

記住我
Sarcopenia is a condition characterized by the progressive reduction in muscle mass and strength, affecting both older adults and the general adult population (1, 2). Recent evidence suggests that sarcopenia can have significant effects on various organs and systems, including liver (3, 4).
The liver, as one of the primary organs responsible for metabolism in the human body, plays a vital role in various important functions, including processing substances, detoxification, breaking down fatty acids, and producing bile (5, 6). When the liver is unable to perform its normal physiological functions, it is referred to as abnormal liver function. Common pathological changes associated with abnormal liver function include fatty liver, cirrhosis, and liver cancer, among others (7, 8). The most common symptoms include elevated liver enzymes, and changes in the structure of the liver (9).
The association between sarcopenia and abnormal liver function is not fully understood, but several potential mechanisms have been identified. Metabolic and endocrine changes, such as insulin resistance, disrupted fatty acid metabolism, and inflammation, may adversely affect liver function in muscle atrophy patients (10). Additionally, hormones, cytokines, and neural regulation pathways influenced by sarcopenia may impact liver physiology (11).
Sarcopenia index is a quantitative measure used to assess the degree of muscle loss and functional decline in individuals (12). However, the nature and extent of its relationship with abnormal liver function have not been conclusively established in the existing literature. In this study, we conducted a rigorous analysis utilizing the data from the 2017–2018 cycle of the NHANES to investigate the association between the sarcopenia index and abnormal liver function in adults. This research aims to provide a theoretical foundation and guidance for further understanding the impact of sarcopenia on liver health, ultimately leading to improved healthcare recommendations for individuals.
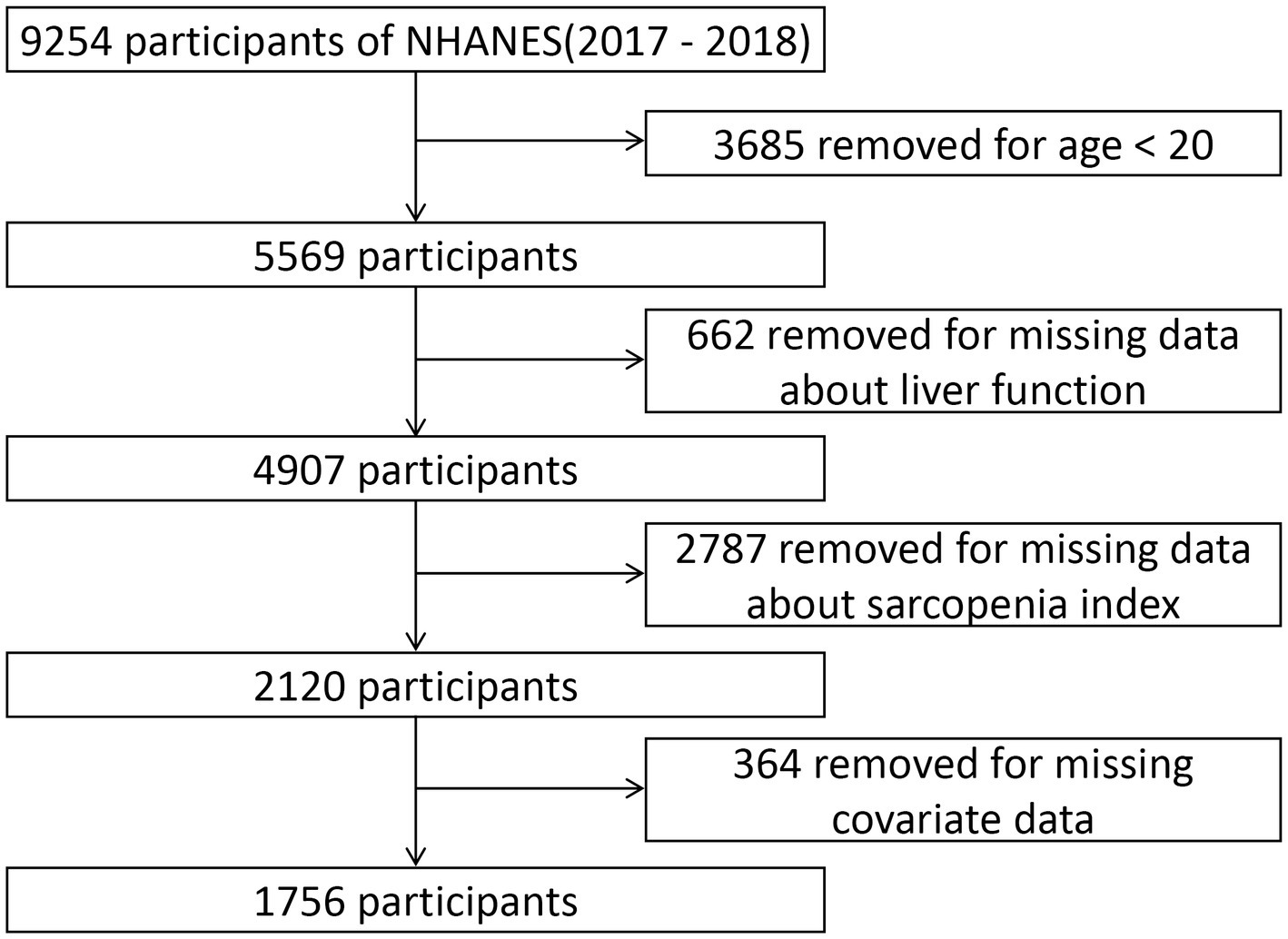
2 Methods 2.1 Study populationIn the NHANES, a biennial national health survey conducted by the National Center for Health Statistics (NCHS), comprehensive data on the health status of the population in the United States is collected (13). This publicly accessible dataset provides extensive information on nutrition and overall health of the general population. The survey data has been ethically approved by the NCHS Institutional Review Board, allowing researchers and users to access it. For this study, we utilized the aggregated NHANES data from the combined years of 2017 and 2018. Participants were excluded from the analysis if they met any of the following criteria: (1) age below 20 years, (2) absence of liver function indicators, (3) inability to calculate the sarcopenia index, and (4) missing covariate data. The final analysis included a total of 1756 individuals, as depicted in Figure 1.
Figure 1. Flowchart illustrating the criteria for participant selection and exclusion in our study cohort.
2.2 Sarcopenia indexThe primary variable under investigation in this study is the sarcopenia index. NHANES utilizes dual-energy X-ray absorptiometry (DXA) to assess the appendicular lean mass (ALM), which represents the cumulative skeletal muscle mass of the limbs. The sarcopenia index is computed by dividing the ALM (measured in kilograms) by the BMI (body mass index), which is determined by dividing the weight (measured in kilograms) obtained during the physical examination by the square of the height (measured in meters) (10, 14).
