
記住我

The benefits of exercise for cardiovascular health are well recognized. However, exercise may have a U-shaped dose–response curve.1 Some of the strongest evidence for adverse cardiovascular consequences is in the development of atrial fibrillation (AF), where both professional and nonprofessional athlete populations seem to be at an increased risk when compared with the general population.2–5 Thromboembolic events, such as stroke, are well-known complications of untreated AF.6 Physical activity is believed to lessen an individual's risk of stroke, attributable to a reduction in cardiovascular risk factors associated with exercise participation in addition to the direct effects of exercise.4,7
On an individual level, studies have shown that endurance athletes who develop AF have a higher incidence of stroke when compared with both athletes and nonathletes without AF.8 CHA2DS2-VASc is a clinical tool used to assess the annual risk of thromboembolic events in AF and to inform anticoagulation therapy (see Supplementary Table 1, https://links.lww.com/JSM/A358).9 However, CHA2DS2-VASc is not validated in athletes, and many athletes will have a score of 0 or 1, indicating no need for anticoagulation. Athletes also demonstrate cardiac phenotypes, such as atrial dilatation, that are associated with an increased risk of stroke in the general population alongside adaptations to blood flow such as sinus bradycardia that are not captured in scoring tools, such as CHA2DS2-VASc.10,11 It is unknown whether cardiac phenotypes observed in athletes may contribute to an increased risk of stroke that is not appropriately risk stratified by CHA2DS2-VASc in athletes who develop AF.12
The aim of this study was to estimate the risk of stroke in veteran endurance athletes (≥40 years old) who develop AF compared with those who remain in sinus rhythm.
METHODS Study Design and ParticipantsAtrial Fibrillation in veteran athLETEs and the risk of Stroke (AFLETES) was approved by the ethics committee at the University of Leicester. Participants were recruited through advertising on social media, and relevant sporting clubs were asked to circulate the questionnaire to their members. The survey link remained open between March 17, 2021, and September 27, 2021.
Participants were linked to a web page that contained information about the study, where individuals were required to confirm informed consent. Participants completed a self-administered questionnaire (Jisc Online Surveys) that contained 27 questions (Supplementary document, https://links.lww.com/JSM/A358). The readability of the questionnaire was calculated using the Simple Measure of Gobbledygook index through an online readability checker to ensure that the reading age was between class years 5 and 7.13,14 Basic demographic data and medical history were collected, and information on health-related behaviors, estimated lifetime exercise dose (weekly dose multiplied by 52 and years of training), exercise participation characteristics and health data on AF, and stroke was also collected. CHA2DS2-VASc was calculated for each participant.
Statistical AnalysisFor continuous variables, normality was assessed using the Kolmogorov–Smirnov test and visual inspection of histograms.15 Continuous data are presented as mean (SD) or median (interquartile range) as appropriate. Categorical data are presented as n (%). Differences between those with and without AF were assessed through the χ2 test or the Fisher exact test for the categorical data and with the independent samples t test or Mann–Whitney U test as appropriate. The cohort was divided into 2 groups: those with and without AF. Mean difference (MD) and 95% confidence intervals (95% CIs) were calculated between these groups and Levene test for equality was used to assume equal variance. Individuals with AF were further substratified by CHA2DS2-VASc status. Individuals with AF and CHA2DS2-VASc of 0 or 1 (AFC0/1) made one group and ≥2 (AFC2) another, to reflect the clinical risk that governs when anticoagulation is often recommended.16 The association of AF with stroke was assessed using binary logistic regression models, adjusted for age, sex, and variables associated with the outcome in univariable models (P < 0.1) while excluding colinear variables. The Bayesian information criterion (BIC) and Nagelkerke pseudo R2 were used to decide upon the most parsimonious model and avoid overfitting due to the low number of stroke events. Data are presented as odds ratios (OR) alongside the 95% CI. All tests were 2 sided, and the significance level was set to 0.05.
