
記住我



Coronavirus disease 2019 (COVID-19) infection may result in diverse symptoms, such as severe upper respiratory problems,1 fever, fatigue, shortness of breath, congestion, or nausea.2 In addition, COVID-19 symptoms may differ in severity among various populations including, but not limited to, those who have underlying medical conditions and older adults. Long COVID pertains to those individuals who experience symptoms for weeks or more following a COVID-19 infection.3 The symptoms result from multisystemic problems that may demonstrate relapsing-remitting presentations that persist over time. Symptoms of myalgia and skeletal muscle weakness have been present in individuals with COVID-19 infection and those with Long COVID.4–6 That is a concern, as muscle weakness is an impairment that may affect the capacity for performing activities (eg, locomotion or the ability to perform activities of daily living [ADL]) or participation (eg, engagement in employment or recreation). If muscle weakness is a sequela of COVID-19 infection it is important to identify the impairment so that health care providers can monitor for this impairment and develop intervention strategies.
Measurement of strength requires the participant's voluntary force output from muscles and measuring or quantifying that force.7 Examples include measures with hand-grip dynamometry (HGD), handheld dynamometry, field tests such as sit-to-stand testing and manual muscle testing (MMT).7,8
HGD testing is a widely used and clinically accepted method for measuring grip strength, which also has an abundance of available normative data.7 Test-retest reliability and interrater reliability of HGD is well established and is good to excellent with coefficients of more than 0.80. HGD also reports excellent concurrent validity.9
Handheld dynamometry is an appropriate measure based on excellent reliability and adequate to excellent validity across multiple populations and diagnoses. The presence of pain in the region being tested does not influence reliability.10 Interrater and intrarater reliability for handheld dynamometry is good to excellent with ICC values more than 0.75, interdevice reliability also demonstrated good to excellent results with the ICC values more than 0.75, and concurrent validity was shown to be good to excellent as well, with ICC values more than 0.75.11 Test-retest reliability has been demonstrated to be good to excellent.10
According to Bohannon and Crouch,8 the 1-minute sit-to-stand test (1-MSTST) has the capability to assess the ability to perform physical functions, and it has good test-rest reliability. Although the 1-MSTST is primarily used as a measure for exercise capacity, this test is also representative of lower limb strength.7,8 Because of the readily available equipment needed for this test it is easily performed in the clinic.8 This test is sensitive, and reproducible among participants with lung disease.12
MMT categorizes the ability to generate a force against an external source, and there are a variety of methods to perform MMT (eg, Daniels and Worthingham MMT Grading System, Medical Research Council sum score). In addition, the performance of MMT relies on judgments from the tester.7,13 However, there is concern that MMT does not accurately differentiate impaired muscle strength.7,14
To recap, muscle strength is measurable body function that contributes to the ability for performing activities and participation, but there has not been a systematic analysis of the changes in muscle strength following COVID-19 infection. The purpose of this systematic review is to identify if muscle strength impairment follows COVID-19 infection.
METHODSThis systematic review followed Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines,15 and the protocol for this review was registered with the International Prospective Register of Systematic Reviews (PROSPERO) as 2022: CRD42022307014.16
To identify relevant studies, PubMed, CINAHL, and Cochrane Database of Systematic Reviews were searched. The search was intentionally broad. Based on consultation with a librarian the terms “‘muscle weakness’ OR ‘strength’ OR ‘muscular atrophy,’” were applied, as described in Table 1, inclusive of the years from 2019 to the search date, February 11, 2022.
TABLE 1. - Search Strategy Source Search Strategy CINAHL (EBscoHOST) covid AND(“muscle weakness” OR strength OR “muscular atrophy”) PubMed (National Library of Medicine) covid AND(“muscle weakness” OR strength OR “muscular atrophy”) The Cochrane Central Register of Controlled Trials (EBscoHOST) covid AND(“muscle weakness” OR strength OR “muscular atrophy”)To identify studies reporting muscle weakness following COVID-19 infection the inclusion criteria were observational studies with participants who had COVID-19 infection and a measure of skeletal muscle strength during the 6 months following infection. Additional inclusion criteria were studies reported in English and published in a journal.
