
記住我

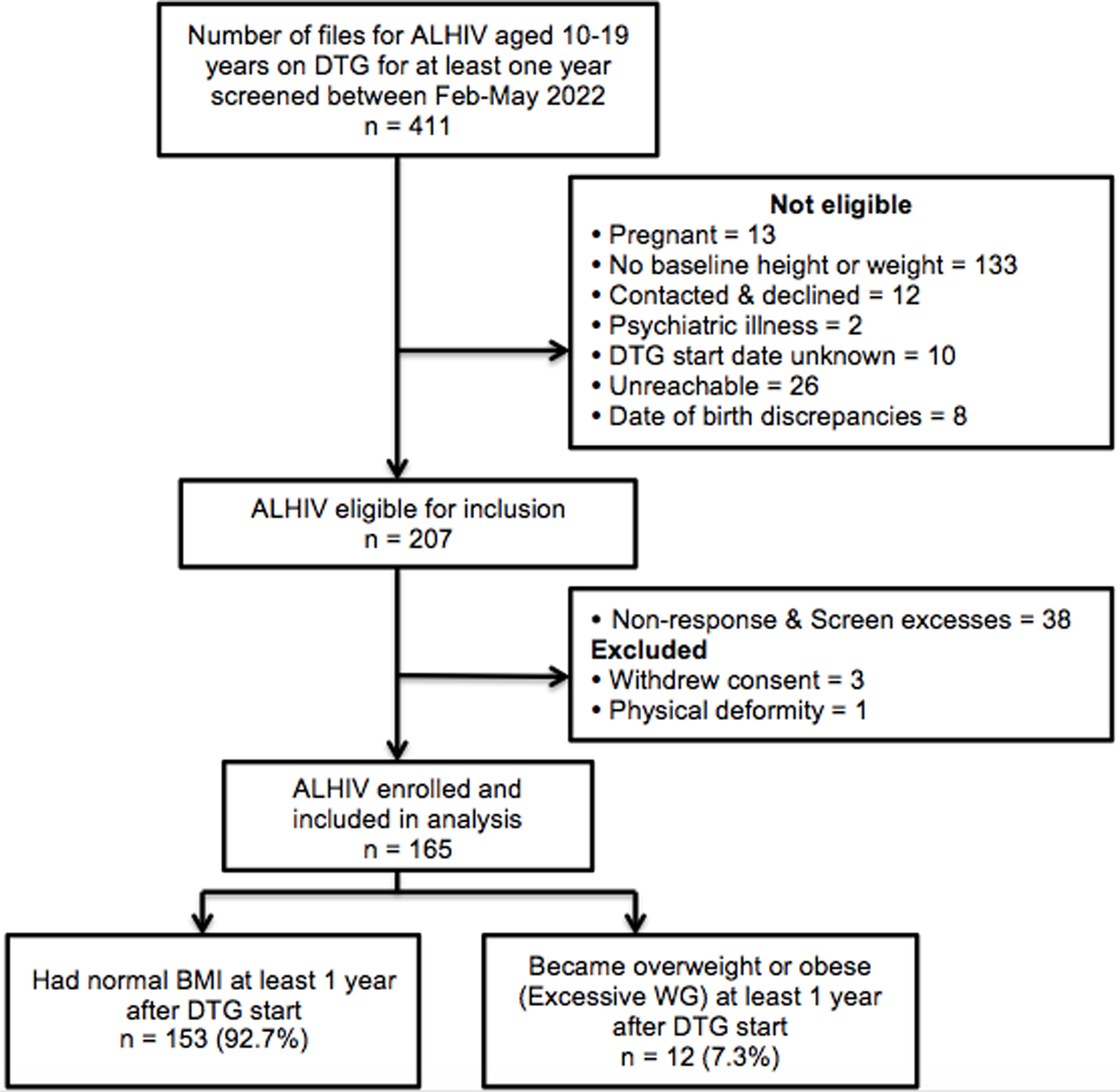








Forty-one PROUD participants were interviewed; 38 selected equally from the immediate and deferred groups and three additional interviews to explore underrepresented topics, including interviews with a trans woman, a person who seroconverted during the study, and a participant who decided not to start PrEP after the deferral period (Fig. 1).
