Constipation is one of the most common chronic health problems reported in the pediatric population worldwide. By far, the most common etiology is functional constipation (FC), which affects more than 10% of children worldwide [17].
The Rome IV Criteria define FC in children (developmental age ≥ 4 years) in the presence of two or more of the following criteria, for at least 1 month: (1) two or fewer defecations per week in the toilet, (2) at least one episode of fecal incontinence per week, (3) retentive behavior, (4) painful or hard bowel movements, (5) detection of large fecal mass in the rectum, and (6) stools of large diameter that may obstruct the toilet. There are also well-defined and overall similar criteria for FC diagnosis in children (toilet-trained and non-toilet-trained) younger than 4 years of age [6].
FC implies a high pharmaceutical cost. Likewise, fecal impaction can lead to a situation that seriously compromises patient health, especially at extreme ages, causing sometimes a vital risk. In order to treat these pathologies, a variety of resources has been employed, including pharmaceutical resources and others that directly impinge upon patient life habits [20].
The most outstanding and frequently utilized resource is the use of laxatives. Laxatives are substances utilized since ancient times for different applications. Their main function is to provoke feces evacuation and/or bowel cleansing. Today, their use is indicated in different situations: including FC treatment non-responding to dietary hygienic measures [23].
PEG is a polymer that is not metabolized in the gastrointestinal tract and creates an osmotic gradient in the lumen of the colon, subsequently leading to fluid retention and hence softening and loosening of stools [1].
In the current study, we aimed to investigate the long-term efficacy of polyethylene glycol (PEG) as a maintenance treatment for functional constipation (FC) in children living in Egypt.
It is worthy to mention that both groups had received a disimpaction treatment before starting maintenance therapy, which was polyethylene glycol (PEG) in a dose of (1–1.5 g/kg for 3–6 days) in group 1 and one daily phosphate enema for 2 to 3 days for those in group 2.
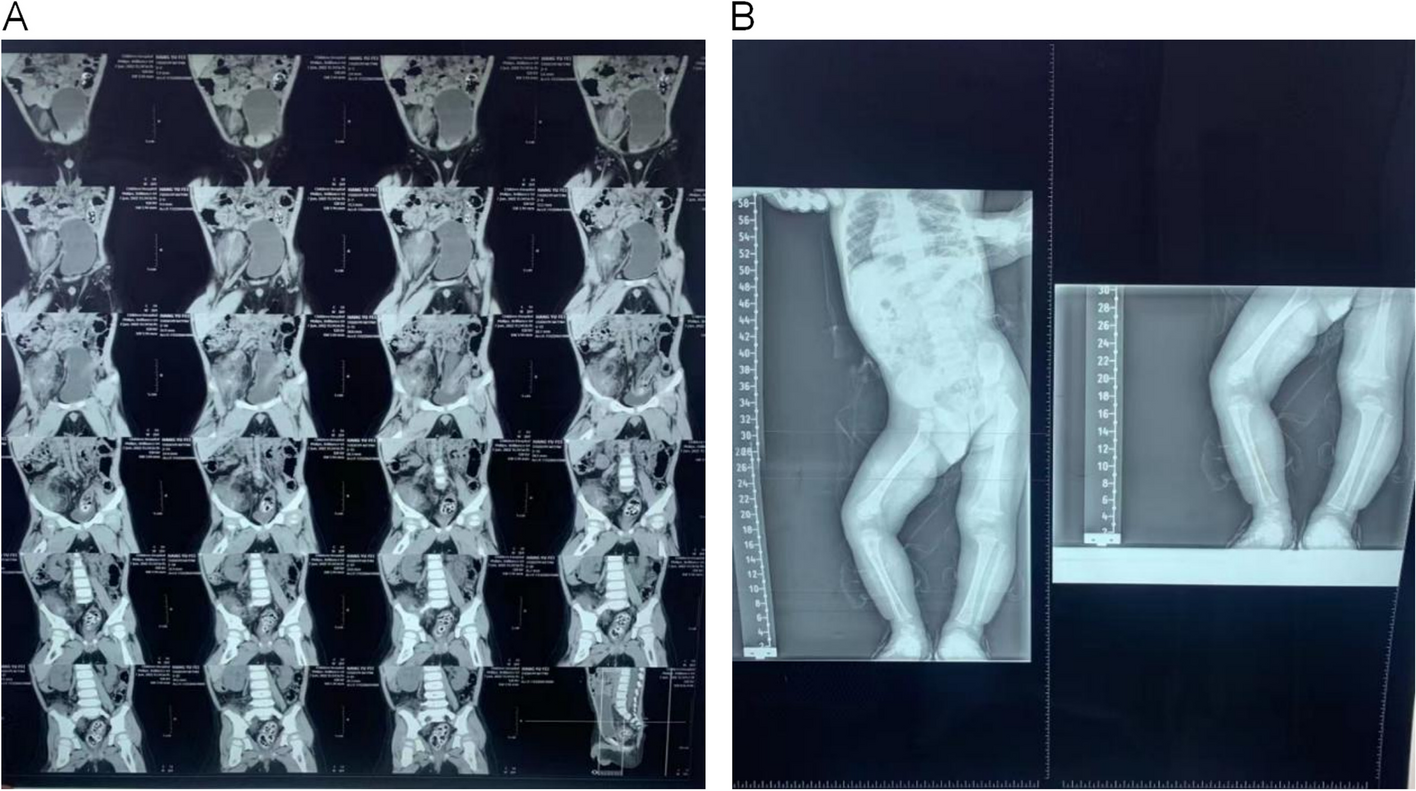
Disimpaction is confirmed by abdominal examination and a plain X-ray abdomen before starting maintenance therapy.