2.3 Liver function measurement resultsBlood samples from NHANES participants were meticulously collected at a mobile examination center. These invaluable samples were carefully preserved in small vials under optimal refrigeration conditions (2–8°C) and expeditiously transported to the esteemed Advanced Research and Diagnostic Laboratory (ARDL) at the University of Minnesota. Utilizing the cutting-edge Roche Cobas 6000 chemistry analyzer (Cobas 6000), the laboratory conducted a comprehensive analysis of serum liver function indicators (accessible on the official NHANES).
The liver, a vital organ, is abundant in two crucial enzymes: alanine aminotransferase (ALT) and aspartate aminotransferase (AST). Elevated serum levels of these enzymes serve as markers of liver cell damage (15). Additionally, alkaline phosphatase (ALP) and gamma-glutamyl transferase (GGT) are also markers of abnormal liver function (16). Furthermore, the liver plays a pivotal role in the metabolism of bilirubin, encompassing its uptake, conjugation, and excretion. Dysfunctions in any of these processes can contribute to elevated levels of total bilirubin (TBIL) (17). In this study, abnormal liver function is defined as elevated levels of ALT, AST, ALP, GGT, or TBIL that exceed the upper limits of the established normal range (AST: 0–37 U/L for males, 0–31 U/L for females; ALT: 0–40 U/L for males, 0–31 U/L for females; ALP: 40–129 U/L for males, 35–104 U/L for females; GGT: 11–51 U/L for males, 7–33 U/L for females; TBIL: 1.0 mg/dL).
2.4 Potential covariatesBased on previous studies, the following variables were included as covariates in our analysis: age (<40 years/≥40 years), gender (male/female), race (Hispanic White/Non-Hispanic Black/Mexican American/Other Hispanic/Other), smoking status (ever smoked at least 100 cigarettes/never smoked) (18), alcohol consumption (ever consumed any type of alcoholic beverage/never consumed) (19), hypertension (systolic blood pressure ≥ 140 mmHg/diastolic blood pressure ≥ 90 mmHg/clinically diagnosed hypertension/current use of antihypertensive medication), diabetes (clinically diagnosed diabetes/glycated hemoglobin ≥6.5%/current use of antidiabetic medication), cancer (clinically diagnosed cancer), gallstones (diagnosed with gallstones by a healthcare professional), physical activity level (being classified as active requires participating in a minimum of 75 min of vigorous-intensity exercise per week or 150 min of moderate-intensity exercise per week; being considered insufficiently active means engaging in fewer than 75 min of vigorous-intensity exercise per week or less than 150 min of moderate-intensity exercise per week; being classified as inactive means not engaging in any form of physical activity) (20), depression (total score ≥ 10 on a nine-item depression screening tool) (21), and hepatitis status (hepatitis B/hepatitis C).
2.5 Statistical analysisSampling weights were applied in the NHANES to account for the complex study design. We utilized the recommended 2-year sample weights (WTMEC2YR) provided by the Centers for Disease Control and Prevention for the mobile examination centers. Baseline characteristics and univariate analysis of abnormal liver function were presented as mean ± standard deviation for continuous variables, while categorical variables were expressed as percentages with a 95% confidence interval. Weighted one-way ANOVA and t-tests were applied to continuous variables, while chi-square tests were utilized for categorical variables to assess disparities among different categories of the sarcopenia index and the risk factors for abnormal liver function.
Three logistic regression models were employed to investigate the independent association between the sarcopenia index and abnormal liver function, with adjustments made for potential confounding factors. Model 1 remained unadjusted, while Model 2 included adjustments for age, gender, and race. Model 3 accounted for additional adjustments, including smoking status, alcohol consumption, hypertension, diabetes, cancer, gallstones, physical activity, depression and hepatitis status. To comprehensively explore this relationship, the sarcopenia index was analyzed both as a continuous variable and stratified into three categories (<0.663, 0.663–0.884, >0.884) based on tertiles. Furthermore, a two-stage linear regression model was utilized to assess the potential threshold effect of the sarcopenia index on abnormal liver function, as indicated by the fitted smooth curve plot. A testing approach was employed to identify the inflection point where the relationship between the sarcopenia index and abnormal liver function exhibited significant changes, optimizing the model likelihood within a predefined interval. Additionally, a log-likelihood ratio test was conducted to compare the fit of a linear regression model (piecewise linear regression model) with that of a two-stage linear regression model.
Lastly, a gender-stratified subgroup analysis was conducted to examine the relationship between the sarcopenia index and abnormal liver function within different gender groups.
All statistical analyses were conducted using the R, Stata, and EmpowerStats software packages. Statistical significance was defined as a p-value of <0.05 (two-tailed).
