INTRODUCTION
The sport of boxing consists of participants enduring repeated blunt force trauma to the head and body. Trauma inflicted to the cranium has led to an array of acute, subacute, and chronic neurological and neuropsychological complications, as well as death in the ring. Despite this, the safety of the participants had not been a concern until 1866 when rules banned the use of spikes on the gloves, introduced weight categories, and the 10-second knockout rule.1 The rules were further amended in 1987 by the World Boxing Association. The association reduced the maximum number of rounds in a match from 15 to 12, due to the death of lightweight boxer Duk Koo Kim, who died from acute neurological complications. The cause of death was most likely from an accumulation of blows ending with a knockout. However, in the modern era of boxing, the occurrences of neurological injuries have declined further because of expanded and improved medical and safety precautions, along with more efficient monitoring. Despite these improvements, the risk of traumatic brain injury/injuries (TBI) continue. Research published by Jordan et al2 observed that approximately 20% of professional boxers develop a chronic traumatic brain injury (CTBI) during their careers, and up to 40% of retired professional boxers were diagnosed with symptoms of chronic brain injury (CBI).3 Arguably, boxing's most famous practitioner, Muhammad Ali, is the most prominent example of an individual with a boxing-related neurological injury. Ali was diagnosed with the neurodegenerative disorder, Parkinson disease (PD) in 1984, which later contributed to his death in 2016. According to Baird et al,4 between 1950 and 2007, there have been 339 deaths in professional boxing. In addition, in 2013, the International Boxing Association (AIBA) faced controversy over the changes in the rules in amateur boxing disallowing male senior boxers (participants older than 18 years old) to wear headguards during their bouts. This resulted in controversy due to the increased awareness of head injuries, in conjunction with concussion awareness in sports generally.5
A TBI is characterized as a blow or impact to the head interrupting the brain's normal function. Most TBIs are a direct result of the “acceleration-deceleration mechanism.”6 It may occur when the skull has been abruptly and violently struck by an object or when an object has cracked the skull and penetrated the brain tissue.3 A TBI can be categorized as an mild TBI generally known as a concussion ranging from grade 1 to grade 3 or a CTBI that can be classified as chronic traumatic encephalopathy (CTE).7 Concussions display almost an instantaneous and short-term reaction from the brain in response to trauma.8 This display of concussion is usual but not always the case. A CTE is defined as a neurodegenerative disease that can manifest years after the initial incident.9 This can result in physical shrinking of the brain, which can lead to neurological disorders such as Parkinson disease (PD), dementia, stroke, epilepsy, and seizures.10 In terms of what is observed postmortem, observations from emerging data suggest that moderate and severe TBIs exhibit a dose–response trend as risk factors for neurodegenerative diseases, including cerebral atrophy.11,12 In up to 30% of patients who died following a single TBI, the pathological findings showed the presence of diffuse axonal injuries and depositions of amyloid-β aggregates.13–16 In addition, even a single TBI could induce progressive tau pathology for years after the initial injury, particularly in the presence of diffuse axonal injuries.17
Knockouts (KO) are the most common causes of acute neurologic injuries in boxing and are responsible for approximately 10 boxing deaths per year.18 The loss of consciousness generated by a knockout punch is sudden in onset and generally temporary in duration. A KO is commonly due to a direct and clean strike to the face or jaw, resulting in an acceleration or torque rotational force, which is transferred to the brain. This impairs the cerebellum and brain stem, resulting in imbalance and unsteadiness causing the fighter to be incapable of posture control and defense.19 Some boxers encounter persistent residual cognitive and physical symptoms, such as temporary short-term memory loss, dizziness, difficulty balancing, and headaches for days or weeks following a boxing bout. This is known as postconcussion syndrome (PCS) or “groggy state.” Boxers regularly appear to recover symptomatically and return to their previous physical and cognitive state. However, boxers with longer and intense careers encounter prolonged durations of symptoms. In addition, when PCS becomes more frequent and increases in duration, the risk of chronic problems, including the progression of CTE can occur.20
Chronic traumatic brain injury or CTE in boxing, also referred to as “being punch drunk” or “dementia pugilistica,” is believed to be the most severe health issue in modern boxing.21 Chronic traumatic encephalopathy is characterized by a mix of gait and speech disruptions, pyramidal tract dysfunction extrapyramidal features, biochemistry disorders, behaviour or personality changes, and psychiatric disease.22 In addition, motor impairments consisting of parkinsonism, hyperreflexia, dysarthria, spasticity, and cerebellar ataxia have also been recorded.23 The distinct neuropsychiatric symptoms include childish behaviour, rage reactions, and mood swings. Chronic traumatic encephalopathy develops slowly or emerges after a brutal bout and typically occurs at the end of a boxer's career or quickly following retirement.1 In addition, neuropsychological examinations have reported a deterioration in memory, processing information, attention span, and execution of basic functions.24–26 In the infancy phase of CTE, the symptoms are sometimes temporary and reversible. However, as the neurodegenerative disease progresses, the symptoms become more severe. The pathology of CTE consists of pigmented cell loss, cerebellar tonsillar scarring, cerebral atrophy, cavum septum pellucidum (CSP), and neurofibrillary tangles.27 However, the neuropathology of CTE can only be conclusively determined during a postmortem neuropathological examination.28 In addition, there are no International Consensus Criteria or biomarkers of disease that exist and may be used to assist in the clinical examination and determination of CTE.29,30
In boxing, the headguard is worn during sparring and previously during amateur boxing bouts. The utilization of headguards in amateur boxing was first introduced in 1984, with the purpose of preventing and decreasing the chances of superficial injuries such as cuts, rather than trauma to the brain.31 The aim of amateur boxing was to outstrike the opponent. Points are awarded for the volume of punches accurately landed on the opponent. These rules were introduced to limit blows and injuries to the head; the body was targeted due to its large surface area, and the headguards and gloves used were heavily padded.32 However, as previously mentioned, the AIBA prohibits the use of headguards in competitions. As a result, concerns over participants' safety have increased because the incidence of cuts and brain injuries continue to rise.31
Therefore, the rationale and purpose of this systematic review and meta-analysis was to determine the overall long-term injury (ie acute and chronic) of the brain resulting from participation in the sport of boxing. The objectives consisted of analyzing and comparing data outcomes in regard to physical chronic brain abnormalities, such as brain atrophy, and CSP within a population of boxers, along with neuropsychiatric and neurological disorders, for example dementia, amnesia, PD, and ataxic gait impairments (AGIs). In addition, concussion rates between boxing and other combat sports, for example, karate and taekwondo, were compared and evaluated, as well as the safety and efficiency of headguards worn during boxing bouts.