The study is reported as per recommendations outlined by the Strengthening the Reporting of Observational Studies in Epidemiology Statement for cross-sectional studies.17
Patient and Public InvolvementPatient and public members had significant involvement in dissemination because the study was widely shared on social media platforms. The Global Cycling Network a YouTube channel with 2.6 million subscribers featured this study in a video: (https://www.youtube.com/watch?v=Fo0j94ODPiA).
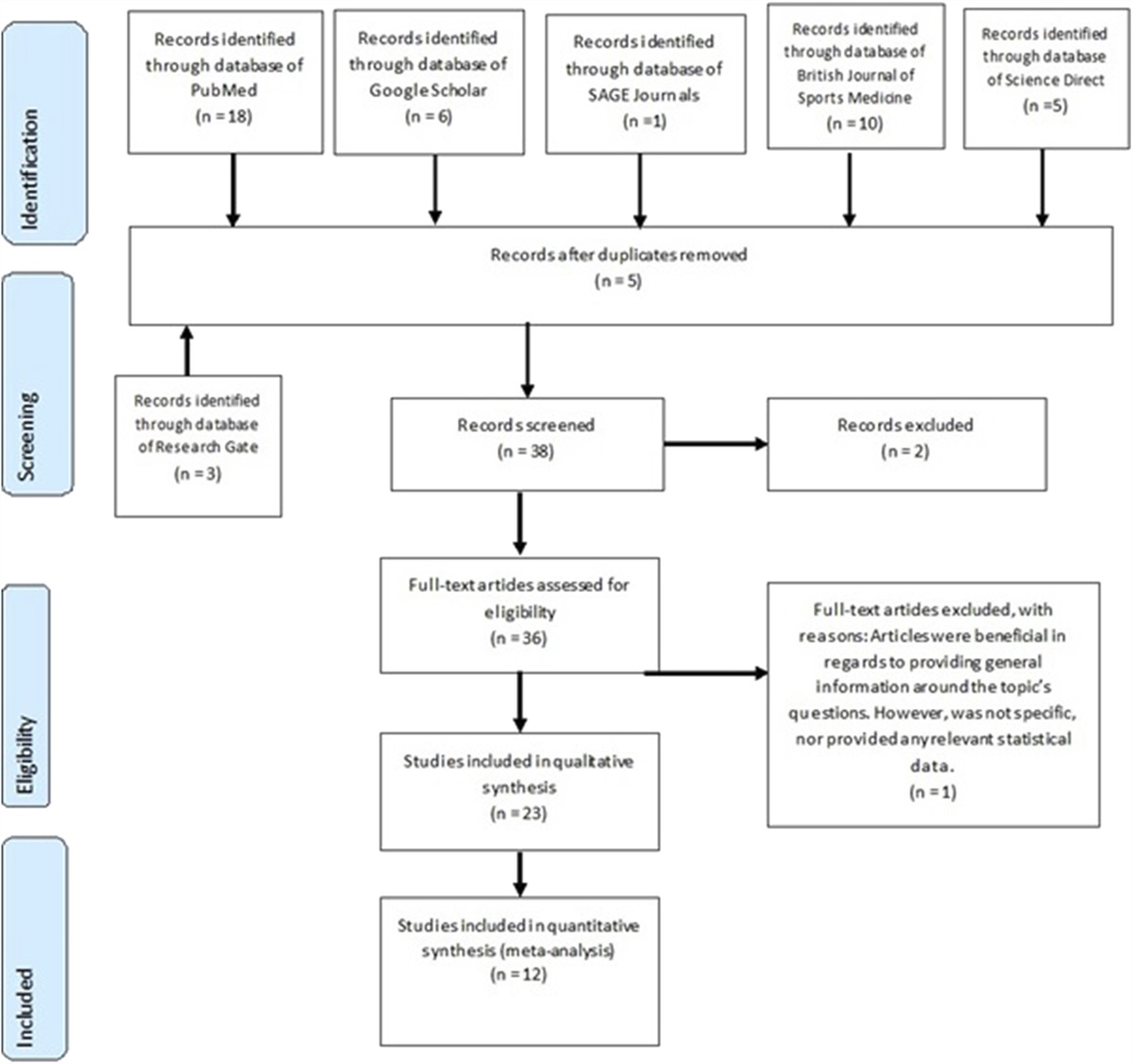
RESULTS Demographics, Exercise, and Cardiovascular Risk FactorsOverall, 1002 individuals from 41 countries across Africa, Asia, Australasia, Europe, and North and South America completed the survey (Supplementary document, https://links.lww.com/JSM/A358). Figure 1 shows how the final analysis data set was derived and reasons for exclusion.