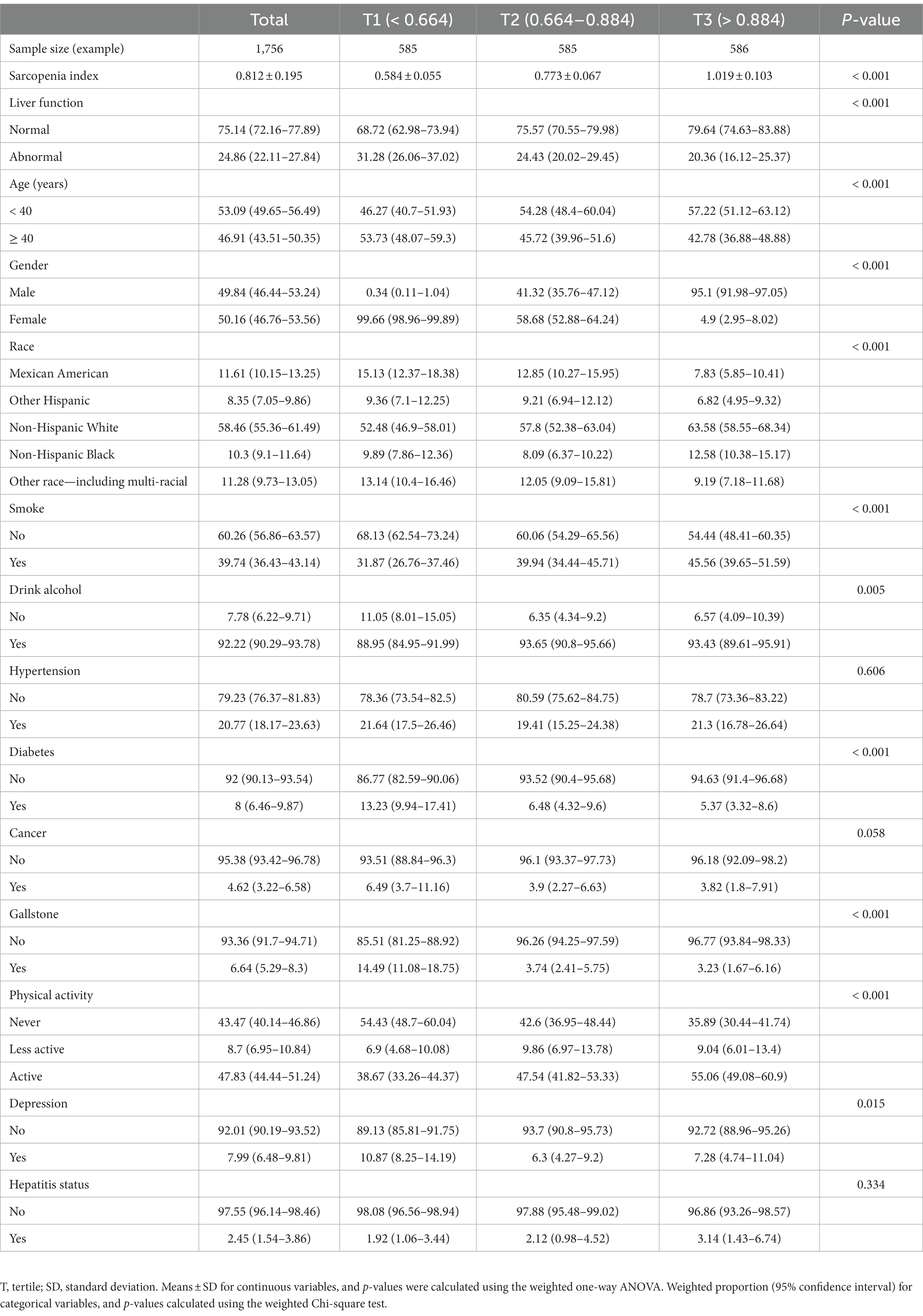
3 Results 3.1 Participant characteristicsA total of 1,756 adult Americans participated in the study, with 53.09% being younger than 40 years old and 46.91% being 40 years old or older. Female participants made up 50.16% and male participants 49.84%. Table 1 presents participant characteristics at baseline, categorized by distinct sarcopenia index levels. Approximately 24.86% of the participants had abnormal liver function. The proportions of participants with abnormal liver function were 31.28, 24.43, and 20.36% in the groups with sarcopenia index <0.664, 0.664–0.884, and > 0.884, respectively.
Table 1. Characteristics of participants stratified by sarcopenia index tertiles (tertiles 1–3).
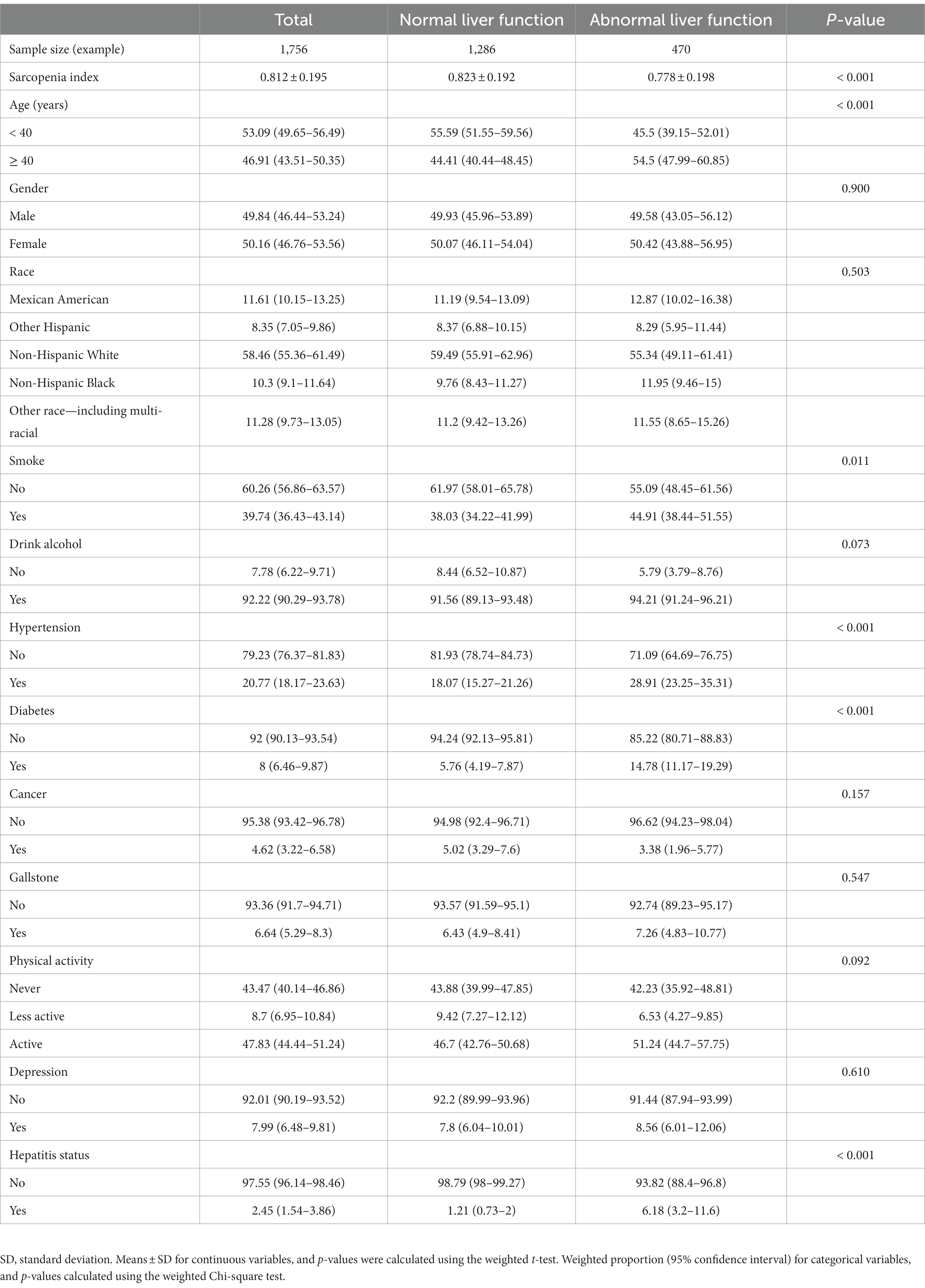
3.2 Univariate analysisAmong the 1,756 participants, 1,286 (73.23%) were categorized as having normal liver function, while 470 (26.77%) were categorized as having abnormal liver function. A statistically significant difference was not found between the two groups in regards to gender, race, alcohol consumption, cancer, gallstones, physical activity, or depression between the two groups (p > 0.05). However, the differences between the two groups were statistically significant in terms of sarcopenia index, age, smoking status, hypertension, diabetes, and hepatitis status (p < 0.05), as shown in Table 2.
