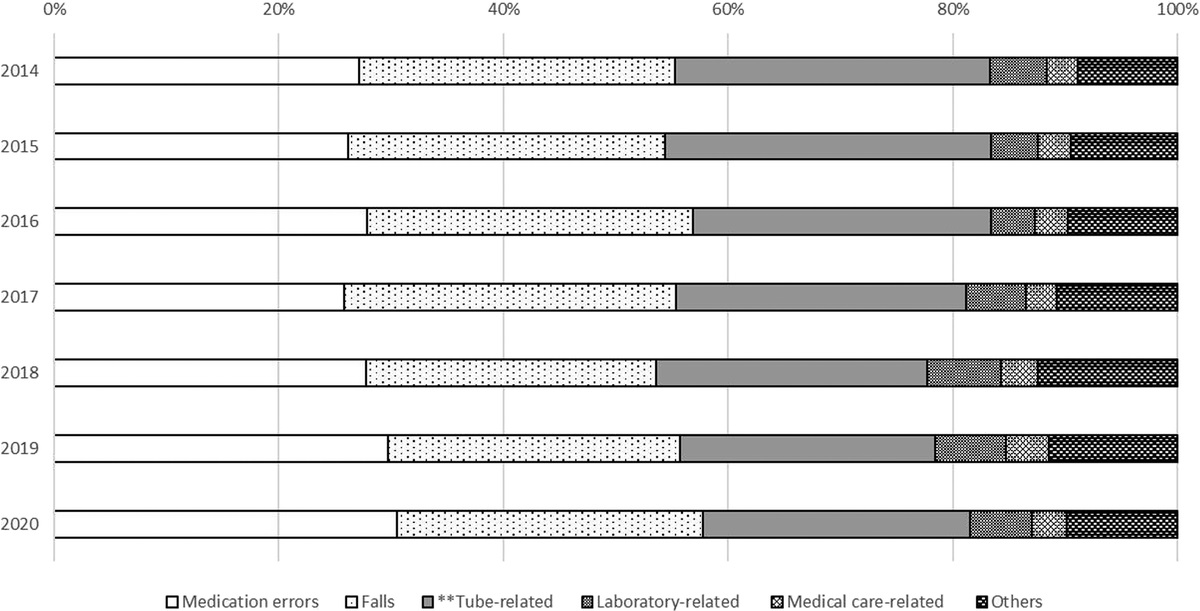
The category of medical care when AEs occurred also differed according to age category (Fig. 2). In neonates, nursing accounted for one-third of all AEs, and the proportion of nursing among all AEs in each age category decreased as age category increased. Judgment showed a similar tendency to nursing; judgment-related AEs only affected young children such as neonates, infants, and preschoolers, and no-judgment–related AEs affected older patients.
 FIGURE 2:
FIGURE 2: Distributions of adverse events by age category and category of medical care.
