
記住我
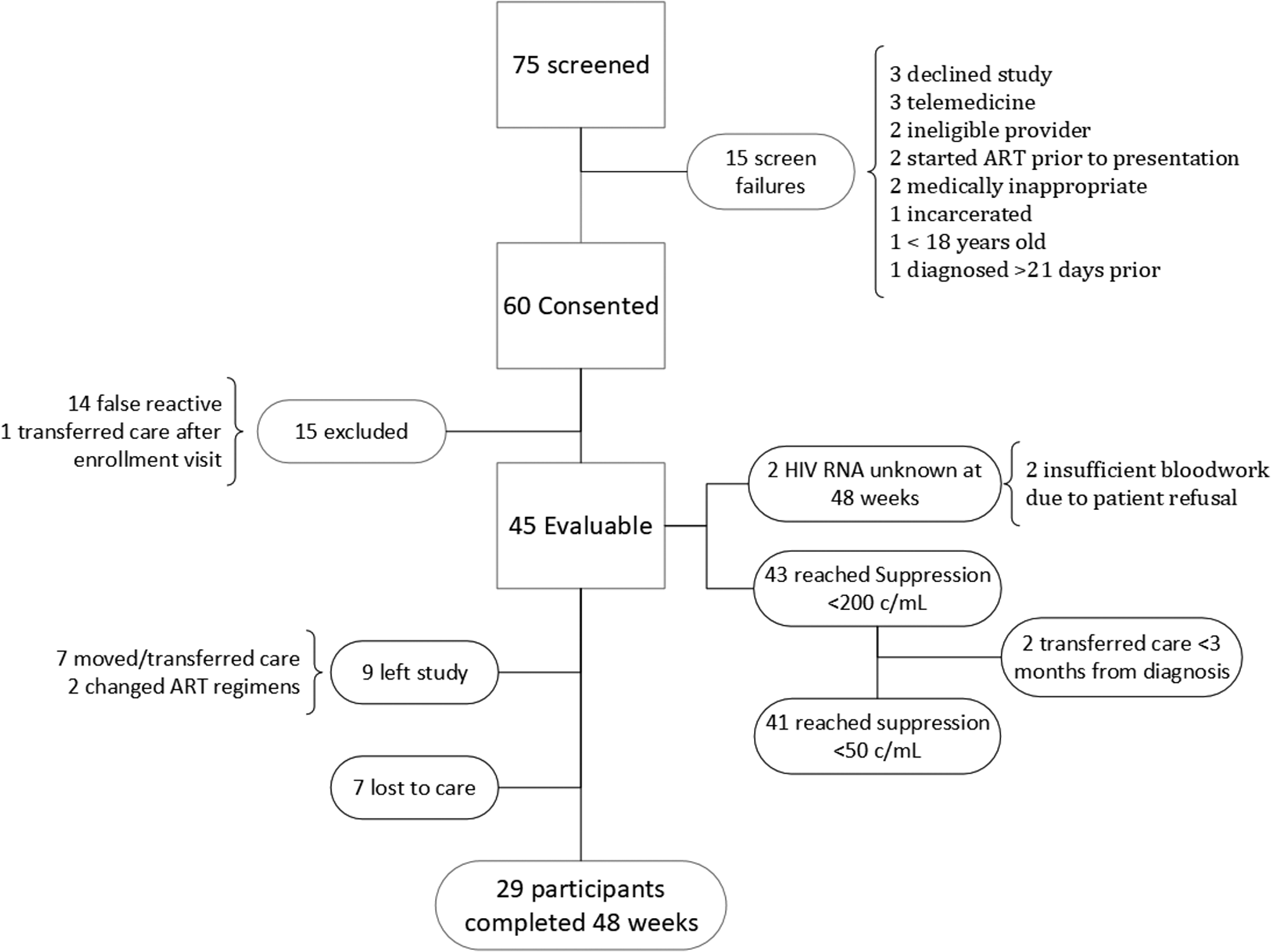








In its first year, Homecare enrolled 34 PLWHIV previously lost-to-follow-up in clinic-based care. The majority identified as African American (n = 31) and male (n = 26). After one year of enrollment, 31 were retained in care with at least 2 medical visits. Additionally, 28 Homecare participants achieved viral loads < 200 copies/mL at least once during fifteen months of follow up.
Table 2 displays interview participants’ demographic characteristics and their perceived barriers to care. The participants’ median age was 42 and 80% were male. Participants had been living with HIV for a median of 10 years and had been in Homecare for a median of 631 days.