Table 2. Univariate analysis between patients with and without abnormal liver function.
3.3 Multiple regression analysisThree multivariable logistic regression models were employed to investigate the association between the sarcopenia index and abnormal liver function (Table 3). Model 1 was unadjusted, while Model 2 controlled for age, sex, and race. Model 3 further adjusted for additional factors, including smoking status, alcohol consumption, hypertension, diabetes, cancer, gallstones, physical activity, depression and hepatitis status. Consistently across all three models, a significant inverse relationship was observed between the sarcopenia index and abnormal liver function. For each 0.1-unit increase in the sarcopenia index, the impact on abnormal liver function was as follows: Model 1 (OR = 0.88, 95% CI: 0.81–0.97), Model 2 (OR = 0.72, 95% CI: 0.62–0.85), and Model 3 (OR = 0.73, 95% CI: 0.63–0.86).
Table 3. Association between the sarcopenia index and the odds of abnormal liver function.
When assessing various levels of the sarcopenia index, individuals in the second tertile exhibited no significant difference in the probability of abnormal liver function compared to those with the sarcopenia index levels in the lowest tertile, as indicated by the findings in Model 1 (OR = 0.71, 95% CI: 0.49–1.02). However, in Model 2 (OR = 0.48, 95% CI: 0.30–0.77) and Model 3 (OR = 0.52, 95% CI: 0.32–0.84), they demonstrated a reduced likelihood. Notably, individuals in the highest tertile had a significantly lower likelihood of abnormal liver function in Model 1 (OR = 0.56, 95% CI: 0.38–0.82), Model 2 (OR = 0.24, 95% CI: 0.13–0.46), and Model 3 (OR = 0.28, 95% CI: 0.15–0.55). Furthermore, the trend p-values for all three models were less than 0.01.
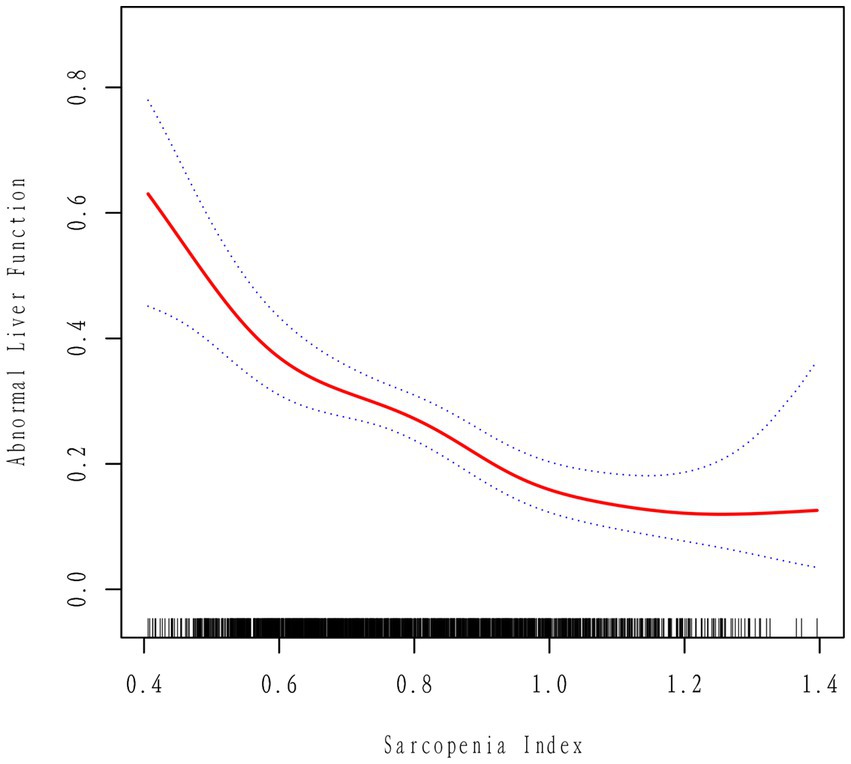
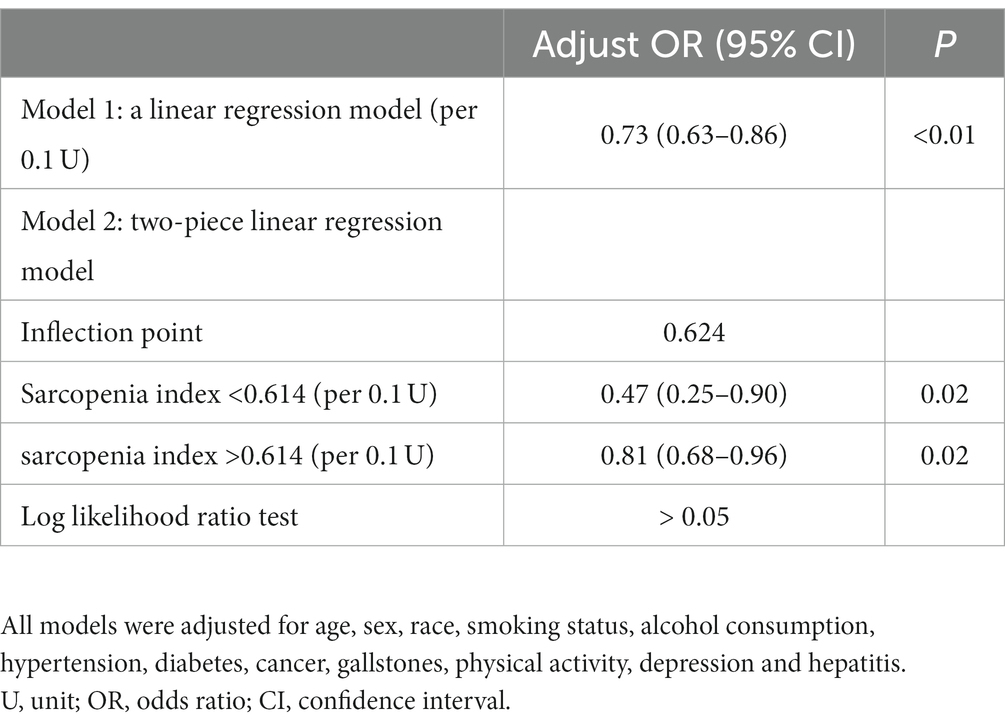
3.4 Nonlinear analysisFigure 2 illustrates a notable nonlinear relationship between the sarcopenia index and abnormal liver function, after adjusting for all relevant covariates. The probability of developing abnormal liver function gradually decreases as the sarcopenia index increases. Subsequently, a two-stage linear regression model was constructed by identifying the optimal inflection point that maximized the model likelihood. A likelihood ratio test was conducted to compare the two-stage linear regression model with a linear regression model, and the results indicated no statistically significant difference (p > 0.05). These findings suggest that the presence of a significant inflection point is not supported (Table 4).