Fig. 1
Purposeful selection of participants for IDIs based on trial arm allocation, risk behaviour and adherence
* One participant co-enrolled and in the main trial analysis is treated as being in the deferred arm to which they were originally allocated. However, they are treated as being in the immediate arm here as this was how they were selected for IDI
** Additional interviews were conducted with a trans woman, a person who seroconverted during the study, and a participant who decided not to start PrEP after the deferral period
At the time of interview, 33 out of 41 participants said they were or had been using oral PrEP. Thirty participants had been prescribed oral PrEP through PROUD and a further three participants had accessed oral PrEP privately: one had purchased oral PrEP in the USA and taken it prior to joining the study, and two had used oral PrEP during their deferred period of the trial (one by using the TDF/FTC from post-exposure prophylaxis [PEP] and the other by using TDF/FTC from an HIV-positive partner). Two participants prescribed oral PrEP in PROUD had discontinued it by the time of their IDI - one due to side effects and the other due to entering a monogamous relationship.
Duration of oral PrEP use ranged from one week to 32.8 months, with a mean of 14.3 months. Demographic characteristics of interviewed participants are presented in Table 1. Baseline data collection on sexual behaviour showed that, in line with the eligibility criteria, all IDI participants had engaged in condomless sex (39 as passive partner and 40 as active partner) in the 90 days prior to enrolling in the trial. The median number of anal sex partners at enrolment was 10, with an interquartile range of 3 to 20. Both the demographic and sexual behaviour data are also presented in qualitative studies analysing the same data published elsewhere [32, 33].
Table 1 Participant demographics at enrolment for IDIs (n = 41)The analysis generated eight themes, as depicted in Fig. 2, which can be categorised as relating to an impact on emotions and on behaviours. As the arrows in Fig. 2 illustrate, there was considerable interplay between psychological and behavioural impacts which are explored further within each theme.
Fig. 2
Psychosocial impact of oral PrEP use among PROUD participants
Psychological impact of PrEPReduced HIV-related anxietyNearly all participants mentioned that PrEP had reduced HIV-related anxiety both during and after sex, regardless of their risk level, age, or any other characteristic. The terms ‘peace of mind’, ‘reassurance’, ‘safety’ and ‘protection’ were regularly used by participants. For example, these participants described what they most liked about PrEP:
“It just takes away any possible worry afterwards, it’s just this protective bubble there” (Deferred, decreased risk, on PrEP, Brighton, aged 35–39).
“The best part of it actually is sex without fear, it really is” (Deferred, low risk, on PrEP, Manchester clinic, aged 25–29).
For many this effect was substantial, with participants describing the reduction in anxiety as ‘a feeling of relief’, ‘a weight lifted’, and ‘life-changing’. For some, this related to growing up during the early days of the HIV epidemic. However, younger participants also described how fear of HIV acquisition affected their sex lives:
“Before PrEP I’d have sex with condoms, it was just the way it was, but then I’d still have that extra level of anxiety if I got a cold afterward… in the past I would freak out about things and [PrEP] just gives me that extra level of security.” (Deferred, medium risk, on PrEP, Brighton clinic, aged 25–29).
Most participants attributed this reduction in anxiety to the additional security they felt PrEP gave them in reducing their risk of acquiring HIV or consequently passing it on to others. A few also attributed their reduced anxiety to more regular testing in addition to the added protection provided by PrEP:
“Regular testing provided me an extra level of worry-free-ness basically as well as the Truvada itself.” (Immediate, high risk, on PrEP, Sheffield clinic, aged 30–34).
Some participants in serodiscordant relationships highlighted that their PrEP use had the secondary effect of reducing anxiety for their HIV-positive sexual partners, either regular or casual. For one participant, PrEP provided the additional reassurance his partner, who was undetectable, needed to feel comfortable having condomless sex with him:
“It’s an absolutely terrifying thing for him to think that he might infect me. It’s his absolute worst nightmare… So, we’ve tried to be extra extra safe, and [PrEP] is the extra safe barrier if the condoms aren’t there.” (Immediate, increased risk, on PrEP, London clinic, aged 35–39).
Notably, participants did not have the same level of anxiety about STIs, which were largely seen as a treatable problem. A small number of participants highlighted that they were concerned about Hepatitis C, which mostly pertained to their use of sex toys and practices such as fisting. However, in most cases concerns relating to STIs were present prior to their use of oral-PrEP since participants were already exposing themselves to potential risk and this had not changed as a result of PrEP use.