METHOD
Search Strategy
This systematic review and meta-analysis used the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines (Figure 1). To summarize evidence relating to various head trauma within professional and amateur boxing, a search for relevant studies was performed in PubMed, Google Scholar, SAGE Journals, British Journal of Sports Medicine, Research Gate, and Science Direct using the key phrases of “Brain injuries within boxing” and “Efficiency of boxing headguards” from 1962 to 2020. The study included articles that were peer and independently reviewed, which reported data from cohort studies, case studies, or cross-sectional studies. Excluded articles consisted of data not published in English, conference posters, data from interventional studies, along with articles that contained boxing injuries that occur to the head or face, such as cuts or broken bones, and injuries or impairments to the brain that were not directly related to boxing.
;) Figure 1.:
Figure 1.: PRISMA Flow Chart showing the search procedures and outputs.
Eligibility Criteria
The initial abstracts were analyzed using the search engines using the following principles: (1) data reported on participants who were either current or former professional or amateur boxers. (2) The boxers had to have at least 5 bouts or career durations of at least 1 year. (3) Data focused on chronic physical brain abnormalities, neuropsychiatric impairment, and neurological impairments within a specific populace evaluated the efficiency of headguards within boxing or compared concussions within boxing with other combat sports.
Eligibility Criteria Rationale
The rationale for the included studies was to execute the objectives of this study, which were to investigate injury to brain in the sport of boxing. Therefore, the participants within the studies were either current or former amateur or professional boxers. The purpose of having a boxing population was to evaluate the risk ratio (RR) of chronic physical brain abnormalities, neuropsychiatric impairment, and neurological impairments within a specific populace, along with evaluating the efficiency of headguards within boxing. This could be completed by comparing the RR of wearing and not wearing a headguard in amateur boxing bouts and sparring. Furthermore, the rationale of comparing the occurrence of concussions between boxing and other combat sports was to determine the safety of boxing by analyzing and contrasting the rate of concussion per 100 participants.
Exclusion Criteria
To determine any prejudice with 1 or more published sources, the Cochrane Risk of Bias Assessment Tool (Supplemental Digital Content 1, https://links.lww.com/JSM/A396) was used. Any sources that were identified as having bias were excluded.
Data Extracted
The data extracted included the year of publication, main author/s, study design, populations' training status (amateur or professional), activity type (sparring or bouts), the number of participants, brain injuries sustained, specific anatomical location within the brain (cerebrum, cerebellum, frontal lobe), and the type of neurological or neuropsychological impairment. The outcomes incorporated included physical chronic abnormalities of the brain, neuropsychiatric disorders, and neurological disorders sustained in amateur or professional boxing, in addition to the safety benefits of boxing headguards. These outcomes were then compiled into tables. The data and references obtained were then implemented into the Review Manager 5.4 software (Cochrane Rev Man, Copenhagen, Denmark) to analyze odds ratios (ORs).
Search Results
From the 6 search engines, a total of 52 335 results appeared, and 84 were shortlisted as potentially relevant to this review (Figure 1). After critical evaluation using the relative key phrases, 35 out of the remaining studies with full text were obtained and evaluated, which were then incorporated into this review.
Statistical Analysis
Review Manager 5.4 software (Cochrane Rev Man, Copenhagen, Denmark) was used to accumulate and process all the statistical data from the selected studies. The overall pooled effect was calculated using a fixed-effects meta-analysis method available in Review Manager 5.4 software (Cochrane Rev Man). The data type was dichotomous, and the effect measures were OR, and RR. The fixed-effects method applied was the Mantel–Haenszel (M–H).33 For the meta-analysis, the fraction of variance due to heterogeneity was estimated by the statistic I2. The bias of I2 was calculated by considering whether the number of studies in the meta-analysis was small, that is, based on the Cochrane Library, the median number of studies per meta-analysis is 7 or less.34 T-tests were also performed to analyze and determine the variation and significance between the comparisons.