Figure 2. Correlation between the sarcopenia index and abnormal liver function, after adjusting for all covariates, as depicted by a smoothed curve. The two dashed lines represent the upper and lower limits of the 95% confidence interval.
Table 4. Threshold analysis of the sarcopenia index on abnormal liver function.
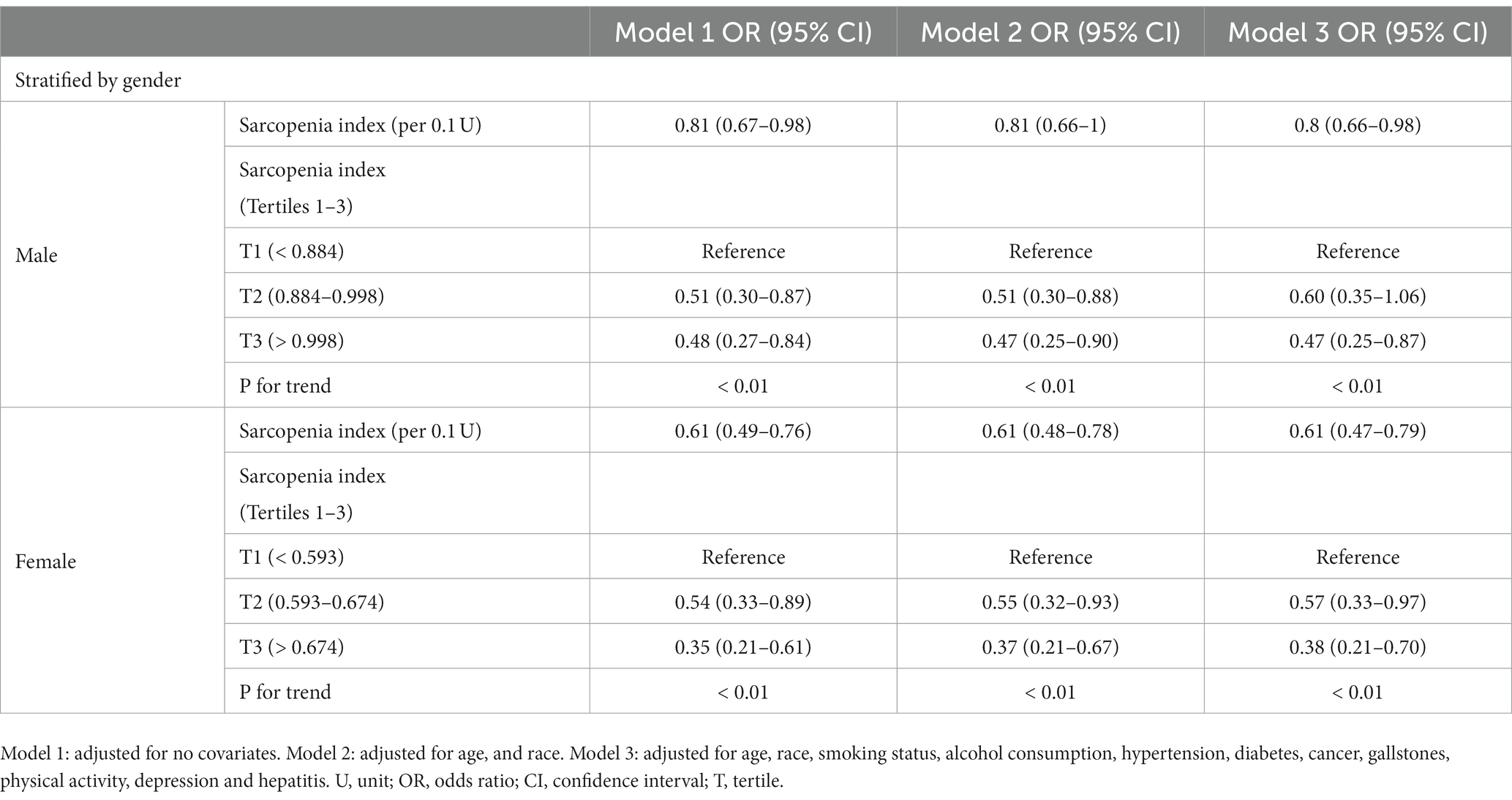
3.5 Subgroup analysisWhen stratified by gender, in multivariable-adjusted models among male participants, we identified a statistically significant difference (p < 0.05) in the association between the sarcopenia index and abnormal liver function. Compared to individuals in the lowest tertile of the sarcopenia index, those in the highest tertile exhibited a reduced likelihood of experiencing abnormal liver function with an odds ratio of 0.47 (95% CI, 0.25–0.87). However, among female participants, for every 0.1 unit increase in the muscle depletion index, the probabilities of having abnormal liver function were 0.61 (95% CI, 0.49–0.76), 0.61 (95% CI, 0.48–0.78), and 0.61 (95% CI, 0.47–0.79) in Model1, Model2, and Model3, respectively. The negative correlation between the sarcopenia index and abnormal liver function persisted. In all three adjusted models, compared to participants at the lowest tertile of the sarcopenia index, those at the second and third tertiles had a reduced likelihood of experiencing abnormal liver function. The trend p-values for all three models were less than 0.01 (Table 5).
Table 5. Associations between sarcopenia index and odds of abnormal liver function by gender.
4 DiscussionThis study aimed to explore the relationship between the sarcopenia index and abnormal liver function. The results demonstrated a significant inverse correlation between the sarcopenia index and the occurrence of abnormal liver function, with a notable decrease in the incidence as the sarcopenia index increased. This association was further substantiated by the fitting of a smooth curve, providing additional evidence. Furthermore, gender-stratified analysis revealed a statistically significant relationship predominantly among females.