 Figure 1.:
Figure 1.: Flow diagram depicting reasons for exclusion and final analysis cohort.
Demographic data for the overall population and stratified by AF status are shown in Table 1. The final analysis data set contained 942 individuals (94% completion rate), with the majority being male (84%) and white ethnic background (96%) from English-speaking countries. Cycling was the most frequently reported sport (n = 677, 72%) followed by running (n = 558, 59%) and triathlon (n = 245, 26%). More than half of the participants reported local events (54%) to be their highest level of competition, and 237 individuals (25.2%) competed at national level or above. On average, individuals exercised 9.3 hours per week (SD: 5.2), over 20.0 years (SD: 13.4). Although rates of diabetes mellitus (DM), congestive heart failure, thromboembolism, vascular disease, and preexisting cardiovascular disease and cardiomyopathy were low, approximately 1 in 10 participants reported hypertension (HTN) and high cholesterol.
TABLE 1. - Characteristics of Participants Overall and Stratified by AF Status Variable Overall (n = 942) Individuals Without AF (n = 752) Individuals With AF (n = 190) P Male sex 788 (84) 613 (82) 75 (92) <0.01 Age, yrs 52.4 (9) 51.3 (8) 56.6 (9) <0.01 Ethnicity White 910 (97) 727 (97) 183 (96) 0.81 Non-white 32 (3) 25 (3) 7 (4) Profession White/blue collar versus others = 0.12 White/blue collar 842 (89) 677 (90) 163 (86) Manual labourers 65 (7) 50 (7) 15 (8) Full-time athlete 4 (0.4) 3 (0.4) 1 (1) Unemployed 31 (3) 21 (3) 10 (5) Smoking Smoking history versus never smoked = 0.91 Current smoker 7 (1) 6 (1) 0 Previous smoker 239 (25) 190 (25) 49 (26) Never smoked 696 (74) 555 (74) 141 (74) Alcohol (units/wk) Non drinker versus drinker = 0.24 0 138 (15) 104 (14) 32 (17) <8 units 426 (45) 341 (45) 85 (45) 8-15 units 250 (27) 203 (27) 47 (25) >15 units 124 (13) 100 (13) 24 (13) Binge drinking Never versus binge drinking <0.01 Never 436 (46) 326 (43) 108 (57) Up to once per month 329 (35) 270 (36) 59 (31) More than once per month 177 (19) 154 (21) 23 (12) Highest level of competition International + professional versus others = <0.01 Local 514 (55) 419 (56) 95 (50) Regional 199 (21) 168 (22) 31 (16) National 120 (13) 90 (12) 30 (16) International 109 (12) 75 (10) 34 (18) Professional 8 (1) 4 (1) 4 (2) Exercise dose (h/wk) 9.3 (5.2) 9.0 (5) 10.5 (7) P < 0.01 Training, yr 20.0 (13.4) 18.8 (13) 24.8 (15) P < 0.01 Lifetime exercise dose (×1000 h) 10.1 (10.9) 9.2 (9) 14.0 (15) P < 0.01 Competitions per year 5 (3-12) 5 (3-12) 6.5 (2-20) 0.05 Resting heart rate (beats per minute) 52.0 (9.4) 52.2 (9.6) 51.5 (8.9) 0.40 DM 12 (1) 9 (1) 3 (1.6) 0.68 Hypertension 101 (11) 73 (10) 28 (14.7) 0.045 Thromboembolism 18 (2) 11 (1) 7 (4) 0.05 Congestive heart failure 5 (1) 1 (0.1) 4 (2) <0.01 Vascular disease 13 (1) 8 (1) 5 (3) 0.10 High cholesterol 104 (11) 81 (11) 23 (12) 0.60 Stroke 26 (3) 12 (2) 14 (7) <0.01 Age of first stroke (yr) 48.1 (12.5) 43 (13) 52.4 (10) 0.06There were 190 individuals (20%) who reported a history of AF, and they were older than those without AF by 5.28 years (95% CI, 3.97-6.59 P < 0.01). Those with AF showed lower rates of binge drinking