Table 2 General Characteristics of Interview Participants enrolled in HomecareResults from eight categories of the Brief-IPQ before and after participation in Homecare are shown in Table 3. Means were significantly decreased (all p < 0.05) for the domains: emotional response, consequences and identity. PLWHIV reported HIV affecting them less emotionally, having less impact on their daily life, and experiencing fewer health sequelae after being enrolled in Homecare. Means were significantly increased (all p < 0.005) for the domains: personal control, treatment control, and understanding of HIV. PLWHIV reported more personal control over their HIV treatment, greater appreciation for the benefits of treatment, and better understanding of HIV in general after Homecare.
The domains timeline and concern did not show statistically significant results. Almost every PLWHIV always knew that HIV was a life-long diagnosis that could not be cured. Concern over HIV status was variable – some PLWHIV coped through repression before Homecare and grew more concerned of HIV as they began to acknowledge, accept, and appreciate treatment management; and others became less concerned through Homecare because they gained a better understanding of their health status and concrete steps to becoming virally suppressed.
Table 3 Brief Illness Perception QuestionnaireQualitative results – interview findingsInterview findings were organized conceptually into three categories: (1) social support and stigma reduction, (2) removing physical and resource barriers, and (3) changing perceptions of illness. Categories one and two are represented below with quotes from PLWHIV and their healthcare workers. The third category is incorporated in the mixed methods results, with interview findings presented in Fig. 1.
Fig. 1
A and B: Joint display. Illness perceptions before and after enrollment in Homecare are presented in box plots, showing median (central line), interquartile range (box), range (whiskers), and outliers (open circles). Quotes displayed below illustrate Homecare participants’ explanation for changing perceptions. 0 indicates lowest perception, 10 indicates highest. See Appendix 1 for B-IPQ
Social support and stigma reductionUpon receiving diagnosis of HIV, many PLWHIV enrolled in Homecare experienced some form of rejection from family and/or peers.
“There wasn’t anybody I could talk to. I tried to tell my family and they ostracized me.” (PLWHIV, Male, Age 71).
Some chose not to disclose their status to anyone or to only very select people in their life for fear of causing their loved ones excessive worry or burden.
“I haven’t gotten to the point where I feel comfortable with exposing it because I haven’t fully 100% accepted it.… I don’t want my children to get something to worry about, give my ex-wife something to worry about. That’s just between me and God…. I don’t want that to be something that someone else has to go through…. That’s my actions, that’s my results…. So, nobody else has to share that debt but me.” (PLWHIV, Male, Age 46).
This limited or nonexistent support network meant that PLWHIV were entirely responsible for enrolling, navigating, and maintaining their healthcare. Additionally, PLWHIV described feelings of shame associated with their status as they faced challenges with perceived stigma which made them want to push others away.
“I still felt like an outcast because…people try to hide it, but I see it…. This is something I have to deal with…. So, I just started using it as a weapon to keep people away…. People when they come up to me, especially guys, the first thing that come out my mouth, ‘I got HIV’…. It’s a defense mechanism for me. It just keeps a lot of people away.” (PLWHIV, Male, Age 46).
Building relationships with healthcare providers was often complicated by a lack of continuity of care, and the strain of having to repeatedly explain their social and medical histories to new providers.
“When I was in the clinic, I had probably seen about four different doctors. I had to keep – it was like ‘so, what happened, what happened’ – I had to keep talking about a traumatic experience over and over and over!” (PLWHIV, Male, Age 21).
Interactions with healthcare staff were, for many, one of the very few or only outlets PLWHIV had to discuss their HIV status openly. Some PLWHIV interviewed had good working relationships with their clinic-based providers, but others had difficulty forming a trusting bond.
“I had several doctors that I just did not like. They had poor bedside manner. It was just like a matter a fact thing for them. Like, dude I think I’m dying. You know one of those ‘should’ve-known-better’ attitudes.” (PLWHIV, Male, Age 57).
In contrast to clinic-based care, relationships with Homecare workers were perceived as consistent and widely praised as uplifting, warm, and non-judgmental.
“I just felt like it was a routine [at the clinic]…. Just another guy with HIV. With them [Homecare workers], they make you feel a little more like they understand. They can talk to you. It’s about having that one on one, not being the next one.” (PLWHIV, Male, Age 46).