Patient and Public Involvement
This is a systematic review and meta-analysis study; therefore, patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
RESULTS
Physical Chronic Brain Abnormalities Because of Boxing
From the 35 studies selected for this review, only 12 were declared suitable in providing sufficient information relating to physical chronic brain abnormalities due to boxing (Table 1).
TABLE 1. -
Overview of all Selected Studies on the Chronic Physical Abnormalities of the Brain Because of Amateur and Professional Boxing
Author (yr)
Data Type
Purpose
Participants' Background
Methods of Measurement
Findings
Lee et al (2020)
Case study
Determine whether combat sports (boxing and martial arts) with CSP and CV possess decreased volumes in brain structures and worse clinical outcomes on mood and cognitive testing
Fighters: 476 (440 male, 36 female. Age: 30.0 ± 8.2 years [range: 18-72 year old])
Control: 63 (57 male, 6 female. Age: 30.8 ± 9.6 years [range: 18-58 year old])
Data collected from 2011 to 2018 on active and retired professional fighters and healthy age-matched controls
All controls and fighters underwent MRI scans
Fighters who possessed CV obtain significantly lower mean psychomotor speed (estimated difference, −11.3; 95% CI, −17.4 to −5.2; P = 0.004) and lower mean volumes in the supratentorium (estimated difference, −31 191 mm3; 95% CI, −61 903 to −479 mm3; P = 0.05)
Longer CSPV length was associated with lower processing speed (slope, −0.39; 95% CI, −0.49 to −0.28; P < 0.001), psychomotor speed (slope, −0.43; 95% CI, −0.53 to −0.32; P < 0.001), and lower brain volumes in the supratentorium (slope, −1072 mm3 for every 1-mm increase in CSPV length; 95% CI, −1655 to −489 mm3; P < 0.001)
Fighters with lower WMC possessed lower cognitive complexity
Bernick et al (2015)
Case study
Investigate the relationship between exposure variables, cognition, and MRI brain structural measures in a cohort of professional combatants
Fighters: 224 (131 mixed martial artists and 93 boxers. Age: range from 18 to 44 years, median of 27.7 year old)
Control: 22. (age and gender was not described within this study)
MRI scans, along with cognitive function was assessed by a FES and a computer-based battery test that consists of 4 subtests of the CNS vital signs, including verbal memory, symbol digit coding, Stroop test, and a finger tapping test
Estimated reduction of brain volume for boxers relative to MMA fighters were 3.3% [P = 0.006] reduction on the thalamus, hippocampus reduction on the left was 2.0% and 4.2% (P = 0.007)
Estimated reduction of overall brain volumes per year: 0.5% for boxers
Jordan et al (1996)
Case study
Evaluate the neuropsychological impairments that professional boxers develop as a consequence of sparring
Professional boxers: 42 (age: 25.6 year old [Range 19-31 year old])
Total amateur bouts: 55.6 bouts [range: 2-266 bouts]. Amateur losses: 6.2 [range: 1-33 losses]
Total professional bouts: 10 bouts [range: 0-36 bouts]
Professional losses 3.1 [range: 0-15 losses]
Sparring exposure: frequency (d/wk): 3.6 days [range: 1-7 days]. Rounds per sparring session: 6.1 rounds [range: 2-12 round]
Total rounds per week: 22.7 rounds [Range: 4-56]
Sparring intensity (Marked on a scale of 1-4): 3.0 [Range: 2-4]
Each boxer underwent a CT scan, along with a battery of neuropsychological test. These consisted of estimates of general intelligence, language, constructional skills, memory, visual motor coordination and concept formation, cognitive stability, and flexibility planning
CT scans demonstrated that 17 boxers (40.5%) possessed borderline brain atrophy, 2 boxers had large abnormal CT scans, and 1 abnormal scan exhibited a focal hypodense lesion in the left frontal lobe that was consistent with posttraumatic encephalomalacia. In addition, another scan displayed cerebellar atrophy with an enlarged fourth ventricle, and 6 boxers possessed cavum septum pellucidum (CSP)
There was significant correlation in increased exposure to sparring and deterioration of neuropsychological functions (P < 0.05)
Casson et al (1984)
Case study
Examine the CTE effects boxing has on professional boxers at different levels (journey-men-champions), who have responsible jobs, secondary or college educations, and no history of substance abuse
Ex/professional and golden glove boxers: 18 (age: 36 ± 12.2 year old [range: 18-60 years old])
Total number of bouts: 88.2 ± 65.1 bouts [range: 7-240 bouts]
Losses: 9.75 ± 7.9 losses [range: 2-26 losses]
Length of career (years): 10.2 ± 5.5 years [range: 1-22 years]
Each boxer under a CT scan, an EEG, a formal neurological examination including mental status, and a battery of neuropsychological tests that consist of trail making test, the digit symbol test, the Wechsler memory test (including both verbal and visual memory), and the Bender Gestalt test
13 of 15 (87%) of ex and active professional boxers possessed abnormal results in at least 2 of the 4 tests (EEG, CT scan, neurological examination, and neuropsychological test battery). All 3 golden glove boxers obtained normal test results across the 4 tests