Increased HIV prevention self-efficacyMany participants reported increased self-efficacy, describing PrEP as making them feel more ‘responsible’, ‘mature’, and ‘in control’ of their sexual health and sexual decision-making. Several participants said they no longer felt they were having to rely on their sexual partners being honest about their HIV status and instead were able to take responsibility for their own health:
“It does give me that extra peace of mind, I do feel in control, I feel that I’m not solely responsible in believing other people.” (Deferred, high risk, on PrEP, Manchester clinic, aged 35–39).
Many participants described how, prior to PrEP use, the conflict between their sexual desire to have condomless sex and their fear of acquiring HIV reduced their self-efficacy for HIV prevention. A small number of participants experienced this to such a degree that they felt it was inevitable that they would acquire HIV. By aligning HIV risk reduction with their sexual needs and desires, PrEP offered them an opportunity for agency over their sexual health:
“I thought I was likely to carry on putting myself at risk so, although I had an attitude where I didn’t care very much what happened, I thought well I don’t want to become positive and make life even more difficult than it is already, so I was glad to go on [PrEP].” (Immediate, decreased risk, on PrEP, London clinic, aged 45–49).
Practical aspects of taking oral PrEP also contributed to increased HIV prevention self-efficacy. Several participants highlighted that the choice to protect themselves from HIV was easier with daily oral PrEP than it was with condoms, since it is not coitally-dependent:
“It’s a decision I make when brushing my teeth not when I’m in the throes of passion, that’s a decision I can make every day, very clearly with no influence, no awkwardness, no risk of changing the situation, it’s there in the medical cabinet, it’s a no brainer. Using a condom before that, using a condom reliably was hit and miss for me, and this is a much easier decision to make, that I make alone.” (Immediate, high risk, on PrEP, London clinic, aged 40–44).
Reduced internalised stigmaMany participants expressed that PrEP had reduced the level of internalised stigma they felt around having and desiring condomless sex:
“It feels like a real privilege… and I feel hopeful that you can disassociate yourself from the sense of guilt” (Immediate, high risk, on PrEP, London clinic, aged 30–34).
Reduced anxiety and increased HIV prevention self-efficacy contributed to the lessening of internalised stigma due to putting themselves ‘at risk’ of HIV. For some participants, PrEP also helped to reduce the shame associated with the expectation of external stigma (from friends, prospective sexual partners, and clinicians) as they felt they had been proactive in reducing their HIV risk:
“I think it’s helped that I’ve been on PrEP - I’ve been able to say, I might not use condoms, but I have done something else. I think a lot of what I hear and see in other people is that ‘bad gay’ - it’s the shame that comes with not doing what we are told to do.” (Immediate, low/medium risk, on PrEP, London clinic, aged 30–34).
Others added that non-judgmental support from clinicians had also helped them to accept, be more honest, and feel less ashamed about their sexual behaviour:
“All of a sudden I have this [clinician] who not only seems to understand but also speaks to other people who are in the same situation as me, so I don’t feel alone anymore. I felt so alone before, I felt like I was the only person who felt like this or wanted to do these things, and all of a sudden I have this release, there is a definite case of psychological release with it.” (Deferred, increased risk, on PrEP, London clinic, aged 25–29).
Social norms around the importance of condom use and practicing safer sex within the gay community were repeatedly referred to by the participants. They noted that PrEP disrupted these social norms by removing HIV risk from condomless sex, with one participant describing this as making ‘the unthinkable [desire to have condomless sex], thinkable’. For some, this disruption of social norms had been instrumental in them feeling less shame and guilt around their sexual behaviour:
“Because the person I was before had had bareback sex but it was in a relationship and it was this kind of… enshrined thing, it wasn’t something that was tangible and acceptable it was really taboo and we’ve broken down that taboo now.” (Immediate, high risk, on PrEP, London clinic, aged 30–34).
However, despite the challenge that PrEP presents to existing social norms, many participants continued to describe themselves as ‘promiscuous’ or a ‘slut’ when discussing their sexual behaviour. Although some reclaimed these terms as a way of subverting their power (such as when one participant described himself as ‘a prime example of a Truvada whore’), it was clear that others still perceived having sex with more people as something negative despite enjoying the improved self-efficacy that PrEP has given them:
“PrEP has allowed me to be a bit more I suppose promiscuous but also feeling responsible at the same time and I know that sounds like a double negative.” (Deferred, high risk, on PrEP, Manchester clinic, aged 35–39).