Studies were excluded if the participants had a prior diagnosis of cancer and/or neurological pathology, as those pathologies may have contributed to skeletal muscle weakness. In addition, studies were excluded if the only measurement of muscle strength was MMT (including Medical Research Council sum score). As described in the introduction, there are concerns regarding accuracy of measures with MMT, as MMT results do not provide for comparison with predicted normal values determined from regression equations developed using healthy people.
The first phase of the review involved screening titles and abstracts relative to the criteria. Each article was screened by 2 authors working independently, and any conflicting decisions resulted in review by a third author. Included studies advanced to the second phase, in which full text of the studies were obtained and 2 authors independently reviewed the full text of the studies to determine eligibility. Conflicting decisions among the 2 reviewers were resolved by review from a third author.
A table was designed prospectively, and that table was used for recording data from the studies. Data collected included study design, number of participants, mean age of participants, marker(s) for COVID-19 infection severity (eg, hospitalization, critical care), strength outcomes (including the method for measuring strength), the time point (weeks after infection) for measurement, the data source for strength comparison (eg, comparison with normative value), and characteristics accompanying skeletal muscle impairment (eg, myalgia). Some included studies contained more than 1 outcome measurement for strength. Therefore, data were extracted for all strength outcomes, so in those situations all relevant strength outcomes were recorded. Two authors worked independently to extract data from each study, and conflicting reports were resolved by review from a third author.
Assessment of the risk of bias for the included studies was done with the Scottish Intercollegiate Guidelines Network, Methodology Checklist 3: Cohort studies17 as that tool has been endorsed by the American Physical Therapy Association for the review of cohort studies.18 An alternative was STrengthening the Reporting of OBservational studies in Epidemiology (STROBE), which identifies preferred items for inclusion in observational research designs. Although observational studies were the focus of this review, the STROBE checklist was not appropriate as it is not designed for critical appraisal of the methodological quality of studies.19 Two authors applied the criteria from the Scottish Intercollegiate Guidelines Network, Methodology Checklist 3 to identify the relative risk of bias for each study, and conflicts were resolved by review from a third author assessed.
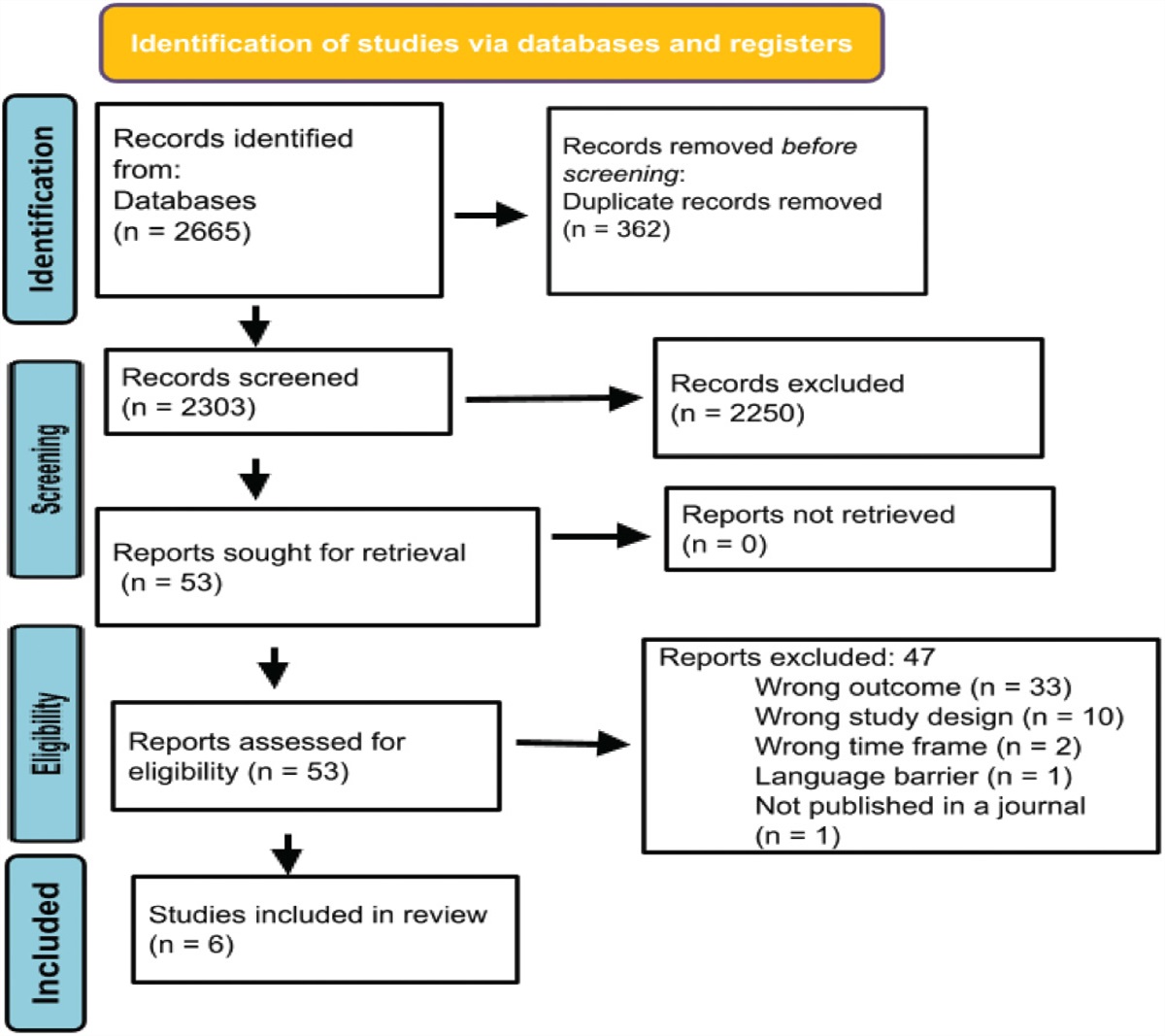