8 boxers had abnormal CT scans, 1 had cerebral cortical atrophy, 2 possessed central cerebral atrophy, and 5 had generalized cerebral atrophy. A cavum septum pellucidum was noted in 3 of these 8 scans
Ross et al (1983)
Case study
Examine the neurological status and CT appearance of brains' of exprofessional boxer
Exboxers: 40 (age: 46.8 ± 17.1 years old)
38 boxers underwent a CT scan, 24 boxers completed a neurological examination and an EEG, and 24 of these individuals also had a CT scan. CT scans were graded 0-4, 0 implied normal, and 4 implied most abnormal
The information gathered displayed a significant relationship between the number of bouts fought and CT changes (P = 0.0229), indicating cerebral atrophy. Positive neurological findings were not significantly correlated with the increase of bouts. EEG abnormalities were significantly correlated with the number of bouts (P = 0.0582)
Haaglund and Persson (1990)
Case study
To investigate possible chronic brain damage as a consequence of Swedish amateur boxing
Total number of former amateur boxers: 47 (22 boxers many bouts [HM], and 25 with few bouts [LM])
Age: 33 years old [range 25-44 years old]
Career length: HM: 8.3 years [range: 2-17 years]. LM: 3.4 years [range: 1-8 years]
Amateur bouts: HM: 54.3 bouts [range: 25-180 bouts]. LM: 5.5 bouts [range: 0-15 bouts]
Total number of control group: 50 (25 football players, and 25 track and field athletes.)
Age: 33 years old [range 25-44 years old]
All participants underwent EEG examinations, along with measuring brain electric activity mapping (BEAN)
No severe EEG abnormalities were identified in both boxing groups; BEAN findings were not significantly different from the control group. In addition, there were no neurophysiological variables that correlated with the number of amateur bouts, number of lost fights, or duration of a boxing career
Jordan and Zimmerman (1990)
Qualitative comparative analysis
Compare and analyze the differences between CT and MRI scans when examining 21 boxers
Total number of boxers: 21 (16 professionals, 4 amateurs, 1 retired)
Age range: 21-66 years old
All participants underwent both CT and MRI scans. CT and MRI scans were then evaluated and compared with each other
11 boxers had normal results on the MRI and CT scans; 7 boxers had abnormal results on the MRI and CT scans; 4 boxers possessed hypodense lesions on CT scans. Out of these 4 boxers, 1 boxer had a dilated sulcus in the left frontal lobe. Another boxer's CT scan demonstrated hydrocephalus and atrophy
Jordan et al (1992)
Case study
Analyze 338 active professional boxer's CT scans
Total number of boxers: 338 professional boxers
Age: range: 17-46 years old
All participants underwent a CT scan. CT scans were analyzed for the detection of any abnormalities
238 (70%) boxers had normal CT scans, 75 (23%) boxers displayed borderline CT scans, and 25 (7%) boxers possessed abnormal CT scans, 22 of these boxers had brain atrophy. 8 had ventricular atrophy, 6 possessed diffuse atrophy, and 3 boxers had focal lesions of low attenuation persistent along with posttraumatic encephalomalacia. There was no difference in scans between normal, borderline, and abnormal CT scans in regards to age, win/loss record, and number of bouts. Brain atrophy was acknowledged more often within boxers with a large CSP compared with boxers with a small or no CSP (P < 0.05). Boxers with abnormal or borderline CT scans who experienced a TKO or KO were slightly older than those with normal CT scans and a history of a TKO or KO (0 (P < 0.05)
Carsson et al (1982)
Qualitative short report
Evaluate the neurological effects of knocked out boxers
Total number of boxers: 10 professional boxers
Age: 24.9 ± 3.4 years old [range: 20-31 years old]
Number of bouts: 20.8 ± 16.3 bouts, [range: 2-52 bouts]
Losses: 3.9 ± 2.7 losses [range: 1-11 losses]
All participants under EEG and CT scans
From the information gathered from the CT scans, 5 (50%) of boxers possessed cerebral atrophy and 1 suffered from CSP. EEG scans displayed that 2 boxers had minimal abnormalities
Jordan et al (1992)
Cohort study
Evaluate potential brain injuries within boxing
Total number of boxers: 45 professional boxers
All participants underwent 2 CT scans with a period of 31.3 months [range: 15-48 months] in between scans
Baseline scan: 33 boxers possessed normal CT scan, 9 had borderline brain atrophy, and 1 had moderate-severe brain atrophy; 6 of these 10 possessed CSP, and 2 had focal lesions
Follow-up scan: 3 boxers displayed progressive CT changes. 31 boxers had normal CT scans, 10 possessed borderline brain atrophy, and 2 had moderate-serve brain atrophy; 9 of the 12 boxers possessed CSP, and 3 had focal lesions
Aviv et al (2010)
Case study
Identify the quantity and extent of a CSP among professional boxers
Total number of boxers: 164 boxers
Control group: 43 control participants
All participants underwent MRI scans
81 boxers possessed medium size CSP, and 13 boxers possessed large size CSP
Katse et al (1982)
Case study
Examine the neurological and psychological affect boxing has on the brain
Total number of boxers: 14 (8 amateur boxers, and 6 professional boxers.)