Homecare workers were seen by participants as helping them focus on self-reflection and life goals not only for their health, but for their future as well.
“I took it a lot more serious, ‘cause it was a lot of conversation, not just a whole bunch of medical conversation. It was conversation about my life. Um, what do I want to do in the future. So having these types of conversations of what I want to do in the future, I had to be healthy to do these things.” (PLWHIV, Male, Age 29).
The quarterly community meetings, where individuals in the program could gather for food, conversation, and a guest speaker, also contributed to this sense of shared experience, community, and support:
“It just keeps you motivated to, like, help other people. Encourage other people. When you sit around these people. You build relationships. I still talk to a few of the guys outside of it. And…you need a support system outside of it.” (PLWHIV, Male, Age 29).
Homecare workers discussed the role of cultural humility in the program, and the need for empathy, understanding, and shared experience to foster strong relationships with PLWHIV.
“When people are even thinking about starting a program like this you have to consider the population that you’re dealing with. You have to get people who are culturally sensitive to that population, people who may be accepted….” (Homecare worker, Female, Age 43).
There were negative opinions shared by three PLWHIV interviewed. Two individuals were disappointed there were not more opportunities for peer interaction through the Homecare program. One individual was disappointed with the length of time between appointments after he achieved viral suppression and hoped to see Homecare staff more frequently.
Removing physical and resource barriersLack of transportation was a barrier to care for 73% of PLWHIV. Additionally, 40% noted work obligations, and 13% reported childcare responsibilities as other barriers to care. Most PLWHIV interviewed could arrange for medical transportation services to their clinic appointment, but many described these services as unreliable.
“You have the medical transportation, you know. Sometimes they come, sometimes they don’t. Or sometimes they come after your appointment time….” (PLWHIV, Male, Age 41).
Entering the clinic itself was a barrier, as worries about privacy and confidentiality were troubling for many PLWHIV. This was compounded by the fact that wait times were often long, and PLWHIV were left sitting in open spaces.
“Before I was always paranoid when I would go to the clinic. Who will see me? And if I see someone, I know I’ll try to hide and be isolated or I’d constantly be going to the bathroom….I remember telling the lady at the counter once, when y’all ready for me can you just call me on my cell phone. Don’t announce my name.” (PLWHIV, Male, Age 33).
In contrast, Homecare workers were described as punctual; they came directly to the PLWHIV’s home – eliminating several barriers described above.
“They [Homecare workers] come to my house. They’re ready to go. If I go to the clinic… when I get there, they’re ready to see me or I might have to wait…. You know, a reasonable amount of time [would be] 5–10 minutes, but an hour? Come on…” (PLWHIV, Male, Age 57).
Homecare providers commented on the value of additional time for environmental home assessments to connect PLWHIV to community resources. As described by a Homecare worker:
“For a new patient [an appointment could] be like an hour and a half to two hours because you’re not just in there for the patient assessment. You’re in there doing a whole environmental assessment also because do they have water, do they have heat, do they have a bed, do they have the necessities that they need because that’s where I touch base with the community organizations, request a bed, request a refrigerator…” (Homecare worker, Female, Age 49).
Mixed methods resultsFigure 1 A and Fig. 1B show a joint display analysis of the Brief-IPQ, with box plots displaying Likert scale results and representative quotations for each domain. We included the exact questions we asked PLWHIV and their responses. Both quantitative and qualitative findings provided evidence that participation in Homecare improved PLWHIV’s ability to reach virologic suppression, remain in care, and positively impact perceptions of illness, including emotional responses to HIV. Additionally, the impact of HIV on daily functioning was significantly reduced, including reductions in negative health consequences. This is shown through direct quotation and Brief-IPQ results. Through Homecare, PLWHIV changed their framework of control, shifting to a person-centered approach to managing their healthcare plans. PLWHIV improved their understanding of the scientific intricacies of HIV care, such as medication resistance and markers of immune function. Moreover, they accepted their treatment’s vital role for their physical health and survivorship. The conceptual framework in Fig. 2 displays obstacles and barriers that contribute to PLWHIV becoming lost-to-follow-up and how the Homecare program mediates their return to care. Quantitative and qualitative data were complimentary, showing significant results in the Brief-IPQ with concordant direct interview quotations, and both were considered to build this framework.
Fig. 2
Conceptual framework. Based on qualitative and quantitative data presented in the results section, Homecare mediates return to and maintenance in care for lost-to-follow-up people living with HIV
留言 (0)