RESULTSThe Covidence platform20 was used to perform all stages of the screening and data extraction. The databases were searched on February 11, 2022, and identified 2665 articles; after removal of 362 duplicates, 2303 articles remained for review (see the Figure). The first phase of screening applied the inclusion and exclusion criteria to article titles and abstracts. That resulted in the exclusion of 2250 articles. The level of agreement among reviewers screening for inclusion was к = 0.647. That is only considered a moderate level of agreement, and all conflicting decisions were resolved by review by a third author. Review of the full text of the 53 remaining studies resulted in the exclusion of 47 studies (reasons for exclusion are identified in the Figure), resulting in 6 studies included in this review. Review of the included studies with the Scottish Intercollegiate Guidelines Network, Methodology Checklist 3: Cohort studies revealed 5 of them to be of acceptable quality21–25 and 1 to be of high quality,26 as identified in Table 2.
 FIGURE.:
FIGURE.: PRISMA flow diagram.
TABLE 2. - Risk of Bias: Results From the Scottish Intercollegiate Guidelines Network, Methodology Checklist 3: Cohort Studiesa Study ID 1.1 1.2 1.3 1.4 1.5 1.6 1.7 1.8 1.9 1.10 1.11 1.12 1.13 1.14 2.1 Wiertz et al,21 2021 Yes DNA Yes DNA 0% DNA Yes No No Yes Yes Yes No No Acceptable (+) Tanriverdi et al,22 2022 Yes DNA Yes No 0% DNA Yes No No Yes Yes DNA Yes No Acceptable (+) van Gassel et al,23 2021 No DNA Yes Yes 12% DNA Yes No No Yes No No No Yes Acceptable (+) Kara et al,24 2021 Yes DNA Yes Yes 0% DNA Yes No No Yes No DNA Yes Yes Acceptable (+) Greco et al,26 2021 Yes Yes Yes Yes 26% subjectsDNA, does not apply.
a1.1: The study addresses an appropriate and clearly focused question; 1.2: The 2 groups being studied are selected from source populations that are comparable in all respects other than the factor under investigation; 1.3: The study indicates how many of the people asked to take part did so, in each of the groups being studied; 1.4: The likelihood that some eligible subjects might have the outcome at the time of enrolment is assessed and taken into account in the analysis; 1.5: What percentage of individuals or clusters recruited into each arm of the study dropped out before the study was completed; 1.6: Comparison is made between full participants and those lost to follow up, by exposure status; 1.7: The outcomes are clearly defined; 1.8: The assessment of outcome is made blind to exposure status. If the study is retrospective this may not be applicable; 1.9: Where blinding was not possible, there is some recognition that knowledge of exposure status could have influenced the assessment of outcome; 1.10: The method of assessment of exposure is reliable; 1.11: Evidence from other sources is used to demonstrate that the method of outcome assessment is valid and reliable; 1.12: Exposure level or prognostic factor is assessed more than once; 1.13: The main potential confounders are identified and taken into account in the design and analysis; 1.14: Have confidence intervals been provided; 2.1: How well was the study done to minimize the risk of bias or confounding.