Amateur boxers: age: 31 years old [range: 19-53 year old]
Number of bouts: mean: 129 bouts
Losses: 28 losses
Professional boxers: age: 38 [range: 29-53 years old]
Number of bouts: Mean: 148 bouts
Number of losses: 35 losses
Each boxer had a neurological examination, and 12 boxers psychological examination. This included Wechsler adult intelligence scale and Wechsler memory scale. In addition, Wisconsin card-sorting test, trial-making test, Benton visual retention test, and the Purdue pegboard test were also incorporated; 6 boxers underwent an EEG (2 professional boxers, and 4 amateur boxers), and 5 boxers had a CT scan (4 professional boxers and 1 amateur boxer)
EEG results were abnormal for 6 boxers. Abnormalities were theta focus in 2 boxers, diffuse in 3 boxers, and paroxysmal theta in 1 boxer
CT scans displayed brain atrophy in 3 (50%) of the professional boxers, CSP was acknowledged in 2 professionals and 1 amateur
FES, fight exposure score; WMC, working memory capacity.
The results in Figure 2A indicate that only 23.30% suffered from CSP (i.e. 147 of 631 amateur and professional boxers). Figure 2B shows that 30.41% possessed some form of brain atrophy (i.e 125 of 411 amateur and professional boxers).
Figure 2.: Forest plot showing (A) CSP results in a boxing population and (B) brain atrophy results in a boxing population.
Chronic Neuropsychiatric and Neurological Disorders within Boxing
A total of 12 study types that provided adequate information in relation to chronic neuropsychiatric or neurological disorders in boxers is presented in Table 2.
TABLE 2. -
Overview of all Selected Studies on the Chronic Neuropsychiatric and Neurological Disorders Because of Amateur and Professional Boxing
Author (yr)
Study Type
Purpose
Participants' Background
Methods of Measurement
Findings
Johnson (1969)
46
Case study
Examine the neuropsychiatric effects of head injuries sustained in former boxers
Exboxers: 17 (16 professional and 1 amateur)
Age: 54 ± 8.5 [range: 35-64 years old]
Bouts: all participants had 200-300 bouts between them
Participants underwent EEGs, AEG, and cognitive assessments
11 exboxers possessed amnesia
3 suffered from dementia
5 had morbid jealousy
4 had rage reactions, generally accompanied with pathological intoxication, and 2 had psychosis
Cognitive assessments displayed slow information processing speed and memory difficulties
Jordan et al (1997)
21
Case study
Assess the relationship between CTBI and APOE genotype in boxers
Professional boxers: 30 boxers
Age: 48.9 ± 16.2 years old [range: 23-76 years old]
Bouts: 30.0 ± 36.8 professional bouts [ange: 0-162 professional bouts]
All participants underwent APOE genotyping, behavioural and neurologic examinations. APOE was examined in relationship of CTBI. A 10-point clinical rating scale (0-9), a CBI scale was created to monitor the severity of CTBI associated with boxing
11 boxers had normal CBI scores
12 displayed mild impairments
4 were moderately deficit
3 possessed were severely impaired
Boxers who had more with ≥12 professional bouts displayed significantly higher CBI scores than boxers with less than 12 professional bouts (P < 0.001)
All boxers who possessed a severe impairment possessed at least 1 APOE e4 allele. Findings indicate that boxers who possess APOE e4 allele and have more than 12 professional bouts may be more likely to suffer from server chronic neurologic deficits
Dominic et al (2017)
47
Case study
To determine the prevalence and elements of risk of PD within retired Filipino boxers
Exprofessional boxers: 21 exboxers
Age: 38.19 ± 2.75 years old
All participants were screened for PD through the utilization of the motor part of the MDS—UPDRS
17 (80.95%) of boxers possessed PD.
10 (58.82%) had asymmetric PD.
10 boxers (58.82%) suffered for PD within the upper extremities
6 (35.29%) suffered from PD within the upper and lower extremities, and only 1 (5.88%) had PD within the lower extremities
PD within boxers were significantly increased (P = 0.0480) with the number of losses, along with the number of knockouts suffered
Spillane (1962)
48
Observational study
Describe the neurological deficits of 5 exprofessional boxers
Exprofessional boxers: 5 exboxers
Age: 48.8 ± 11.8 years old [range: 33-69 years old]
Professional bouts: all boxers had more than 200 bouts each
All participants had a PEG, and 2 had neurological examinations
Boxer 1 possessed progressive dysarthria, ataxic gait, AD, impairment of intelligence. Pneumoencephalogram (PEG) findings displayed an absence of the septum pellucidum
Boxer 2 possessed progressive dysarthria, ataxia, right hemiparesis, right optic atrophy, and impaired intelligence. PEG displayed CSP.