Sarcopenia, a condition characterized by muscle wasting, can exert substantial deleterious effects on multiple physiological organs, including the liver. Previous research endeavors have unveiled a compelling nexus between sarcopenia and the initiation as well as progression of hepatic pathologies, encompassing non-alcoholic fatty liver disease, cirrhosis, and hepatocellular carcinoma. In order to elucidate this correlation, a comprehensive inquiry encompassing 309 instances, led by Koo et al. (22), has definitively established a substantial relationship between diminished skeletal muscle mass and the histopathological gravity of non-alcoholic fatty liver disease. Additionally, sarcopenia has exhibited a pronounced correlation with non-alcoholic steatohepatitis within this context. Furthermore, a retrospective analysis comprising 8,361 subjects has discerned sarcopenia as a pivotal gauge of the severity of non-alcoholic fatty liver disease (23). Tandon et al. (24), in a systematic analysis, have explicated the proclivity of sarcopenia in influencing the prevalence and fatality rates associated with cirrhosis. In a meta-analysis incorporating findings from 22 studies, Tantai et al. (25) have underscored the escalating mortality rates in cirrhosis patients, concomitant with the severity and duration of sarcopenia. Notably, Perisetti et al. (26) have documented the early manifestation of sarcopenia in hepatocellular carcinoma, alongside its close correlation with mortality rates in hepatocellular carcinoma cases. These investigations corroborate our own research outcomes and provide further empirical substantiation, particularly in the quantification of the interrelation between sarcopenia index and abnormal liver function.
The potential mechanistic underpinnings delineating the nexus between sarcopenia and abnormal liver function encompass a spectrum of contributory facets, as follows: Firstly, sarcopenia may adversely affect liver function through insulin resistance. Sarcopenia results in decreased responsiveness of muscle tissue to insulin, leading to reduced glucose uptake and elevated blood sugar levels (10, 27). High insulin levels stimulate glucose production in the liver while inhibiting glycogen synthesis and utilization, causing excessive accumulation of glucose and fat in the liver, ultimately resulting in liver damage (28). Secondly, sarcopenia may adversely affect liver function through disruptions in fatty acid metabolism. Disruptions in fatty acid metabolism pose challenges to the liver, leading to oxidative stress and fat accumulation, triggering oxidative stress and inflammatory responses (29). This can result in liver cell injury and functional abnormalities. Thirdly, sarcopenia may affect liver function through inflammatory responses (29). The inflammatory responses triggered by sarcopenia may be associated with muscle tissue damage, release of inflammatory mediators, as well as inflammation in adipose tissue and oxidative stress caused by malnutrition. These inflammatory factors can enter the circulatory system and affect the liver, leading to liver cell damage and functional abnormalities. Fourthly, sarcopenia may adversely affect liver function through dysregulated hormone regulation. Sarcopenia contributes to insulin resistance, disrupting normal carbohydrate and fat metabolism, resulting in liver fat accumulation and abnormal cholesterol synthesis (30). Additionally, sarcopenia may lower testosterone and growth hormone levels, impacting fat metabolism and muscle tissue recovery, further negatively affecting liver function (31). Fifthly, sarcopenia may adversely affect liver function through dysregulated cytokine regulation. Sarcopenia leads to decreased muscle tissue and impaired function, which may trigger inflammatory responses and excessive release of cytokines. These inflammatory cytokines, such as TNF-α, IL-6, and C-reactive protein, can induce liver inflammation and fibrosis, causing liver cell damage and interfering with liver function (32). Furthermore, sarcopenia may also reduce anti-inflammatory factors, disrupting cytokine balance and exacerbating liver inflammation and functional abnormalities (32). These dysregulated mechanisms interact with each other, ultimately leading to the occurrence and development of abnormal liver function. Finally, sarcopenia may adversely affect liver function through abnormal neural regulation. The nervous system plays a crucial role in regulating metabolism, inflammatory responses, and hormonal balance in the body (33). Sarcopenia can lead to heightened sympathetic nervous system activity and diminished parasympathetic nervous system activity, disrupting the delicate balance of the neurophysiological milieu. This disruption may induce an upregulation of inflammatory and stress responses, thereby exerting an adverse influence on hepatic function (34). Additionally, sarcopenia may interfere with neural regulatory pathways between muscle and liver, affecting liver physiological regulation and metabolic activities. The occurrence of insulin resistance may also be one of the mechanisms by which sarcopenia affects liver function through neural regulation (34).
Subsequent investigations conducted among different genders have unveiled that the influence of the sarcopenia index on abnormal liver function is notably more pronounced within the female demographic. Several factors may contribute to the greater manifestation of abnormal liver function caused by sarcopenia in women. Firstly, females generally possess higher levels of body fat and lower muscle mass physiologically (35, 36). Under conditions where muscle mass changes are equivalent, the impact on liver function may be more evident. Additionally, the accumulation of body fat is closely associated with hepatic fat accumulation, which can lead to the development of fatty liver and non-alcoholic fatty liver disease (37). Consequently, this can trigger abnormal liver function. Secondly, this gender disparity could be attributed to the protective effects of estrogen on female liver function, which may enhance the association between the sarcopenia index and abnormal liver function in women (38, 39).
Moreover, amid the set of covariates ascertained in this inquiry, a statistically significant differentiation in terms of abnormal liver function coinciding with hypertension has been discerned. A working hypothesis posits that this phenomenon can be ascribed to heightened blood pressure inciting pro-inflammatory cascades encompassing TNF-α and interleukins, adipokines, and leptin, potentially predisposing to hepatotoxicity (40). Parallelly, findings from animal experiments have suggested that hypertension-induced liver injury may emanate from the confluence of anomalies in hepatic fatty acid metabolism and concurrent microcirculatory disturbances (41). These mechanistic determinants, among others, beckon additional rigorous scrutiny to validate their veracity.
The present study conducted a comprehensive investigation with a large sample size to explore the association between the sarcopenia index and abnormal liver function, while rigorously adjusting for potential confounding factors to ensure the reliability of the results. However, the study does have some limitations. Firstly, due to its cross-sectional design, it is not possible to establish a causal relationship, and further prospective cohort studies are needed to confirm causality. Secondly, there is currently no universally accepted definition for the sarcopenia index. Thirdly, there may still be unaccounted confounding factors that could potentially bias the accurate assessment of the true associations.
5 ConclusionThis cross-sectional study yields robust evidence indicating a negative correlation between the sarcopenia index and abnormal liver function, predominantly observed among females. Consequently, individuals with lower sarcopenia index values should consider enhancing their physical exercise regimens, increasing protein intake, and managing underlying health conditions such as diabetes, inflammatory bowel disease, and renal disorders, which may contribute to muscle loss. These measures can lead to an improvement in sarcopenia index and potentially help mitigate the risk of abnormal liver function.