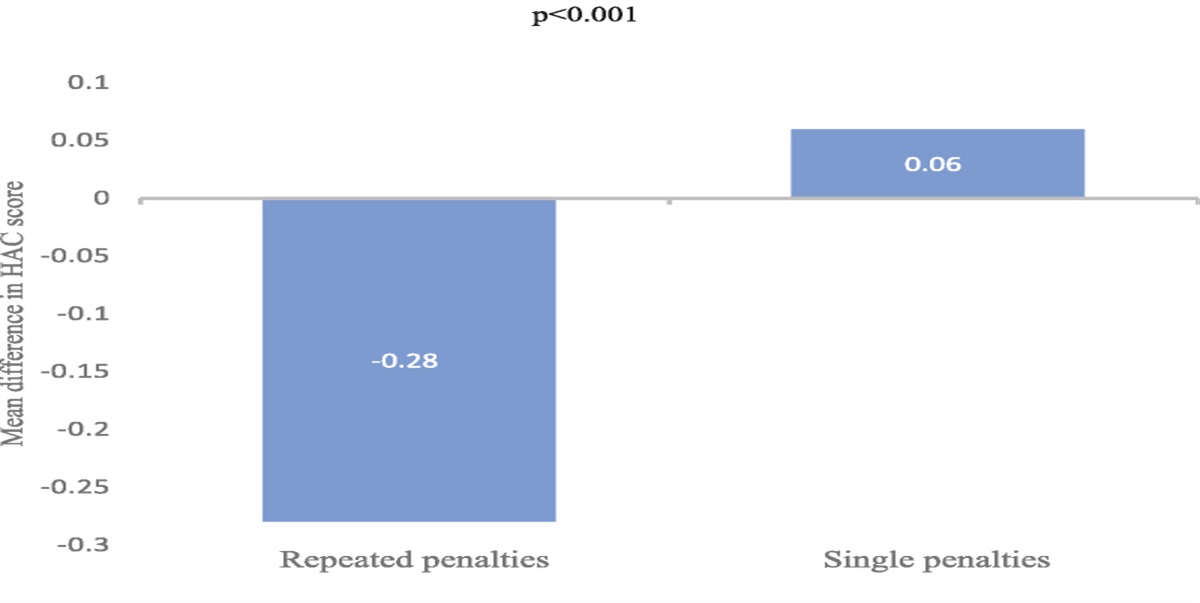
Of all AEs, the most frequent medical care was drug, at 34% (322/953) of all AEs, followed by operation (294, 31%), exam/procedures (169, 18%), and nursing (137, 14%) (Fig. 3). There were no medical care–related deaths. Life-threatening AEs accounted for 3.3% (31/953) of all AEs, and serious and significant AEs accounted for 25% (241/953) and 71% (681/953) of all AEs, respectively. Of the category of medical care, AEs related to judgment were life-threatening at a rate of 43% (3/7) and significant at a rate of 14% (1/7), which is more likely to result in severe AEs, whereas AEs related to nursing were less likely to result in severe AEs, and 90% (123/137) of them were significant.
 FIGURE 3:
FIGURE 3: The frequency of adverse events and preventable adverse events by category of medical care.
Medical Errors and Preventable AEsThe physician reviewers identified 865 medical errors affecting 433 patients (38%) (Fig. 1). Thus, the incidence was 68.5 (95% CI, 64.0–73.1) per 1000 patient-days, and the rate was 76.8 (95% CI, 71.7–81.9) per 100 admissions. Of the 433 patients affected by medical errors, 83 (19%) had 3 or more medical errors during their hospitalization.
Of the 865 medical errors, 218 (25%) resulted in AEs; thus, 23% of AEs (218/953) were considered preventable. The incidence rate of preventable AEs was 17.3 (95% CI, 15.0–19.6) per 1000 patient-days, and the rate per 100 admissions was 19.4 (95% CI, 16.8–21.9). In neonates, preventable AEs accounted for 39% of all AEs (50/127), the highest of all age categories. Then, the proportions of preventable AEs to AEs decreased with increasing age category (Table 3).
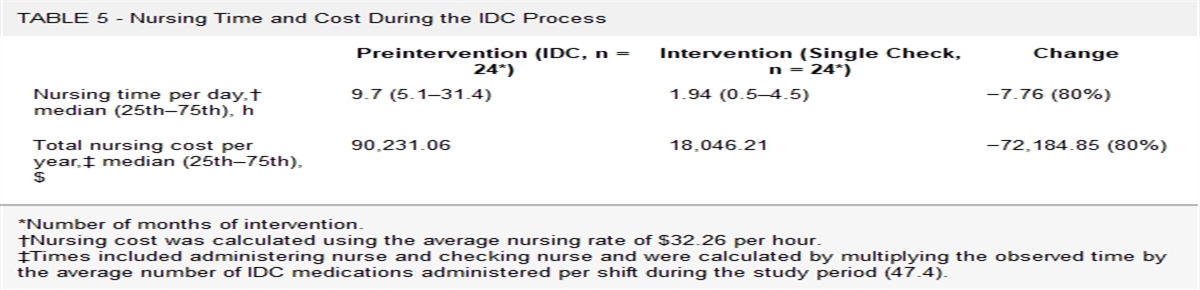
In terms of the category of medical care, AEs due to judgment or management were all related to medical errors, and AEs due to nursing were also highly related to medical errors (63%, 86/137), whereas nonpreventable AEs, which were not related to medical errors, accounted for approximately 90% of AEs in the category of drug and operation (Fig. 3). Of these 218 preventable AEs, 17 (8%) were classified as life-threatening while only 1.9% (14/735) were life-threatening in 735 nonpreventable AEs; thus, preventable AEs were more likely to become more severe compared with nonpreventable AEs. Specifically, preventable AEs related to exam/procedure or judgment resulted in life-threatening AEs at a higher rate (Fig. 4).
