Providing physiotherapy or other health care services in alternative ways to face to face in-person delivery has been around for many years. One of the earliest examples is a trial published in 1977 comparing telephone consultations to in-person education to parents of children with disabilities.1 As technology has developed, research into alternative models of remote health care delivery has exploded. A large range of options now exist, covering the spectrum from assessment to intervention and including real-time video consultations, remote monitoring, health care mobile applications, and Web-based platforms. As the different ways in which remote health care can be offered have increased, so too has the variation in terminology. This can be problematic; for example, a search of the Cochrane Database of Systematic Reviews using the key words “telehealth or telerehabilitation or telemedicine or e-health or m-health” resulted in only 41 hits. Adding the term “digital health” and “virtual care” increased the yield to 137 reviews, but this included unrelated topics, for example, related to digital nerve blocks, or virtual reality training (that can occur either in-person or remotely).
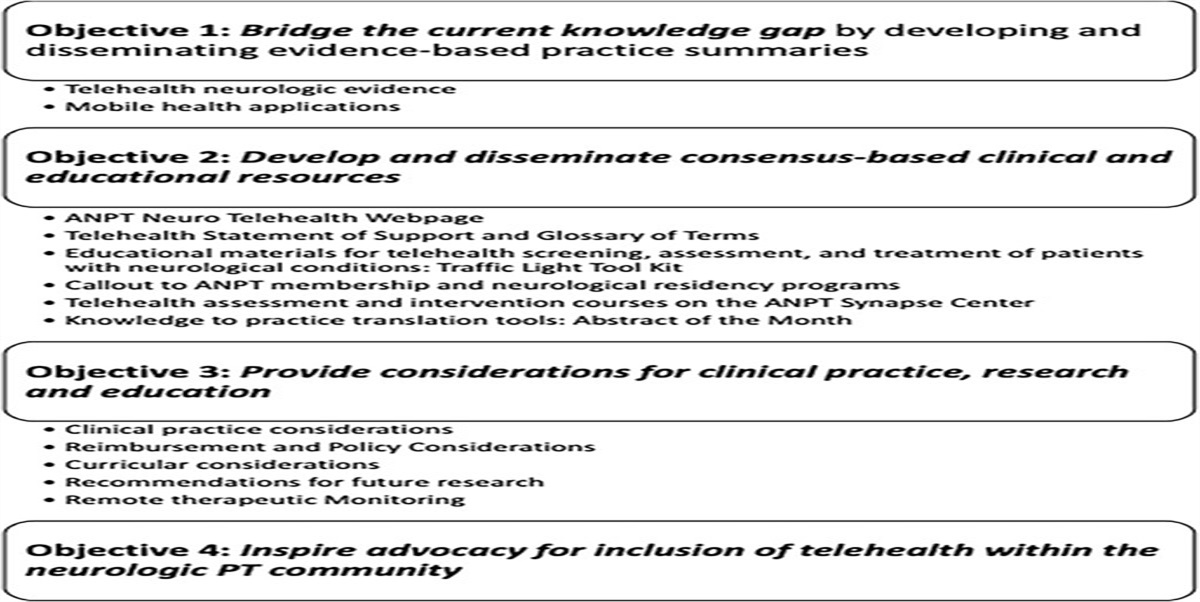
In this Digital Health Special Issue of JNPT, we include 5 papers that span the range from assessment to intervention, including activity monitoring for people with Parkinson disease, telerehabilitation models of pelvic floor retraining for people with multiple sclerosis, tele-exercise programs for people with spinal cord injury, development and testing of a modified version of the Fugl-Meyer assessment for use in telerehabilitation, and consensus-based best practice strategies for implementing telehealth in neurological clinical practice. The papers included in this issue all use different terminology, including telerehabilitation, telehealth, tele-exercise, and digital health interventions. Other common terms include “remote or virtual health care.” In the United States, the Health Resource Services Administration defines telehealth as “the use of electronic information and telecommunication technologies to support long-distance clinical health care, patient and professional health-related education, public health, and health administration.”2 The American Telemedicine Association Rehabilitation Group3 describes the difference between the term “telehealth” (“broad term used to describe the use of electronic or digital information and communications technologies to support clinical healthcare,...”) and “telerehabilitation” (“the delivery of rehabilitation and habilitation services via information and communication technologies...”)
Variations in terminology can lead to lack of clarity about the specifics of interventions delivered in trials, as well as difficulties in identifying and synthesizing relevant evidence. A recent review of the evidence for telehealth for stroke rehabilitation services recommends a taxonomy of terminology.4 The taxonomy recommends that the term “telehealth” be used as an overarching term to describe health care provided remotely, and that interventions are described according to their purpose (assessment, intervention), timing of delivery (synchronous, asynchronous, continuous), and type of technology used (telephone, videoconferencing, Web sites, or digital apps). For example, in the case of the paper in this issue by Kahraman et al, the intervention would be described as “Pelvic floor muscle training using synchronous videoconferencing.” We urge authors to implement this taxonomy to create greater clarity in the field.