behaviors, were more likely to be swimmers (P = 0.01), and included a higher number of international and professional athletes (P < 0.01) (Table 1) (Figure 2). The number of hours exercised per week (MD: 1.47, 95% CI, 0.64-2.30 P < 0.01) and years trained (MD: 6.03, 95% CI, 3.64-8.41 P < 0.01) were higher in those who had AF. The highest quartile of lifetime exercise dose had the largest proportion of individuals with AF (Figure 2). There were higher rates of both HTN (P < 0.05) and congestive heart failure (P < 0.01) in individuals with AF. Of those participants reporting AF, more than half were paroxysmal (n = 119, 63%) (Table 2). Most individuals were diagnosed after reporting symptoms (n = 134, 71%).
 Figure 2.:
Figure 2.: Bar chart showing the number and proportion of individuals with AF stratified into quartiles of lifetime exercise dose (A) and exercise type (B). Panel A: P value refers to chi-squared test across the groups. Missing exercise lifetime dose for 12 individuals (4 with AF). Lifetime exercise dose (per 1000 hours) by Quartile: 1 = 0 to 3.12, 2 = 3.12 to 7.28, 3 = 7.28 to 13.0, 4 >13.0. Panel B: P value = for each of the 4 most common sports, the prevalence of AF for that sport was compared with the prevalence in all the other athletes not participating in that sport.
TABLE 2. - Characteristics of Participants With a Diagnosis of AF, With and Without Stroke Variable AF With No Stroke (n = 176) AF With Stroke (n = 14) P Male sex 162 (92) 13 (93) 0.49 Age 56.5 (9) 57.6 (9) 0.64 Age of AF diagnosis 48.6 (13) 48.4 (14) 0.96 AF Paroxysmal 113 (64) 6 (43) 0.46 Persistent 28 (16) 4 (29) 0.83 Permanent 31 (18) 3 (21) 0.91 Unknown 4 (2) 1 (7) Diagnosis of AF Symptoms 127 (72) 9 (64) 0.60 Incidentally from heart rate monitor 39 (22) 0 0.08 Athlete screening 24 (14) 1 (7) 0.70 Diagnosed after stroke/transient ischaemic attack NA 11 (79) NA White ethnicity 170 (97) 13 (93) 0.48 White/blue collar 153 (87) 11 (79) 0.38 Never smoked 129 (73) 12 (86) 0.31 0 units alcohol per week 29 (17) 4 (29) 0.25 Never binge drink 99 (56) 9 (64) 0.56 Cycling 140 (80) 6 (43) <0.01 Running 103 (59) 8 (57) 0.92 Triathlon 39 (22) 6 (43) 0.08 Swimming 37 (21) 6 (43) 0.06 Other 26 (15) 4 (29) 0.24 Highest level of competition National, international, and professional versus others = 0.45 Local 89 (51) 6 (43) Regional 29 (17) 2 (14) National 28 (16) 2 (14) International 30 (17) 4 (29) Professional 3 (2) 1 (7) Exercise dose per week (h) 10.4 (7) 10.8 (3.5) 0.48 Training years (yrs) 24.4 (15) 30.4 (17.6) 0.16 Lifetime exercise dose (×1000 h) 13.8 (15) 14.9 (10.9) 0.81 Competitions per year 6 (2-20) 7.5 (3.5-25) 0.92 Resting heart rate (beats per minute) 51.4 (8.4) 54.1 (14.4) 0.25 DM 1 (1) 2 (14) 0.01 Hypertension 26 (15) 2 (14) 0.66 Thromboembolism 7 (4) 0 NA Congestive heart failure 4 (2) 0 NA Vascular disease 5 (3) 0 NA High cholesterol 20 (12) 3 (21) 0.19 Pacemaker 7 (4) 0 NA Myocardial infarction 3 (2) 0 NA Cardiomyopathy 2 (1) 0 NAThere were 26 individuals (3%) who reported stroke. The average age at which the stroke occurred was 48.1 ± 12.5 years. Most strokes occurred in individuals with CHA2DS2-VASc of 0 (n = 14, 54%) or 1 (n = 8, 31%). The proportion of