No statistically significant difference was found between both groups according to age, sex, duration of start complaining, and family history. However, females represented more than half of patients in group 1 and group 2 (55% and 67%, respectively).
These results were different from those in the study of Olaru and colleagues [25] where a higher prevalence was observed in males. Moreover, other studies reported a similar prevalence in boys and girls [21].
Many patients with FC have a positive family history of FC, suggesting that genetic factors may play a role. In our study, we found that family history was reported among (40–27%) for group 1 and group 2. This was consistent with the study of Olaru and colleagues [25] who reported a positive family history of functional constipation among 38.49%.
We found a statistically significant improvement after the treatment in both groups; regarding weight, z-score weight for age, height, z-score height for age, mid-arm circumference, and z-score mid-arm circumference for age as these variables were low before treatment.
This was in accordance with the study of Yousefi and colleague [34] as their study demonstrated that children with symptoms of functional constipation had much less average weight and height than children without constipation. z-scores of height and weight for age were considerably different in both groups. In other words, this study showed that functional constipation leads to significant impairment of growth, including children’s height and weight which is totally independent of the gender of the child.
The study of Chao and colleagues [5] showed the functional constipation of children as the cause of their growth retardation. In their study, a significant increase in z-scores of height and weight for age and body mass index for age was observed after 12 and 24 weeks of constipation treatment in children aged 1 to 15 years with constipation. These results were different from other studies that have shown a high prevalence of obesity in children with functional constipation.
This does not coincide with the study of Koppen and colleagues [15] that showed most of the children with constipation were obese or overweight. A similar study conducted on 100 Iranian children younger than 18 years old with functional constipation found a higher obesity rate and higher BMI and weight z-scores in constipated patients compared to the healthy control group [7].
This was in agreement with the study of Pawłowska and colleagues [26] which illustrated that pediatric patients with functional gastrointestinal disorders present with various growth abnormalities. They found that underweight was more frequent in children with functional constipation; also, short stature and stunting were common in patients with functional constipation.
There are various causes for delayed growth in children with constipation. Fecal impaction in these children may cause abdominal fullness and discomfort and nausea leading to decreased appetite and food aversion [34]. On the other hand, the psychological effects of functional constipation on children and their parents impact the child’s nutrition and growth, too. Many recent studies have emphasized the significant effects of constipation on children’s alimentary habits and on their developmental parameters, which can return to normal growth by treatment of anorexia or the elimination of organic causes associated with constipation [13].
After treatment, both groups showed a significant improvement regarding different parameters as in abdominal circumference, presence of fecal masses, and decrease in anal fissures or piles after treatment in group 1; however, in group 2, there was a significant improvement in abdominal circumference and abdominal fecal masses with a p-value < 0.05. There was a significant improvement in hemoglobin, hematocrit value, and serum iron after treatment in both groups which contributed to improving the appetite of those patients.
Regarding the Rome IV Criteria, there was a significant improvement in the number of defecation, number of fecal incontinence, history of retentive posturing or excessive volition stool retention, and history of pain or hard bowel movement after treatment in children more than 4 years old with a p-value < 0.001 in group 1, but in group 2, there was a statistically significant improvement in pain and hard bowel movement after treatment with a p-value 0.004.
By comparing both groups, a significant improvement was observed in fecal masses after treatment in group 1 with a p-value < 0.05; also, there was a significant improvement in the number of defecations regarding the Rome IV Criteria in children less than 4 years old with a p-value < 0.05 due to the effect of polyethylene glycol.
We found a statistically significant decrease in number of the patients who needed to continue treatment and patients who had impaction during treatment intake in group 1 than in group 2 with a p-value < 0.05. However, there is a statistically significant increase in the number of patients who complained of palatability in group 1 with a p-value of 0.000.