Collectively, the included studies involved 659 participants with a mean age of 59.8 years. Three of the studies measured skeletal muscle strength within 3 months of the onset of COVID-19 infection (range: 1 week to 3 months)21–23; the timeline for measurement in the other 3 studies was within the 6-month window for this study but was not clearly defined.24–26 Four out of the 6 studies involved participants that were hospitalized21,23–25; 1 study included both participants that were hospitalized and participants that were not21; and 1 study involved residents in a skilled nursing facility.26
Two of the studies involving hospitalized patients also stratified their participants into groups based on severity. One used clinical signs of pneumonia, vital signs, and computed tomography findings as factors to categorize the participants into a cohort of mild, moderate, or severe COVID-19 infection.24 Another study categorized participants into mild (not hospitalized) or moderate severity (hospitalized) groups22 (see Table 3).
Study ID Aim of Study Number of Subjects Mean Age of Subjects, in years COVID-19 Infection Severity Time Since Infection Comparison Strength Outcome Greco et al,26 2021 Evaluate changes in frailty, physical and cognitive performance related to COVID-19 infection among nursing home residents 152 84.4 Not defined 92 (± 10) d Handgrip strength among age-matched controls 19% reduction in handgrip strength compared with age-matched controls (P = .05) Kara et al,24 2021 Investigate the relationship between handgrip strength and disease severity in adult patients with COVID-19 312 46.1 All subjects were hospitalized and categorized with mild, moderate, or severe COVID-19 infection Not clearly defined Gender-specific peak mean value of handgrip strength among healthy young adults; weakness was defined as 2 standard deviations below the gender-specific peak mean value Weakness among 10% of subjects in the mild cohort, 9% in the moderate cohort, and 39.5% in the severe cohort (P < .001) Tanriverdi et al,22 2022 Investigate peripheral muscle strength and physical performance among subjects who recovered from COVID-19 infections 48 39.2 Mild severity (not hospitalized) or moderate severity (hospitalized) At least 12 wk Handgrip and quadriceps strength predicted normal values; weakness was defined as below 80% of the predicted normal value 36% with mild severity had handgrip weakness, 43.5% with moderate severity had handgrip weakness; 24% with mild severity had quadriceps weakness, 47.8% with moderate severity had quadriceps weakness. Handgrip and quadriceps strength were significantly lower in the moderate severity group than in the mild group (P < .05) van Gassel et al,23 2021 Investigate pulmonary function, skeletal muscle and physical functions among mechanically ventilated COVID-19 survivors 46 62 Hospitalized in intensive care unit 3 mo Handgrip strength predicted normal values 81% of predicted handgrip strength (P = .008) Wiertz et al,21 2021 To describe characteristics of subjects with COVID-19 the first week after admission for inpatient rehabilitation 60 59.9 Hospitalized in intensive care unit Not clearly defined Handheld dynamometry predicted normal values 37.35% of predicted shoulder abduction (nondominant) strengthSkeletal muscle strength in the included studies was measured using HGD, handheld dynamometry, or 1-MSTST (see Table 3). Four of the included studies used HGD,22–24,26 3 used handheld dynamometry,21,22,25 and 1 used 1-MSTST.26 Weakness was determined by comparison with normative values and no study provided preinfection measurements for comparison.
All of the included studies reported decreases in skeletal muscle strength following COVID-19 infection. The studies used a variety of methods to measure skeletal muscle strength, and the severity of muscle weakness varied among studies. Among the studies that measured HGD, Greco et al26 measured strength as a percentage of values from age-matched controls and reported a 19% reduction in grip strength. Three studies reported the strength outcome as the percentage of participants with weakness. Tanriverdi et al22 reported 39.6% of their participants had HGD strength below 80% of the normal (predicted) values. Kara et al24 defined low HGD strength as 2 standard deviations below predicted peak values. They reported that among participants with mild COVID-19 infection severity 10% met the threshold for weak, among participants with moderate infection severity 9% were weak, and among participants with severe infection 39% of the participants were weak.26 van Gassel et al23 reported that 81% of participants had weakness when compared with predicted (normal) values.