individuals reporting stroke can be seen in Figure 3, where there was a higher proportion of strokes in those with AF, AFC0/1, and AFC2 compared with those without AF. In individuals with AF, there were 14 strokes (54%), but in 11 (42%) of these individuals, AF was diagnosed following the stroke (Supplementary Table 2, https://links.lww.com/JSM/A358). In those with AF and stroke, most occurred in individuals with AFC0/1 (n = 12, 46%) with only 2 strokes (8%) reported in those with AFC2. Those with AF and stroke had a greater proportion of individuals with DM when compared with those who did not have a stroke (Table 2). Only half those with AFC2 reported taking anticoagulation therapy (Supplementary Table 3, https://links.lww.com/JSM/A358). Three individuals had a subsequent stroke after their initial diagnosis of stroke, 2 of whom were anticoagulated.
 Figure 3.:
Figure 3.: Bar chart showing the number and proportion of individuals with stroke stratified by AF and CHA2DS2-VASc status. Percentage refers to the proportion of individuals with stroke in each category.
Associations with Atrial FibrillationUnivariable associations with AF are shown in Supplementary Table 4 (https://links.lww.com/JSM/A358). All measures of exercise dose were associated with AF as was male sex (OR, 2.49, 95% CI, 1.39-4.45, P < 0.01), but binge drinking more than once per week (OR, 0.54, 95% CI, 0.33-0.86, P = 0.01) was associated with a reduced risk of AF. In multivariable models, age (OR, 1.06, 95% CI, 1.04-1.09, P < 0.01), lifetime exercise dose (OR, 1.02, 95% CI, 1.00-1.03, P = 0.02), swimming (OR, 1.56, 95% CI, 1.02-2.39, P = 0.04), and male sex (OR, 2.48, 95% CI, 1.38-4.43, P < 0.01) remained independently associated with AF (Figure 4).
 Figure 4:
Figure 4: .Odds ratios for selected variables associated with AF (top) and stroke (bottom).
Associations with StrokeUnivariable analysis are seen in Supplementary Table 5 (https://links.lww.com/JSM/A358). Atrial fibrillation was associated with stroke (OR, 4.71, 95% CI, 2.14-10.37, P < 0.01), and this was true for all AF types and individuals with AFC0/1 (OR, 4.15, 95% CI, 1.88-9.16, P < 0.01). In the multivariable models, AF (OR, 4.18, 95% CI, 1.80-9.72, P < 0.01), DM (OR, 6.72, 95% CI, 1.30-34.75, P = 0.02), and AFC0/1 (OR, 4.20, 95% CI, 1.83-9.66, P < 0.01) remained associated with stroke, but age (OR, 1.03, 95% CI, 0.99-1.08, P = 0.20) and male sex (OR, 0.74, 95% CI, 0.24-2.27, P = 0.60) did not (Figure 4). The construction of the multivariable model can be seen in Supplementary Table 6 (https://links.lww.com/JSM/A358). A multivariable analysis of AFC2 was not conducted due to the low number of events.
DISCUSSIONAFLETES aimed to estimate the risk of stroke in competitive endurance athletes who have developed AF. To our best knowledge, this is the first study to assess this risk and the most widely distributed and largest survey to assess AF in athletes. Individuals mostly participated in endurance sport, and the majority were White and male. The overall burden of cardiovascular disease and risk factors for atherosclerotic disease was low, and the majority of participants had a CHA2DS2-VASc of 0 or 1 (n = 884, 93.8%).