We argue that the time for trials comparing telehealth versus in-person delivery has past, and instead research efforts should focus on the development and implementation of interventions with known effectiveness via telehealth. Development of telehealth modes of delivering interventions should involve careful codesign in partnership with lived experience experts. This is important to ensure what is created is fit for purpose, accessible, and acceptable to the end user. An example of this is the development of the i-REBOUND after Stroke Web site.5 This Web site was developed in close partnership with people with stroke, and the design features (eg, large icons, ease of navigation, page layouts, and strengths-based approach) reflect this. Qualitative studies, such as that conducted by Fowler King et al in this edition, provide valuable information about barriers and facilitators to effective implementation. Being able to accurately assess the effect of interventions using valid and reliable assessments that can be delivered remotely is essential to drive the field forward. The study by Carmona et al in this issue provides valuable information about the adaptation of the Fugl-Meyer assessment tool for telehealth.
Telehealth modes of delivery can increase the accessibility of services. Many people with mobility difficulties find difficulties with transport a barrier to attending in-person appointments. Across urban and rural environments, telehealth may also overcome financial burdens and distance from major medical centers that offer specialty care for persons with neurological disorders. In countries with sparse populations over wide geographical areas, such as in Australia or rural areas of the United States and Canada, telehealth models of care can mean more people have access to the services they need. Telehealth also holds promise for providing more health care services to people living in low- to middle-income countries. In India, a nation-wide study has been tracking Internet use since 1998. Their latest report estimates 67% of the urban population and 31% of the rural population are regular Internet users, with increases in rural areas driving growth, particularly in mobile phone usage.6 However, another report suggests India has the lowest smartphone ownership, well below the median of 45% across emerging economies and 76% in advanced economies.7
Accessibility issues for telehealth are not limited to low-income countries. Studies in the United States have reported uptake of telehealth services is lower amongst older age groups, Black Americans, unemployed individuals, those without high school education, and those living outside of metropolitan centres.8–10 Development and implementation of telehealth models of care must include strategies to ensure equity of access.
We hope you enjoy this issue.
1. Heifetz LJ. Behavioral training for parents of retarded children: alternative formats based on instructional manuals. Am J Ment Defic. 1977;82(2):194–203.
2. Health Resources & Services Administration (HRSA). What is telehealth? HRSA Web site.
https://www.hrsa.gov/rural-health/topics/telehealth/what-is-telehealth. Published March 2022. Accessed June 17, 2023.
3. Richmond T, Peterson C, Cason J, et al. American Telemedicine Association's principles for delivering telerehabilitation services. Int J Telerehabil. 2017;9(2):63–68. doi:10.5195/ijt.2017.6232.
4. English C, Ceravolo MG, Dorsch S, et al. Telehealth for rehabilitation and recovery after stroke: state of the evidence and future directions. Int J Stroke. 2022;17(5):487–493. doi:10.1177/17474930211062480.
5. Stroke Foundation. Welcome to iREBOUND. EnableMe Web site.
https://irebound.enableme.org.au. Published 2023. Accessed June 17, 2023.
6. Internet Mobile Association of India (IAMAI). Internet adoption in India (ICUBE 2020). IAMAI Web site.
https://www.iamai.in/research/internet-adoption-india. Published June 2021. Accessed June 17, 2023.
7. Silver L. Smartphone Ownership Is Growing Rapidly Around the World, But Not Always Equally. Washington, DC: Pew Research Center; 2019.
https://www.pewresearch.org/global/dataset/spring-2018-survey-data. Accessed June 17, 2023.
8. Werneke MW, Deutscher D, Grigsby D, Tucker CA, Mioduski JE, Hayes D. Telerehabilitation during the COVID-19 pandemic in outpatient rehabilitation settings: a descriptive study. Phys Ther. 2021;101(7):pzab110. doi:10.1093/ptj/pzab110.
9. Strowd RE, Strauss L, Graham R, et al. Rapid implementation of outpatient teleneurology in rural Appalachia: barriers and disparities. Neurol Clin Pract. 2021;11(3):232–241. doi:10.1212/CPJ.0000000000000906.
10. Peirce RP, Stevermer JJ. Disparities in the use of telehealth at the onset of the COVID-19 public health emergency. J Telemed Telecare. 2023;29(1):3–9. doi:10.1177/1357633X20963893.





留言 (0)