Boxer 3 suffered from progressive dementia along with serve dementia, and ataxia tremors. PEG revealed CSP, and enlarged lateral ventricles
Case 4 possessed normal a PEG and neurological examination results
Boxer 5 suffered from progressively worsening dysarthria, dragged his left leg. Neurological examinations displayed no dementia, but poor concentration, and PEG was normal. An autopsy revealed mental deterioration due to the degeneration of the left cerebral and cerebellar hemispheres
Mawdsley, and Ferguson (1963)
49
Observational and case study
Examine the neurological diseases within boxers
Exprofessional boxers: 10 exboxers
Age: 55.9 ± 8.9 years old [range: 33-69 years old]
Professional bouts: 232.4 ± 175.6 bouts [range: 80- 600 bouts]
Every participant underwent clinical examinations
All boxers had some form of tremors, ranging from 1 limb to all 4, 8 exboxers possessed CSP
5 displayed EEG abnormalities
9 had abnormal AEGs
3 suffered from dementia
4 had grossly defected memories
6 had ataxic gaits and 8 had speech impairments, ranging from slurring words to dysarthria
Casson et al (1984)
38
Case study
Examine the CTE affects boxing has on professional boxers a different levels (journey-men-champions), who have responsible jobs, secondary or college educations, and no history of substance abuse
Ex/professional and golden glove boxers: 18 (age: 36 ± 12.2 years old [range: 18-60 years old])
Total number of bouts: 88.2 ± 65.1 bouts [range: 7-240 bouts]
Losses: 9.75 ± 7.9 losses [range: 2-26 losses]
Length of career (years): 10.2 ± 5.5 years [range: 1-22 years]
Each boxer under a CT scan, an EEG, a formal neurological examination including mental status, and a battery of neuropsychological tests that consist of trail making test, the digit symbol test, the Wechsler memory test (including both verbal and visual memory), and the Bender Gestalt test
5 boxers possessed abnormal neurological examinations and 3 suffered from a memory loss, disorientation, and confusion
1 exboxer had an impaired recent memory without any confusion or disorientation
1 exboxer had an organic mental syndrome, and 1 exboxer had cortical release phenomena
All boxers had abnormal Bender Gestalt test, verbal delay, verbal immediate results
11 boxers had visual delayed abnormalities
10 had abnormal trail making test results and 7 possessed abnormal digit symbol results
Drew et al (1986)
50
Case study
Examine the neuropsychological deficits in active professional boxers
Professional boxers: 19 (age: 23.4 ± 2.95 years [range: 18-25 years old])
Amateur career: 52.8 ± 55.98 bouts [range: 1-195 bouts]. Losses: 5.2 ± 4.7 [range: 0-15 losses]
Professional career: 13.7 ± 13.08 bouts [range: 0-37]. Losses: 3.8 ± 2.88 [range: 0-10]
Control: 10 (age: 23.9 ± 2.59 years [range: 19-28 years old])
QNST, the RMT, and the HRNTB. Subtests within the QNST involved rapidly reversing
Repetitive hand movements, finger to nose, thumb, and finger circle, tandem walk, and single foot stand. RMT was used to measure overall memory index. HRNTB consisted of subtest such as aphasia screening test, trails test, fingertip number writing
Seashore rhythm, tactile performance test (TPT), finger tapping, and category test
Boxers who possessed a higher number of professional bouts and losses had a higher correlation of memory, cognitive, sensory motor impairments, along with cerebellar vestibular dysfunctions
Brooks et al (1987)
51
Case study
Examine the neuropsychological affects within amateur boxers
Amateur boxers: 29 (age: 21 ± 3.1 years old. [range: 15-27 years old]); amateur bouts 26.2 ± 22.2 [range: 2-96]. Losses: 8.6 ± 7.4 [range: 0-32]
Control: 19 (age: 21 ± 3.0 years old)
Cognitive test procedures included 3 subtests that consists of learning and memory, information processing and motor skill, and intelligence
There was no significant differences between the boxers and control group in terms of verbal intelligence, nor was there any significant predictors of impaired cognitive performance
Kaste et al (1982)
45
Case study
Examine the neurological and psychological affect boxing has on the brain
Total number of boxers: 14 (8 amateur boxers, and 6 professional boxers.)
Amateur boxers: age: 31 years old [range: 19-53 years old]
Number of bouts: mean: 129 bouts
Losses: 28 losses
Professional boxers: age: 38 [range: 29-53 years old]
Number of bouts: mean: 148 bouts
Number of losses: 35 losses
Each boxer had a neurological examination, and 12 boxers psychological examination. This included Wechsler adult intelligence scale, and Wechsler memory scale. In addition, Wisconsin card-sorting test, trial-making test, Benton visual retention test, and the Purdue pegboard test were also incorporated; 6 boxers underwent an EEG (2 professional boxers and 4 amateur boxers), and 5 boxers had a CT scan (4 professional boxers and 1 amateur boxer)
One professional boxer had abnormal neurological results, apraxia and slight unsteadiness, along with slight slowness and uncertainty in mental functions
EEG results were abnormal for 6 boxers
Abnormalities were theta focus in 2 boxers, diffuse in 3 boxers, and paroxysmal theta in 1 boxer. Mean IQ (112 ± 15) was slightly above the normal national average (100 ± 15)
However, 12 boxers took a longer time in the trail making test, compared with average performance times
Thomassen et al (1979)
52
Qualitative comparative analysis
Display possible neurological consequences of amateur boxing
Total number of boxers: 53 amateur boxers
Number of bouts: 76 ± 44 bouts [range: 19-209 bouts]
Losses: 30 ± 16 losses [5-82 losses]
Career length: 8 ± 3 years [range: 3-16 years]
Control group: 53 former football players
Neurological, neuropsychological, and EEG examinations were completed on all participants
EEG results and neurological examinations did not display any significant differences between the 2 groups. Neuropsychological findings displayed a significant difference between the 2 groups (P < 0.05), as boxers possessed more dysfunctions in the motor function of the left hand, memory, and expressive speech
Bernick et al (2015)
36
Investigate the relationship between exposure variables, cognition, and MRI brain structural measures in a cohort of professional combatants
Fighters: 224 (131 mixed martial artists and 93 boxers. Age: range from 18 to 44, median of 27.7 years old)
Control: 22 (age and gender was not described within this study.)