Increased sexual pleasure and intimacyMany participants described how they were enjoying sex more as a result of using PrEP. By reducing anxiety and internalised stigma, and increasing self-efficacy, PrEP allowed participants to be more present in their sexual encounters and more focused on their pleasure and that of their partner(s):
“I just enjoyed the moment a lot more and to me it made a difference because it meant that it was a lot less worry for me at the time. I was more concerned about my own partner’s pleasure than I was concerned about what I was going to have to worry about afterwards.” (Immediate, high risk, on PrEP, Sheffield clinic, aged 30–34).
A number of participants commented that PrEP increased intimacy and emotional closeness with sexual partners. For some, this was because they experienced condoms as a barrier to intimacy, and PrEP enabled them to have condomless sex where they would not have done so previously. For others, it was because they were no longer distracted by HIV-related anxiety during sex and were instead better able to focus on being intimate with their partner.
“I think [my sex life] is the best it’s ever been to be honest… it’s the most intimate it’s ever been.” (Deferred, low risk, on PrEP, Manchester clinic, aged 25–29).
A few participants highlighted that they had entered relationships for the first time in their lives since they started using PrEP. While some felt this was coincidental, others credited it to the greater intimacy that they were able to have with sexual partners due to using PrEP.
“I mean maybe I was at a stage in my life anyway where I was ready to try and have a relationship. But I think there was something about the fear and the terror that was taken out of sexual contact that enabled more and repeated intimate contact.” (Deferred, high risk, on PrEP, Sheffield clinic, aged 20–24).
Internal conflictFor some participants, it was clear that despite the benefits PrEP provided, it was also a source of internal conflict with a number describing PrEP as a ‘double-edged sword’. While a few attributed this to concerns around STIs and ongoing HIV risk, the remainder appeared to feel conflicted about the sex they were having because they felt using condoms was the ‘ideal’ way to prevent HIV acquisition:
“I don’t know. The ideal I suppose is that we’d be having protected sex [with a condom], regardless. Would I wish for it? I don’t know, I don’t think so.” (Immediate, increased risk, on PrEP, Sheffield clinic, aged 40–44).
“I know [using PrEP] is not necessarily the best way of going about things, but if you’re gonna… put yourself in any danger it’s better to have that extra protection” (Deferred, medium risk, on PrEP, Sheffield clinic, aged 35–39).
A few participants felt that PrEP had contributed to a loss of self-control (in contrast to most participants who experienced an increase in self-efficacy) with regards to condom use or their sexual behaviour. For example, this participant initially described how he felt disempowered by PrEP as the removal of HIV risk made it harder to motivate himself to use condoms, although he later said that ‘disempowered’ was too strong a term:
“I felt disempowered, I felt I’d lost the control… it was becoming a case of the condom use was becoming less and less. I decided that what I needed to do was take myself away so that I can rebuild the thought processes in my head so that I could start to say no I’m going to start to use condoms again.” (Deferred, high risk, on PrEP, Manchester clinic, aged 45–49).
Despite the internal conflict described in this section, the majority of participants who felt this way maintained their PrEP use. Notably, the participant who chose not to take PrEP when offered explained his decision was due to concerns about PrEP stigma and being perceived as someone who engages in ‘high risk behaviour’. A few participants described how this internal conflict led to them considering a break from taking PrEP to compel them to use condoms or reduce their sexual activity, but at the time of interview none had actually gone through with this:
“In some ways I’ve thought to myself maybe I should come off [PrEP], because then I’d have to go back to that chain of thought that I should be using condoms all the time.” (Deferred, high risk, on PrEP, Manchester clinic, aged 45–49).
Behavioural impact of PrEPGreater sexual freedomApproximately half of participants noted that PrEP hadn’t changed their sexual behaviour particularly, it had just made them feel more comfortable and less worried about it. But for some participants, PrEP had enabled them to have sex that they would not have had previously. This included condomless sex with HIV positive partners (who mostly had undetectable viral loads), increasing the frequency and number of their sexual partners, and participating in group sex, amongst other activities. These participants tended to describe these experiences as liberating and fulfilling:
“The benefit was to have uninhibited sex as much as I wanted, where I wanted, when I wanted.” (Immediate, low risk, on PrEP, Manchester clinic, aged 40–44).
“The whole experience has really made me quite I suppose liberated, promiscuous, but also feeling in control and educated” (Deferred, high risk, on PrEP, Manchester clinic, aged 35–39).