Wiertz et al21 measured strength using handheld dynamometry and found that there were substantial reductions in strength for motions of shoulder abduction, elbow flexion, wrist extension, hip flexion, and knee extension,21 as described in Table 3. Tanriverdi et al22 reported 35.4% of their participants had knee extension strength below 80% of the normal (predicted) values and Paneroni et al25 reported knee extension weakness (below 80% of predicted values) among 86% of participants and biceps weakness among 73% of participants. Paneroni et al25 also measured lower extremity strength using a 1-MSTST and found that the participants, on average, performed 21 repetitions, which was 63% of the predicted normal for the population.
DISCUSSIONThis systematic review investigated whether muscle strength impairment follows COVID-19 infection. Review of methodological quality revealed that 5 studies were at an acceptable level and 1 at a high level of quality. Therefore, the conclusions are founded on evidence with an acceptable risk of bias.
Together, the studies included 659 participants, with a mean age of 59.8 years. The majority of the participants were hospitalized,20–24 and some were residents in skilled nursing facilities.26 Reduced skeletal muscle strength was identified among participants across age groups and across the severity of the COVID-19 infection. Among those hospitalized and experiencing moderate to severe COVID-19 infection there was greater likelihood, and severity, for muscle strength loss. This is relevant, as strength is an essential physical component for functioning and performing tasks such as ADL and locomotion.
Collectively, the included studies revealed that weakness is a risk following COVID-19 infection. The degree of weakness is similar to skeletal muscle weakness that has been described with postintensive care syndrome27 and acute respiratory distress syndrome.28 However, only 2 of the studies in this review involved participants who were in an intensive care unit, suggesting that COVID-19 infection imposes a greater risk for the development of weakness among those without critical illness. A recent analysis has attributed this to underlying “decreased neural activation, fibre atrophy, necrosis, fibrosis, and alterations in blood flow and metabolic function.”29 This impairment of strength is a likely contributor to the deterioration in exercise capacity and health that persist following COVID-19 infection.30
One study demonstrated a pattern of skeletal muscle weakness that was greater for proximal motions, with better preservation of muscle strength distally.21 In another study, larger muscles (such as the quadriceps and biceps brachii) demonstrated weakness among a high percentage of participants.25 These findings suggest that skeletal muscles with a larger cross-sectional area were at greater risk for demonstrating weakness following COVID-19 infection.21 One study also found a correlation between COVID-19 infection and acceleration of age-related musculoskeletal changes.26 Collectively, the results demonstrated that the risk for COVID-19 associated skeletal muscle weakness may persist for months following the infection, regardless of the severity of the COVID-19 infection.
The strengths of this study included consultation with a research librarian to assist in developing optimal search terms when exploring databases, following the PRISMA guidelines, prospectively registering this research with the PROSPERO, and using Covidence to organize and manage the processes of the review. Beginning the research process with broad search strategies and setting stringent inclusion and exclusion criteria provided confidence that there are no other related studies that could have fit into the designed search. There was a moderate level of agreement among reviewers when screening titles and abstracts for inclusion,31 and all conflicts were resolved through the consensus process.
A limitation within this study was that only studies in English were included. This systematic review does not reveal the cause of the weakness, only the extent and duration of the loss of strength. In future studies it will be beneficial to measure the persistence of the weakness, apply strength measurements that reveal the performance of larger muscle groups, and investigate appropriate clinical interventions to rehabilitate the loss of muscle strength. In addition, revealing the physiological cause for the weakness should be informative to preventative and restorative interventions. Future research should investigate participants with follow-up a year after infection to capture the duration of strength loss.