MRI scans, along with cognitive function was assessed by a FES and a computer-based battery test that consists of 4 subtests of the CNS vital signs, including verbal memory, symbol digit coding, Stroop test, and a finger tapping test
Fighters who had more professional fights or an increased FES tended to have lower brain volumes, specifically the caudate and thalamus. In addition, processing speed declined in relationship to decreased thalamic volumes, along with increased fighting exposure. Increased scores on a FES used to reflect exposure to repetitive head trauma were linked with greater probability of possessing a cognitive impairment
McLatchie et al (1987)
53
Examine evidence of abnormal neuronal dysfunction within active amateur boxers
Amateur boxers: 20 (age: 26 ± 8.1 years old [range: 18-49 years]). Amateur bouts: 61.8 ± 56.8 [range: 4-200 bouts]
Participants underwent an EEG and a CT scan. Neuropsychological function was assessed by means of clinical psychometric procedures and computer administered tests, such as the Wechsler memory scale
7 (35%) of participants displayed neurological abnormalities
The most notable of these consisted of extensor plantar responses, and deterioration of rapid alternating movement of the hands and forearm
Abnormal neurological examination significantly correlated with increasing number of fights (P < 0.05 Mann–Whitney U test)
EEG abnormalities within 8 (40%) of participants were detected, many displayed local slow wave activity unrelated to any relevant medical history, and 2 displayed fast transients or discharges. However, did not possess a history of seizures
4 of the 8 EEG abnormalities (50%) also possessed an abnormal clinical examination
Abnormalities within EEG significantly correlated with age (P < 0.05 Mann–Whitney U test), as the younger the participant, the increased likelihood of obtaining an abnormal EEG.
CT scans were normal
9 (45%) of the boxers had poor performances on 2 or more clinical measurements
AEG, air encephalogram; APOE, apolipoprotein E; HRNTB, Halstead–Reitan neuropsychological test battery; MDS, Movement Disorder Society; PEG, pneumoencephalogram; QNST, quick neurological screening test; RMT, Randt memory test; UPDRS, Movement Disorder Society—Unified Parkinson's Disease rating Scale.
The meta-analyses results outlined in Figure 3A indicate that from a total population of 159 current and former boxers, only 86 (54.9%) had either chronic neuropsychiatric (NP) or neurological (NL) disorders related to boxing. The forest plot in Figure 3B demonstrates that 61.79% (i.e 46 of 71 current and former boxers) suffered from varying degrees of dementia or amnesia. Figure 3C illustrates that 51.42% (ie 36 of 70 active and former boxers) possessed various forms and severities of cognitive disorders, such as PD or AGIs, and Figure 3D illustrates that 52.29% (i.e 57 of 109 active and former boxers) possessed abnormal CT or EEG scan results.
Figure 3.: A display of forest plots showing (A) boxers who possess either NP or NL. (B) Boxers who possess dementia or amnesia. C, Boxers who possess PD or AGI, and (D) Boxers with abnormal CT or EEG scan results.
Efficiency of Headguards
There was limited information on the effectiveness of headguards in boxing (Table 3). Only 5 appropriate study types were considered suitable to include, and from these 5 study types, 2 provided data on the AIBA 2013 rule change. Davis et al58 highlighted that there was little difference between using and not using a headguard during amateur bouts. The data compared punches thrown and punches that contacted the head, pre and post the 2013 AIBA rule change. The following outputs were reported: rounds (Pre 2013—headguard: 29; Post 2013—without headguard: 50), total punches thrown expressed as an average (Pre 2013—headguard: 65.2; Post 2013—without headguard: 62.7), punches landed expressed as a bout average (Pre 2013—headguard: 7.6; Post 2013—without headguard: 10), and punches landed to the head expressed as a bout average (Pre 2013—headguard: 6.3; Post 2013—without headguard: 8.9). There were no significant differences between the Pre 2013—headguard and the Post 2013—without headguard (P = 0.380). The RRs of punches landed to the head were 0.82 and 0.89 for the Pre 2013—headguard and Post 2013—without headguard, respectively. However, there was an average 25% increase in punches landed per bout and an average 30% increase in punches landed to the head.