Participants also described that by enabling them to have the sex that they wanted, PrEP allowed them to safely pursue their sexual fantasies and desires without putting themselves at risk of HIV:
“I’m having better sex and more of the sex I want. I wanted to explore the wild sex scene that cities like London and Berlin have to offer - but I’m beginning to lose interest in the scene now after about a year and a half… I guess there is a fantasy about quantity but it isn’t always better - but I wanted to try it so I just did it.” (Immediate, increased risk, on PrEP, London clinic, aged 40–44).
However, as noted above, a few participants felt discomfort with the greater sexual freedom that PrEP afforded them, particularly in relation to increased condomless sex.
Reduced harmful drug useJust under a third of participants had engaged in chemsex in the 3 months prior to enrolment (see Table 1). In the IDIs, participants were asked more generally about their drug and alcohol use, including during chemsex. Several participants explained that they had previously used drugs and alcohol to reduce their anxiety around condomless sex and repress feelings of shame and guilt. In these cases, participants described their drug use as ‘self-destructive’ or ‘self-harm’. Most described a reduction in harmful drug use due to changes in circumstances and accessing psychological support. However, one participant directly attributed their reduced harmful drug use to PrEP’s removal of anxiety and shame around sex, since it was no longer a prerequisite for them to have uninhibited condomless sex:
“It was easier before to get drunk or take drugs, have unprotected [condomless] sex and then never speak to the person again and feel less able to worry about it, but still worry about it hugely - to then, not feeling anxious around sex, to be able to have intimate sex with people, to not need huge amounts of sex and drugs.” (Deferred, high risk, on PrEP, Sheffield clinic, aged 20–24).
In contrast, participants who did not experience their drug use as harmful reported that their drug use during sex remained the same, with PrEP simply enabling them to reduce their HIV risk while doing so. These participants described how recreational drugs helped them reduce their inhibitions during sex and enjoy increased pleasure and intimacy:
“I nearly always use mephedrone or perhaps occasionally ketamine. It makes me feel very relaxed, sexual, much more intimate with people and less inhibited in my interactions with them.” (Immediate, decreased risk, on PrEP, London clinic, aged 45–49).
However, one participant who had not yet started PrEP expressed concern that he would increase his drug use once PrEP removed the risk of HIV:
“I guess my worry is that PrEP will increase my drug usage… That risk of acquiring HIV limits how often I do [chemsex] right now to maybe once a month or something.” (Deferred, increased risk, not on PrEP, London clinic, aged 35–39).
More protective sexual health behavioursSome participants described how the reduction in HIV-related anxiety and internalised stigma following PrEP use helped them develop a healthier, more positive attitude to sex and consequently reduced their sexual activity:
“One of the impacts is that there has been an aspect of normalisation of my sex, which is because it became so stress-free so worry-free, in fact one of the aspects of PrEP is I have less sex, so instead of having these highly problematic sexual behaviours, I still have them, but I think I have calmed down about sex and I have less of them” (Immediate, low/medium risk, on PrEP, London clinic, aged 45–49).
Others noted that PrEP had reduced their use of sex as ‘self-harm’ by breaking the link between sex and danger:
“I used to call it pressing the ‘fuck it’ button, just going off and doing whatever, if I’m doing something for risk… and I did things, like I did do, because I think I’m worthless, then PrEP made that not dangerous, so why bother?” (Deferred, low risk, on PrEP, Manchester clinic, aged 25–29).
Several participants credited the information and counselling they received during clinic visits for improving their confidence about the sex they have and their ability to negotiate condom use:
“I think I’m slightly better than I used to be at using condoms, using them without discussing it, just taking control of that. But I don’t think that’s related to being on the trial or medication - I think it’s from coming [to the clinic] and discussing risks regularly.” (Immediate, increased risk, on PrEP, Sheffield clinic, aged 40–44).
They also felt that the regular visits, risk counselling, and testing supported them to be more proactive in caring for their sexual health:
“PROUD is good because it keeps me having my regular checks - before I joined PROUD, I’d only come to the clinic once a year.” (Deferred, increased risk, not on PrEP, Sheffield clinic, aged 25–29).
“I’m much more aware of the risks now of having unprotected [condomless] sex with people who say they are negative but actually haven’t tested for a long time. I think coming in to see somebody regularly has made me think more about what I do and why I do it.” (Immediate, decreased risk, on PrEP, London clinic, aged 45–49).
留言 (0)