Data availability statementThe datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/supplementary material.
Ethics statementThe studies involving humans were approved by the National Center for Health Statistics. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributionsJX: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Validation, Writing – original draft. Z-XX: Data curation, Software, Writing – review & editing. Q-FY: Resources, Software, Writing – review & editing. JZ: Data curation, Resources, Writing – review & editing. XZ: Resources, Visualization, Writing – review & editing. JY: Conceptualization, Supervision, Writing – review & editing.
FundingThe author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was supported by a grant from Zhenjiang Science and Technology Bureau (Project No. SH2023042).
AcknowledgmentsThe authors appreciate the efforts given by participants in the NHANES project.
Conflict of interestThe authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s noteAll claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes References2. Sayer, AA, and Cruz-Jentoft, A. Sarcopenia definition, diagnosis and treatment: consensus is growing. Age Ageing. (2022) 51:afac220. doi: 10.1093/ageing/afac220
CrossRef Full Text | Google Scholar
3. Buchard, B, Boirie, Y, Cassagnes, L, Lamblin, G, Coilly, A, and Abergel, A. Assessment of malnutrition, sarcopenia and frailty in patients with cirrhosis: which tools should we use in clinical practice? Nutrients. (2020) 12:186. doi: 10.3390/nu12010186
CrossRef Full Text | Google Scholar
4. Fernández-Mincone, T, Contreras-Briceño, F, Espinosa-Ramírez, M, García-Valdés, P, López-Fuenzalida, A, Riquelme, A, et al. Nonalcoholic fatty liver disease and sarcopenia: pathophysiological connections and therapeutic implications. Expert Rev Gastroenterol Hepatol. (2020) 14:1141–57. doi: 10.1080/17474124.2020.1810563
CrossRef Full Text | Google Scholar
5. Mega, A, Marzi, L, Kob, M, Piccin, A, and Floreani, A. Food and nutrition in the pathogenesis of liver damage. Nutrients. (2021) 13:1326. doi: 10.3390/nu13041326
CrossRef Full Text | Google Scholar
6. Zhou, M, Deng, Y, Liu, M, Liao, L, Dai, X, Guo, C, et al. The pharmacological activity of berberine, a review for liver protection. Eur J Pharmacol. (2021) 890:173655. doi: 10.1016/j.ejphar.2020.173655
PubMed Abstract | CrossRef Full Text | Google Scholar
9. Chen, VL, Du, X, Chen, Y, Kuppa, A, Handelman, SK, Vohnoutka, RB, et al. Genome-wide association study of serum liver enzymes implicates diverse metabolic and liver pathology. Nat Commun. (2021) 12:816. doi: 10.1038/s41467-020-20870-1
PubMed Abstract | CrossRef Full Text | Google Scholar
10. Kim, JA, and Choi, KM. Sarcopenia and fatty liver disease. Hepatol Int. (2019) 13:674–87. doi: 10.1007/s12072-019-09996-7
CrossRef Full Text | Google Scholar
11. Kuchay, MS, Martínez-Montoro, JI, Kaur, P, Fernández-García, JC, and Ramos-Molina, B. Non-alcoholic fatty liver disease-related fibrosis and sarcopenia: an altered liver-muscle crosstalk leading to increased mortality risk. Ageing Res Rev. (2022) 80:101696. doi: 10.1016/j.arr.2022.101696
PubMed Abstract | CrossRef Full Text | Google Scholar
12. Cruz-Jentoft, AJ, Bahat, G, Bauer, J, Boirie, Y, Bruyère, O, Cederholm, T, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. (2019) 48:16–31. doi: 10.1093/ageing/afy169
PubMed Abstract | CrossRef Full Text | Google Scholar
13. Chen, T-C, Clark, J, Riddles, MK, Mohadjer, LK, and Fakhouri, THI. National health and nutrition examination survey, 2015-2018: sample design and estimation procedures. National Center for Health Statistics. Vital Health Statistics. Vol. 2. Washington, DC, USA (2020). 1–35.
14. Zhang, Y, Tian, C, Wang, Y, Zhang, H, Ni, J, Song, W, et al. Association between sarcopenia and kidney stones in United States adult population between 2011 and 2018. Front Nutr. (2023) 10:1123588. doi: 10.3389/fnut.2023.1123588
PubMed Abstract | CrossRef Full Text | Google Scholar
15. Whitehead, MW, Hawkes, ND, Hainsworth, I, and Kingham, JG. A prospective study of the causes of notably raised aspartate aminotransferase of liver origin. Gut. (1999) 45:129–33. doi: 10.1136/gut.45.1.129
PubMed Abstract | CrossRef Full Text | Google Scholar
16. Yu, L, Yang, M, Cheng, M, Fan, L, Wang, X, Xu, T, et al. Associations between urinary phthalate metabolite concentrations and markers of liver injury in the US adult population. Environ Int. (2021) 155:106608. doi: 10.1016/j.envint.2021.106608
PubMed Abstract | CrossRef Full Text | Google Scholar
17. Newsome, PN, Cramb, R, Davison, SM, Dillon, JF, Foulerton, M, Godfrey, EM, et al. Guidelines on the management of abnormal liver blood tests. Gut. (2018) 67:6–19. doi: 10.1136/gutjnl-2017-314924
CrossRef Full Text | Google Scholar
18. Kim, D, Konyn, P, Sandhu, KK, Dennis, BB, Cheung, AC, and Ahmed, A. Metabolic dysfunction-associated fatty liver disease is associated with increased all-cause mortality in the United States. J Hepatol. (2021) 75:1284–91. doi: 10.1016/j.jhep.2021.07.035
PubMed Abstract | CrossRef Full Text | Google Scholar
19. Xie, ZQ, Li, HX, Tan, WL, Yang, L, Ma, XW, Li, WX, et al. Association of serum vitamin C with NAFLD and MAFLD among adults in the United States. Front Nutr. (2021) 8:795391. doi: 10.3389/fnut.2021.795391
PubMed Abstract | CrossRef Full Text | Google Scholar