TABLE 3. -
Overview of Selected Studies on the Impact of Headguards in Boxing
Author (yr)
Study Type
Purpose
Participants' Background
Methods of Measurement
Findings
McIntosh, and Patton (2015)
54
Qualitative
Evaluate the impact energy attenuation performance on a variety of headguards designed for combat sports
Boxing headguards: Adidas (AIBA), and Top Ten Boxing (AIBA)
Lateral drop tests at 0.4, and 0.6 meters onto a flat rigid anvil, and a comparative reduction in peak headform acceleration with headguard only and glove only tests at 0.6, and 0.8 meters on a flat rigid anvil
Top Ten Boxing headguard possessed superior performance in comparison to the Adidas (AIBA). Mean peak acceleration was on average at all heights was between 32% and 40% lower at all meters for the Top Ten model compared with the Adidas boxing model
McIntosh, and Patton (2015)
55
Qualitative
Examine the effects of headguards on head impact dynamics and injury risk
Boxing Headguards: Adidas (AIBA), and Top Ten Boxing (AIBA)
Linear impact was devised, and a variety of impacts was delivered to an instrumented Hybrid III head and neck system both with and without an AIBA approved headguards
Impacts at selected speeds between 4.1 and 8.3 m/s were undertaken. The impactor mass was approximately 4 kg and an interface comprising a semirigid “fist” with a glove was used


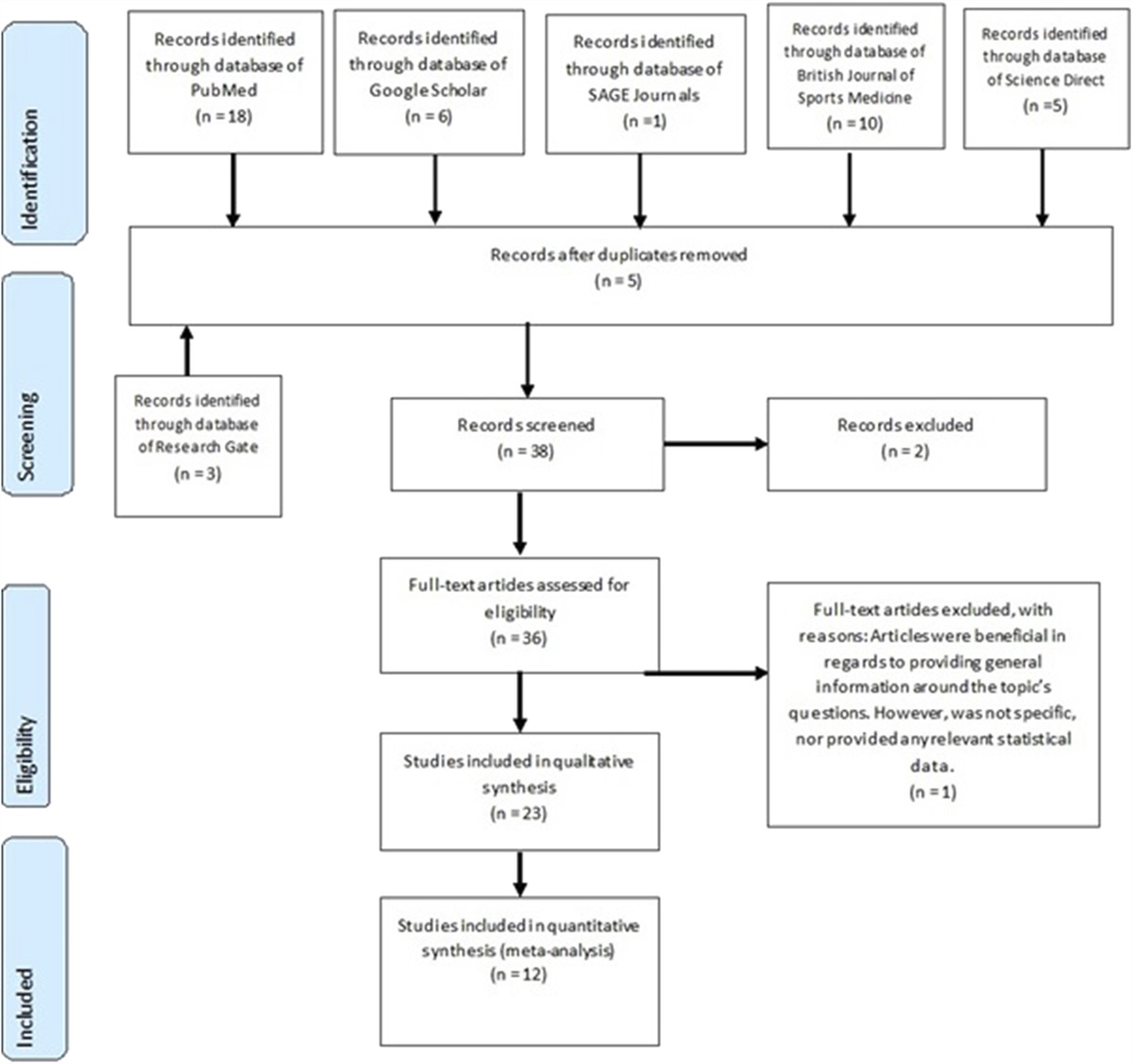

 Figure 1.:
Figure 1.:  Figure 2.:
Figure 2.:  Figure 3.:
Figure 3.:
留言 (0)