Because of the heterogeneity of the outcome measures, 2 of the studies in this systematic review were not appropriate for meta-analysis.21,25 The homogeneity of the outcome measures in 4 studies provided the opportunity for performing meta-analysis22–24,26; however, meta-analysis was deemed inappropriate as there was an insufficient number of studies to provide for an acceptable appreciation of variance between studies, creating a risk for incorrect conclusions due to insufficient power.32,33
CONCLUSIONBased on evidence with an acceptable level of methodological quality, this systematic review identifies that patients recovering from a COVID-19 infection are at risk for experiencing weakness in the early months following the infection. We recommend that measurement of strength should be included in the clinician's examination of these patients. Two studies revealed that weakness in proximal or larger muscles was more pronounced than weakness in distal muscles. Measurement with HGD effectively identifies distal upper extremity muscle weakness, but it cannot reveal the performance of proximal or larger muscles. Therefore, we propose that HGD should not be a surrogate measurement for revealing the extent of muscle weakness after COVID-19 infection and clinicians should use strength measurements for the performance of proximal and larger muscles. Those are often relevant for functions such as locomotion, as larger muscles are responsible for tasks such as transferring out of a chair, ambulation or negotiating stairs. Additional research is needed to reveal interventions for the prevention and/or restoration of weakness in skeletal muscles accompanying COVID-19 infection.
REFERENCES 1. Platto S, Xue T, Carafoli E. COVID-19: an announced pandemic. Cell Death Dis. 2020;11(9):799. doi:10.1038/s41419-020-02995-9. 2. Centers for Disease Control and Prevention, National Center for Immunization and Respiratory Diseases, Division of Viral Diseases. Symptoms of COVID-19. https://www.cdc.gov/coronavirus/2019-ncov/symptoms-testing/symptoms.html. Updated October 26, 2022. Accessed June 25, 2023. 3. Department of Health and Human Services. What is long COVID? Long COVID terms and definitions development explained. COVID https://www.covid.gov/longcovid/definitions. Accessed June 25, 2023. 4. Tuzun S, Keles A, Okutan D, Yildiran T, Palamar D. Assessment of musculoskeletal pain, fatigue and grip strength in hospitalized patients with COVID-19. Eur J Phys Rehabil Med. 2021;57(4):653–662. doi:10.23736/S1973-9087.20.06563-6. 5. Disser NP, De Micheli AJ, Schonk MM, et al. Musculoskeletal consequences of COVID-19. J Bone Joint Surg Am. 2020;102(14):1197–1204. doi:10.2106/JBJS.20.00847. 6. Ali AM, Kunugi H. Skeletal muscle damage in COVID-19: a call for action. Medicina (Kaunas). 2021;57(4):372. doi:10.3390/medicina57040372. 7. Bohannon RW. Considerations and practical options for measuring muscle strength: a narrative review. BioMed Res Int. 2019;2019:8194537. doi:10.1155/2019/8194537. 8. Bohannon RW, Crouch RH. 1-minute sit-to-stand test: systematic review of procedures, performance, and clinimetric properties. J Cardiopulm Rehabil Prev. 2019;39(1):2–8. doi:10.1097/HCR.0000000000000336. 9. Roberts HC, Denison HJ, Martin HJ, et al. A review of the measurement of grip strength in clinical and epidemiological studies: towards a standardised approach. Age Ageing. 2011;40(4):423–429. doi:10.1093/ageing/afr051. 10. Arnold CM, Warkentin KD, Chilibeck PD, Magnus CR. The reliability and validity of handheld dynamometry for the measurement of lower-extremity muscle strength in older adults. J Strength Cond Res. 2010;24(3):815–824. doi:10.1519/JSC.0b013e3181aa36b8. 11. Mentiplay BF, Perraton LG, Bower KJ, et al. Assessment of lower limb muscle strength and power using hand-held and fixed dynamometry: a reliability and validity study. PLoS One. 2015;10(10):e0140822. doi:10.1371/journal.pone.0140822. 12. Briand J, Behal H, Chenivesse C, Wémeau-Stervinou L, Wallaert B. The 1-minute sit-to-stand test to detect exercise-induced oxygen desaturation in patients with interstitial lung disease. Ther Adv Respir Dis. 2018;12:1753466618793028. doi:10.1177/1753466618793028. 