 FIGURE 4:
FIGURE 4: The severity of preventable adverse events and nonpreventable adverse events by category of medical care.
DISCUSSIONWe found that AEs were common in Japanese pediatric inpatients, with an incidence of 76 per 1000 patient-days, and 37% of pediatric inpatients had at least one AE during their hospitalization. In addition, the preventability and severity of AEs differed by age category and the category of medical care.
A critical step in reducing AEs in pediatric inpatients is to have the reliable and robust measurement of AEs. If such measurement is in place, it will be possible to evaluate their incidence over time and also to assess the effectiveness of efforts to improve pediatric patient safety. In adults, efforts to improve AE detection have accelerated with the adult-focused Institute Healthcare for Improvement Global Trigger Tool (IHI GTT).16 The IHI GTT has also been adapted for pediatrics; it has been tailored for NICUs and PICUs,17,18 the Pediatric All-Cause Harm Measurement Tool was modeled after the IHI GTT,19 and finally, the Global Assessment of Pediatric Patient Safety (GAPPS) Trigger Tool, which is the current standard trigger tool in pediatric inpatients, was developed building on multiple trigger tools.20 Through the development of these and other trigger tools, the methodology to detect AEs considerably improved, and medical record review using trigger tools proved far more sensitive and reliable than more traditional methodologies based on voluntary reporting systems or administrative screening tools.21
While the GAPPS Trigger Tool is a reliable measurement of AEs, it may not detect minor or rare AEs because in the process of its development, investigators removed triggers that indicated the presence of an AE infrequently to make it easier to use and decrease the time burden of review.20 In addition, the distribution of AEs by the category of medical care could not be analyzed using the GAPPS Trigger Tool, because each trigger had been already classified. In the present study, AEs were measured based on the manual review of all medical records, even though this was time and labor intensive. We chose this approach to have a comprehensive picture, including capture of infrequent and rare AEs that may not be captured by triggers. This also allowed AEs to be analyzed by the category of medical care, which is a strength of this study.
Several previous studies that have similarities have been done. For example, Kirkendall et al22 found high rates of AEs, with 76 AEs per 1000 patient-days by applying the IHI GTT to a pediatric inpatient population, and Stockwell et al23 reported 55 AEs per 1000 patient-days at 6 teaching hospitals by applying the Pediatric All-Cause Harm Measurement Tool. Although the incidence of AEs varied across the studies, the present findings are mostly consistent with these previous reports that used trigger tools. Stockwell et al7 further reported an incidence of 19.0 AEs per 1000 patient-days in pediatric inpatients by applying the GAPPS Trigger Tool. The present incidence was higher than this report because this relatively lower rate in the study applying the GAPPS Trigger Tool may be attributable to the methodology of the GAPPS Trigger Tool, which is more sophisticated and efficient, or to the study settings. Another possibility for higher incidence of AEs in this study could be related to the patients’ characteristics of study population. In this study, 42% of patients had any congenital malformation, and patients who had congenital anomalies were likely to have experiences of AEs during their hospitalization compared with patients who did not have congenital anomalies (49% versus 37%).