20. Cao, C, Friedenreich, CM, and Yang, L. Association of daily sitting time and leisure-time physical activity with survival among US cancer survivors. JAMA Oncol. (2022) 8:395–403. doi: 10.1001/jamaoncol.2021.6590
PubMed Abstract | CrossRef Full Text | Google Scholar
21. Iranpour, S, and Sabour, S. Inverse association between caffeine intake and depressive symptoms in US adults: data from National Health and nutrition examination survey (NHANES) 2005-2006. Psychiatry Res. (2019) 271:732–9. doi: 10.1016/j.psychres.2018.11.004
PubMed Abstract | CrossRef Full Text | Google Scholar
22. Koo, BK, Kim, D, Joo, SK, Kim, JH, Chang, MS, Kim, BG, et al. Sarcopenia is an independent risk factor for non-alcoholic steatohepatitis and significant fibrosis. J Hepatol. (2017) 66:123–31. doi: 10.1016/j.jhep.2016.08.019
CrossRef Full Text | Google Scholar
23. Chun, HS, Kim, MN, Lee, JS, Lee, HW, Kim, BK, Park, JY, et al. Risk stratification using sarcopenia status among subjects with metabolic dysfunction-associated fatty liver disease. J Cachexia Sarcopenia Muscle. (2021) 12:1168–78. doi: 10.1002/jcsm.12754
PubMed Abstract | CrossRef Full Text | Google Scholar
24. Tandon, P, Montano-Loza, AJ, Lai, JC, Dasarathy, S, and Merli, M. Sarcopenia and frailty in decompensated cirrhosis. J Hepatol. (2021) 75:S147–62. doi: 10.1016/j.jhep.2021.01.025
PubMed Abstract | CrossRef Full Text | Google Scholar
25. Tantai, X, Liu, Y, Yeo, YH, Praktiknjo, M, Mauro, E, Hamaguchi, Y, et al. Effect of sarcopenia on survival in patients with cirrhosis: a meta-analysis. J Hepatol. (2022) 76:588–99. doi: 10.1016/j.jhep.2021.11.006
PubMed Abstract | CrossRef Full Text | Google Scholar
26. Perisetti, A, Goyal, H, Yendala, R, Chandan, S, Tharian, B, and Thandassery, RB. Sarcopenia in hepatocellular carcinoma: current knowledge and future directions. World J Gastroenterol. (2022) 28:432–48. doi: 10.3748/wjg.v28.i4.432
PubMed Abstract | CrossRef Full Text | Google Scholar
27. Consitt, LA, Dudley, C, and Saxena, G. Impact of endurance and resistance training on skeletal muscle glucose metabolism in older adults. Nutrients. (2019) 11:2636. doi: 10.3390/nu11112636
CrossRef Full Text | Google Scholar
28. Norton, L, Shannon, C, Gastaldelli, A, and DeFronzo, RA. Insulin: the master regulator of glucose metabolism. Metabolism. (2022) 129:155142. doi: 10.1016/j.metabol.2022.155142
CrossRef Full Text | Google Scholar
29. Li, C-W, Yu, K, Shyh-Chang, N, Jiang, Z, Liu, T, Ma, S, et al. Pathogenesis of sarcopenia and the relationship with fat mass: descriptive review. J Cachexia Sarcopenia Muscle. (2022) 13:781–94. doi: 10.1002/jcsm.12901
CrossRef Full Text | Google Scholar
30. D’Souza, K, Mercer, A, Mawhinney, H, Pulinilkunnil, T, Udenigwe, CC, and Kienesberger, PC. Whey peptides stimulate differentiation and lipid metabolism in adipocytes and ameliorate lipotoxicity-induced insulin resistance in muscle cells. Nutrients. (2020) 12:425. doi: 10.3390/nu12020425
CrossRef Full Text | Google Scholar
31. Batsis, JA, and Villareal, DT. Sarcopenic obesity in older adults: aetiology, epidemiology and treatment strategies. Nat Rev Endocrinol. (2018) 14:513–37. doi: 10.1038/s41574-018-0062-9
PubMed Abstract | CrossRef Full Text | Google Scholar
33. Delbono, O, Rodrigues, ACZ, Bonilla, HJ, and Messi, ML. The emerging role of the sympathetic nervous system in skeletal muscle motor innervation and sarcopenia. Ageing Res Rev. (2021) 67:101305. doi: 10.1016/j.arr.2021.101305
PubMed Abstract | CrossRef Full Text | Google Scholar
34. Nishikawa, H, Fukunishi, S, Asai, A, Yokohama, K, Nishiguchi, S, and Higuchi, K. Pathophysiology and mechanisms of primary sarcopenia (review). Int J Mol Med. (2021) 48:156. doi: 10.3892/ijmm.2021.4989
CrossRef Full Text | Google Scholar
35. Janssen, I, Heymsfield, SB, Wang, ZM, and Ross, R. Skeletal muscle mass and distribution in 468 men and women aged 18-88 yr. J Appl Physiol (1985). (2000) 89:81–8. doi: 10.1152/jappl.2000.89.1.81
CrossRef Full Text | Google Scholar
36. Hori, Y, Hoshino, M, Inage, K, Miyagi, M, Takahashi, S, Ohyama, S, et al. Gender-specific analysis for the association between trunk muscle mass and spinal pathologies. Sci Rep. (2021) 11:7816. doi: 10.1038/s41598-021-87334-4
PubMed Abstract | CrossRef Full Text | Google Scholar
37. Johannesdottir, F, Allaire, B, Anderson, DE, Samelson, EJ, Kiel, DP, and Bouxsein, ML. Population-based study of age- and sex-related differences in muscle density and size in thoracic and lumbar spine: the Framingham study. Osteoporos Int. (2018) 29:1569–80. doi: 10.1007/s00198-018-4490-0
PubMed Abstract | CrossRef Full Text | Google Scholar
38. Lee, C, Kim, J, Han, J, Oh, D, Kim, M, Jeong, H, et al. Formyl peptide receptor 2 determines sex-specific differences in the progression of nonalcoholic fatty liver disease and steatohepatitis. Nat Commun. (2022) 13:578. doi: 10.1038/s41467-022-28138-6
CrossRef Full Text | Google Scholar
40. Musso, G, Gambino, R, De Michieli, F, Durazzo, M, Pagano, G, and Cassader, M. Adiponectin gene polymorphisms modulate acute adiponectin response to dietary fat: possible pathogenetic role in NASH. Hepatology. (2008) 47:1167–77. doi: 10.1002/hep.22142
PubMed Abstract | CrossRef Full Text | Google Scholar
41. Li, B, He, X, Lei, S-S, Zhou, FC, Zhang, NY, Chen, YH, et al. Hypertensive rats treated chronically with Nω-nitro-L-arginine methyl Ester (L-NAME) induced disorder of hepatic fatty acid metabolism and intestinal pathophysiology. Front Pharmacol. (2020) 10:1677. doi: 10.3389/fphar.2019.01677
留言 (0)