13. Avers D, Brown M. Daniels and Worthingham's Muscle Testing: Techniques of Manual Examination and Performance Testing. 10th ed. St. Louis, MO: Elsevier; 2019. 14. Toemen A, Dalton S, Sandford F. The intra- and inter-rater reliability of manual muscle testing and a hand-held dynamometer for measuring wrist strength in symptomatic and asymptomatic subjects. Hand Ther. 2011;16(3):67–74. doi:10.1258/ht.2011.011010. 15. Page MJ, Moher D, Bossuyt PM, et al. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ. 2021;372:n160. doi:10.1136/bmj.n160. 16. Arsenault R, Berry-Sullivan S, Lavier S, et al. Is COVID-19 infection associated with loss of muscle strength? A systematic review of the literature. PROSPERO International Prospective Register of Systematic Reviews. 2022, CRD42022307014. https://www.crd.york.ac.uk/PROSPERO. Accessed September 1, 2022. 17. Scottish Intercollegiate Guidelines Network. Methodology Checklist 3: cohort studies. https://www.sign.ac.uk/media/1712/checklist_for_cohort_studies.rtf. Published 2021. Accessed February 16, 2022. 18. American Physical Therapy Association. APTA Clinical Practice Guidelines Development Manual, Revised. https://www.apta.org/patient-care/evidence-based-practice-resources/cpgs/cpg-development/cpg-development-manual. Published March 23, 2021. Accessed June 18, 2023. 19. Strengthening the reporting of observational studies in epidemiology. https://www.strobe-statement.org/. Accessed August 10, 2023. 20. Covidence. Veritas Health Innovation. www.covidence.org. Accessed February 1, 2022. 21. Wiertz CMH, Vints WAJ, Maas GJCM, et al. COVID-19: patient characteristics in the first phase of postintensive care rehabilitation. Arch Rehabil Res Clin Transl. 2021;3(2):100108. doi:10.1016/j.arrct.2021.100108. 22. Tanriverdi A, Savci S, Kahraman BO, Ozpelit E. Extrapulmonary features of post-COVID-19 patients: muscle function, physical activity, mood, and sleep quality. Ir J Med Sci. 2022;191(3):969–975. doi:10.1007/s11845-021-02667-3. 23. van Gassel RJJ, Bels J, Remij L, et al. Functional outcomes and their association with physical performance in mechanically ventilated coronavirus disease 2019 survivors at 3 months following hospital discharge: a cohort study. Crit Care Med. 2021;49(10):1726–1738. doi:10.1097/CCM.0000000000005089. 24. Kara O, Kara M, Akin ME, Özçakar L. Grip strength as a predictor of disease severity in hospitalized COVID-19 patients. Heart Lung. 2021;50(6):743–747. doi:10.1016/j.hrtlng.2021.06.005. 25. Paneroni M, Simonelli C, Saleri M, et al. Muscle strength and physical performance in patients without previous disabilities recovering from COVID-19 pneumonia. Am J Phys Med Rehabil. 2021;100(2):105–109. doi:10.1097/PHM.0000000000001641. 26. Greco GI, Noale M, Trevisan C, et al. Increase in frailty in nursing home survivors of coronavirus disease 2019: comparison with noninfected residents. J Am Med Dir Assoc. 2021;22(5):943–947. doi:10.1016/j.jamda.2021.02.019. 27. Ohtake PJ, Lee AC, Scott JC, et al. Physical impairments associated with post-intensive care syndrome: systematic review based on the World Health Organization's international classification of functioning, disability and health framework. Phys Ther. 2018;98(8):631–645. doi:10.1093/ptj/pzy059. 28. Dinglas VD, Aronson Friedman L, Colantuoni E, et al. Muscle weakness and 5-year survival in acute respiratory distress syndrome survivors. Crit Care Med. 2017;45(3):446–453. doi:10.1097/CCM.0000000000002208. 29. Soares MN, Eggelbusch M, Naddaf E, et al. Skeletal muscle alterations in patients with acute Covid-19 and post-acute sequelae of Covid-19. J Cachexia Sarcopenia Muscle. 2022;13(1):11–22. doi:10.1002/jcsm.12896. 30. Magdy DM, Metwally A, Tawab DA, Hassan SA, Makboul M, Farghaly S. Long-term COVID-19 effects on pulmonary function, exercise capacity, and health status. Ann Thorac Med. 2022;17(1):28–36. doi:10.4103/atm.atm_82_21. 31. McHugh ML. Interrater reliability: the kappa statistic. Biochem Med (Zagreb). 2012;22(3):276–282. 32. Borenstein M, Hedges LV, Higgins J PT, Rothstein HR. Introduction to Meta-Analysis. West Sussex, UK: John Wiley & Sons; 2009. 33. Jackson D, Turner R. Power analysis for random-effects meta-analysis. Res Synth Methods. 2017;8(3):290–302. doi:10.1002/jrsm.1240.
留言 (0)