In the present study, the incidence of AEs tended to decrease with increasing age category, except for “overaged” children, who tend to be quite complex. The findings that younger children are more vulnerable to AEs could be related to unique pediatric safety issues, including particular attention in care attributable to changes in patient weight and physiological maturation and limited capacity for cooperation in young children.24 The distribution of AEs by category of medical care was also different by age category. In neonates, nursing-related AEs were the most frequent AEs and accounted for one-third of all AEs, whereas nursing accounted for only 5% of AEs in teens. In a previous report, Woods et al25 showed that the diagnostic-related AEs were higher in children than in nonelderly adults (defined as patients 21–65 y of age in their study), and they assumed that the specific characteristics in pediatric care, such as the more varied presentation of symptoms of illness and the greater difficulties in history taking and physical exam, could be related to it. Thus, it may be that some AEs are more age dependent because of children’s limited linguistic skills.26 The incidence of such AEs could be higher in younger patients, and we need to be aware of these findings to provide intensive monitoring for pediatric inpatients with such medical care in daily clinical practice.
Overall, the most frequent medical care that was related to AEs was drug use, which accounted for 34% of all AEs, and only 10% of these drug-related AEs were due to errors or preventable. The incidence of drug-related AEs is generally consistent with the previous report in Japan5 and is similar with the report by Kaushal et al9 showing that preventable ADEs were relatively infrequent. On the other hand, judgment and management-related AEs were all due to errors; thus, all were considered preventable AEs, and this suggests that the preventability also varied by the category of medical care. Although judgment and management-related AEs accounted for 0.7% and 2.5% of all AEs, respectively, a substantial number of AEs could be effectively reduced if the appropriate intervention to prevent such AEs could be developed.
This is the first report, to the best of our knowledge, to capture the effects of age and medical care on the distribution of AEs applying the standard methodology of chart review.12 Considering these findings and developing a strategy according to age category and the category of medical care could be the next steps to reduce the burden and impact of AEs in daily clinical practice.
The present study has several limitations. It may have underestimated the true rate of AEs, by its nature of record review-based methodologies, which are limited to information provided in the medical records; however, the approach used the rigorous standard method to detect AEs. The classification of AEs as preventable or nonpreventable was based on the professional judgment of the physician reviewers; although they were well trained and experienced, they might have been biased. Finally, the present findings may not be generalizable to all inpatients in other settings, because patients’ characteristics or systems of medical care vary across hospitals and countries.
CONCLUSIONSWe found that AEs were common in Japanese pediatric inpatients, and their preventability and severity varied considerably different by age category and the category of medical care. Further investigations should assess which strategies may be most effective for improving pediatric patient safety.
ACKNOWLEDGMENTSThe authors thank Ms Masako Tomotsune, Ms Toshiko Mizuno, Ms Yuki Obayashi, Ms Yukari Inose, Dr Takeo Iwamoto, Dr Kinu Takahashi, Dr Takashi Kawakubo, Ms Yukie Mishima, Ms Eriko Waki, Ms Yumiko Kimura, Ms Sayako Kakimi, Ms Hiroko Nukita, Ms Makiko Ohtorii, Ms Kaori Yamamoto, Mr Susumu Seki, Ms Ai Mizutani, Ms Yuka Iwamaoto, Ms Masami Wakisaka, Ms Namiko Ikeda, Ms Naomi Shimohara, Ms Mika Sakai, Ms Yuko Ueo, and Ms Lisa Yorogi for their assistance with this project.