This was in accordance with our findings and the study of Voskuijl and colleagues [31] which analyzed PEG 3350 (n = 46) versus lactulose (n = 45) for an 8-week period in a double-blind, randomized clinical trial of parallel groups, constituted by children from 6 months to 15 years of age. Children younger than 6 years took 2.95 g/sachet/day of PEG or 6 g/sachet/day of lactulose and children older than 6 years took 5.9 g/day versus 12 g/day (2 sachets). The dose was increased by another 2.95 g of PEG or 6 g of lactulose if the effect was considered as insufficient, or it was reduced by 50% if diarrhea appeared. The percentage of success (number of patients presenting ≥ three stools per week and ≤ one episode of encopresis every 2 weeks) was higher in the group with PEG (56% versus 29%, p < 0.02) than in the group with lactulose, in both PEG doses. Moreover, in this group, an improvement in abdominal pain, effort, and pain during bowel movement regarding lactulose intake was also observed.
This was also in accordance with the study of Candy and colleagues [3] which analyzed the long-term (3 months) efficacy to avoid new impaction episodes and to increase the number of defecations/week after a fecal disimpaction treatment in 27 children (2–11 years old). In the lactulose group, 23% of patients suffered impaction, compared to 0% in the PEG-treated group (PGE + E) (p < 0.01), and the number of weekly stools was significantly higher in the PEG-treated group (9.4 versus 5.9, p = 0.007, 95% CI 1.0–6.0).
This was also in agreement with the study of Wang and colleagues [33] which evaluated the efficacy and safety of PEG 4000 in children (n = 105) (20 g/day, during 14 days) versus lactulose (n = 111) (10 g/day during three days and 6.7 g/day during 11 days) in a blind, randomized, and multi-center study. Clinical remission was considered when patients presented more than three stools per week, and their consistency had a 4–6 value on the Bristol Stool Scale. Moreover, 72.38% of patients treated with PEG achieved remission, compared to 41.44% of patients treated with lactulose; the average frequency of stools in the PEG-treated group increased from 2 to 7, with respect to a 2 to 6 increase in the lactulose-treated group, and stool consistency during the second week was better in the PEG-treated group.
Treepongkaruna et al. [29] compared PEG 4000 versus lactulose in 88 children of 1–3 years of age affected by FC during a period of 1 month in a randomized, double-blind study (8 g per day of PEG 4000 and 3.3 g of lactulose). The average change in the stool frequency/day in both groups was 0.51 stools/day in the PEG group, compared to 0.15 stools/day in the lactulose group. Furthermore, stool consistency and ease of stool passage were significantly better in the PEG-treated group.
In a recent randomized, multicenter study, Mathew and Bhatnagar [19] covered 12 weeks of treatment and 4 weeks of follow-up of patients with functional constipation. Patients were randomized (central randomization) to receive either PEG or lactulose. The primary end points were the number of defecations per week after 12 weeks of treatment and improvement in stool consistency of at least 2 points on the Bristol Scale. The secondary end point was the presence of adverse events. Bowel movements ≥ 3 per week and stool consistency ≥ 2 (Bristol Scale) were considered as successful treatment; at week 12, good clinical outcome was achieved in 98% (PEG) and 90% (lactulose). The PEG group had more defecations per week compared with the lactulose group (7.9 ± 0.6 vs 5.7 ± 0.5, p = 0.008), and both groups had similar frequency of defecation with pain (5% vs 5%, p = 0.9), stool retention (7% vs 10%, p = 057), large volume of stools (30% vs 31%, p = 0.9), and hard stools (7% vs 13%, p = 0.58). There were more patients with side effects in the lactulose group (15 vs 23, p = 0.02), mostly bloating and abdominal pain. The authors concluded that PEG 3350 is more effective and causes fewer side effects compared to lactulose in the treatment of constipation in infants and children [19].
In harmony with our findings, Gordon et al. [11] in the intervention review evaluated the efficacy and safety of osmotic and stimulant laxatives used to treat functional childhood constipation. The authors included in the analysis 6 studies comparing PEG and lactulose. The number of patients included ranged from 50 to 100 in different ages, between 6 months of age and 16 years old. A statistically significant difference in frequency of defecation in favor of PEG over lactulose was seen, with a mean difference of 0.70 stools per week (95% CI 0.10 to 1.31). Thirty-seven percent (46/123) of PEG patients experienced at least one adverse event compared to 45% (54/119) of lactulose patients (95% CI 0.68 to 1.11).
These results were different from the findings of Gremse and colleagues [12] which analyzed in an open, randomized, and crossover study the efficacy of PEG 3350 (10 g/m2/day) versus lactulose (1.3 g/kg/day in two intakes) in 37 children (2–16 years old) for 2 weeks, and subsequently, treatments were crossed over for another 2 weeks. In addition, the number and features of the stools, colonic transit time, and grade of satisfaction perceived by health care providers and physicians were evaluated. They did not observe significant differences between the treatment groups in any parameter analyzed.
The strength of the current study contributed to the type of study “randomized clinical trial,” and according to our knowledge, this study is the first one in Egypt to compare PEG and our classic treatment (lactulose or senna).





留言 (0)