Risk Factors for Stroke in Veteran Athletes and Clinical ImplicationsThe most significant and novel result from this survey is that AF was independently associated with stroke in athletes, even in those with low CHA2DS2-VASc score. This suggests that current methods of risk stratification in AF may not appropriately capture this risk in athletes, although it is believed to perform better in individuals at lower risk of stroke compared with the previous congestive heart failure, hypertension, age ≥75, diabetes mellitus and stroke (CHADS) score.16 Currently, individuals with low CHA2DS2-VASc score are unlikely to be offered anticoagulation because the risk of stroke is deemed to be low (approximately 0.8 events per 100 patient-years), and the risk of major bleeding may outweigh any benefits of anticoagulation for stroke prevention.18 Although this study has not compared the risk of stroke in athletes with AF against individuals with a low CHA2DS2-VASc score in the general population, the results may suggest that the risk of stroke in athletes with AF is not negligible, even in those with no risk factors. Although physical activity undisputedly improves cardiovascular health, further longitudinal studies in athletes with AF are required to accurately determine stroke risk and the need for anticoagulation to guide clinical shared decision making.
Typically, anticoagulation is offered to individuals with CHA2DS2-VASc scores of ≥2. In this study, the number of individuals receiving anticoagulation for AF was 30.5%, and it was only 53.8% in AFC2, which suggests that there is a lower rate of treatment in this group than would be expected.18 Clinician or athlete reluctance for anticoagulation may have several drivers. First, fears of bleeding associated with exercise participation in sports with a risk of traumatic injury such as cycling.19 Second, anticoagulation may mandate the individual to refrain from sports participation.2,12 Finally, as participation in competitive exercise is viewed as a positive health-related behavior, it may sway clinicians and patients away from anticoagulation due to perceptions of low risk. Although exercise may be cardioprotective, the results from this study suggest that exercise does not completely exclude an individual from the risk of stroke, and hesitancy against anticoagulation therapy should be carefully explored and balanced while prospective data are unavailable. Of those with AF and a stroke, most (11 of 14) were diagnosed with AF after the stroke. This represents a significant proportion of those with AF who had a stroke (79%) and brings into question how many athletes may have subclinical paroxysmal AF, particularly because this may not be diagnosed even with short-term ambulatory monitoring.20
Potential Mechanisms of StrokeWithin the limitations of the survey design, inferring causality is not justified. However, there may be biological plausibility for the observed risk of stroke. Left atria are more dilated in athletes.21 In the general population, meta-analyses have shown that left atrial enlargement is associated with a graded risk of stroke.10,22 Fibrosis, oxidative stress, and inflammation may lead to myopathic states of the atria.23 Atrial myopathy is associated with endothelial dysfunction and hemodynamic stasis, which in turn may favor a prothrombotic state.23 During exercise, there is increased reliance on the atrial contractile–booster function, but this can be reduced in individuals with AF, which could promote deranged atrial flow.24 Individuals who engage in exercise frequently develop sinus bradycardia. Although traditionally considered a benign phenotype of cardiorespiratory fitness, bradycardic patterns may be a sign of atrial dysfunction that can cause hemodynamic stasis, a component of Virchow triad.25 Although numerous studies have investigated structural and functional adaptations within the athletic heart syndrome, there are no data using novel flow phenotyping methods.26
Swimming is Associated with Atrial FibrillationThis is the first study to demonstrate that swimming was associated with an increased risk of AF when compared with other sports and after adjusting for lifetime exercise dose.27 Other studies have estimated the prevalence of AF in endurance swimmers and compared that with hospital patients.27,28 Swimming varies from sports such as cycling and running in 2 ways. First, individuals perform in a horizontal or prone position and so the characteristics of hemodynamic homeostasis may vary when compared with sport conducted in orthostasis. Orthostatic intolerance in swimmers has been previously described, and this may be accompanied by changes in aut
留言 (0)