REFERENCES 1. Institute of Medicine 2000. To Err is Human: Building a Safer Health System. Washington, DC: The National Academies Press doi: 10.17226/9728. 2. Makary MA, Daniel M. Medical error—the third leading cause of death in the US. BMJ. 2016;353:i2139. 3. Plint AC, Stang A, Newton AS, et al. Adverse events in the paediatric emergency department: a prospective cohort study. BMJ Qual Saf. 2021;30:216–227. 4. Walsh KE, Bundy DG, Landrigan CP. Preventing health care-associated harm in children. JAMA. 2014;311:1731–1732. 5. Sakuma M, Ida H, Nakamura T, et al. Adverse drug events and medication errors in Japanese paediatric inpatients: a retrospective cohort study. BMJ Qual Saf. 2014;23:830–837. 6. Halvorson EE, Thurtle DP, Kirkendall ES. Identifying pediatric patients at high risk for adverse events in the hospital. Hosp Pediatr. 2019;9:67–69. 7. Stockwell DC, Landrigan CP, Toomey SL, et al. Adverse events in hospitalized pediatric patients. Pediatrics. 2018;142:e20173360. 8. Morimoto T, Fukui T, Lee TH, et al. Application of U.S. guidelines in other countries: aspirin for the primary prevention of cardiovascular events in Japan. Am J Med. 2004;117:459–468. 9. Kaushal R, Bates DW, Landrigan C, et al. Medication errors and adverse drug events in pediatric inpatients. JAMA. 2001;285:2114–2120. 10. Steering Committee on Quality Improvement and Management and Committee on Hospital Care. Policy statement—principles of pediatric patient safety: reducing harm due to medical care. Pediatrics. 2011;127:1199–1210. 11. Institute of Medicine. Patient Safety: Achieving a New Standard for Care. Washington, DC: The National Academies Press. 2004. doi: 10.17226/10863. 12. Morimoto T, Gandhi TK, Seger AC, et al. Adverse drug events and medication errors: detection and classification methods. Qual Saf Health Care. 2004;13:306–314. 13. Leape LL, Brennan TA, Laird N, et al. The nature of adverse events in hospitalized patients. Results of the Harvard Medical Practice Study II. N Engl J Med. 1991;324:377–384. 14. Brennan TA, Leape LL, Laird NM, et al. Incidence of adverse events and negligence in hospitalized patients. Results of the Harvard Medical Practice Study I. N Engl J Med. 1991;324:370–376. 15. Hiatt HH, Barnes BA, Brennan TA, et al. A study of medical injury and medical malpractice. N Engl J Med. 1989;321:480–484. 16. Classen DC, Lloyd RC, Provost L, et al. Development and evaluation of the Institute for Healthcare Improvement Global Trigger Tool. J Patient Saf. 2008;4:169–177. 17. Sharek PJ, Horbar JD, Mason W, et al. Adverse events in the neonatal intensive care unit: development, testing, and findings of an NICU-focused trigger tool to identify harm in North American NICUs. Pediatrics. 2006;118:1332–1340. 18. Agarwal S, Classen D, Larsen G, et al. Prevalence of adverse events in pediatric intensive care units in the United States. Pediatr Crit Care Med. 2010;11:568–578. 19. Stockwell DC, Bisarya H, Classen DC, et al. Development of an electronic pediatric all-cause harm measurement tool using a modified Delphi method. J Patient Saf. 2016;12:180–189. 20. Landrigan CP, Stockwell D, Toomey SL, et al. Performance of the Global Assessment of Pediatric Patient Safety (GAPPS) Tool. Pediatrics. 2016;137:e20154076. 21. Classen DC, Resar R, Griffin F, et al. ‘Global trigger tool’ shows that adverse events in hospitals may be ten times greater than previously measured. Health Aff (Millwood). 2011;30:581–589. 22. Kirkendall ES, Kloppenborg E, Papp J, et al. Measuring adverse events and levels of harm in pediatric inpatients with the Global Trigger Tool. Pediatrics. 2012;130:e1206–e1214. 23. Stockwell DC, Bisarya H, Classen DC, et al. A trigger tool to detect harm in pediatric inpatient settings. Pediatrics. 2015;135:1036–1042. 24. Lannon CM, Coven BJ, Lane France F, et al. Principles of patient safety in pediatrics. Pediatrics. 2001;107:1473–1475. 25. Woods D, Thomas E, Holl J, et al. Adverse events and preventable adverse events in children. Pediatrics. 2005;115:155–160. 26. Takeuchi J, Sakuma M, Ohta Y, et al. Differences in adverse drug events and medication errors among pediatric inpatients aged J Patient Saf Risk Manag. 2021;26:261–266.
留言 (0)