
記住我




Following recovery from unilateral vestibular hypofunction (UVH), interruption of regular daily activities may precipitate a decompensation of a previously compensated vestibular system. Decompensation is characterized by a reemergence of symptoms consistent with that experienced during the initial insult/injury (eg, dizziness, oscillopsia, balance difficulty) and has been previously documented in transient situations that have demonstrated rapid resolution.1,2 Decompensation has been attributed to a lack of central nervous system input of vestibular, visual, and somatosensory signaling integrated and used to control adapted motor outputs.1 Therefore, anything that interrupts regular daily activity for a prolonged period of time, such as illness or hospitalization, may contribute to decompensation.
SARS-CoV-2 (COVID-19) was first identified in December 2019 in Wuhan, China.3 COVID-19 most often causes respiratory symptoms similar to a cold or the flu; most people infected with the virus will experience mild to moderate illness. However, some will develop severe illness and require medical attention, with 2.1% of people hospitalized. Hospitalized individuals with significant pulmonary effects may require intensive care unit (ICU) stays and supplemental oxygen limiting their mobility. There has also been a number of cases reporting the development of vestibular neuritis during and following COVID-19 infection.4-7 Vestibular neuritis is the most common cause of UVH and most often affects the superior vestibular nerve, resulting in an anatomical pattern of impaired horizontal and anterior semicircular (A-SCC) canals and utricle, with a sparing of the posterior semicircular canal (P-SCC) and saccule.8-10
Vestibular schwannoma resection (VSR) is another cause of UVH. The pattern of impairment in VSR results in severe symptoms of dizziness, oscillopsia, and imbalance, and reduced function of the vestibulo-ocular reflex (VOR) in all canals ipsilateral to the lesion.11 Recovery and improvement in symptoms following unilateral VSR occur as a result of central nervous system compensation and habituation.12 Physiologic compensation following a profound loss, like that seen following VSR, results in structural neurogenesis leading to the proliferation of GABAergic neurons, astrocytes, and microglial cells in the vestibular nuclei, believed to occur in response to the apoptosis of neurons.13 These new neurons and intact neurons remaining in the vestibular nuclei experience multimodal compensation—encoding proprioceptive, motor efferent, and vestibular information from the contralesional and ipsilesional side, if any function is preserved.14 Thus, compensation is dependent upon the presence of proprioceptive, motor, and vestibular input. This reweighting of vestibular nuclei encoding leads to compensation in both the vestibulo-ocular and vestibulo-spinal systems.14,15 In addition, functional improvements in postural stability occur through increased reliance on other sensory modalities,16 while oculomotor movements are utilized to overcome deficits in the VOR.17 Such recovery can occur spontaneously but is dependent upon appropriate sensory and motor stimulation. However, greater improvements in compensation and habituation can be produced by implementing high doses of specific head motion, mobility, and balance exercise typically prescribed in vestibular rehabilitation.18
In this case, we report on an individual presenting to an outpatient physical therapy clinic with persistent vestibular symptoms and moderate disability 6 months after a prolonged intensive care stay, and resulting months long reduction in activity, for COVID-19 related illness. This patient also has the unique medical history of past VSR. In this case, we hypothesize the presentation of vestibular decompensation following illness and demonstrate the potential role of vestibular rehabilitation in contributing to recovery in this person.
CASE DESCRIPTIONA 49-year-old woman, M.W. (not her real initials), self-referred to outpatient vestibular rehabilitation due to complaints of persistent dizziness and decreased balance. Pertinent medical history included left VSR in 2011. Other reported past medical history included the following: acne, colon polyp, depression, hypothyroidism, intrauterine device, migraine, postoperative nausea, seasonal allergies, and staph infection. Because of history of migraine and its association with vestibular symptoms,19 migraine status was assessed and determined to be stable and not active. The patient had been taking baclofen for migraines since September 2018, now has migraines 2 to 3 times a year, takes meloxicam for these breakthrough headaches, and symptoms include right-sided head and facial pain, photophobia, and nausea. None of these symptoms were reported by the patient. Medications included levothyroxine (Synthroid) 137-μg tablet, baclofen (Lioresal) 20-mg tablet, bupropion XL (Wellbutrin XL) 300-mg, fluconazole (Diflucan) 150-mg tablet, meloxicam (Mobic) 7.5-mg tablet, and tretinoin (Retin-A) 0.1% cream.
Patient-reported symptoms immediately following resection included dizziness/vertigo, left-sided hearing loss (resulting in need for the use of a hearing aid), oscillopsia, and imbalance that was successfully treated with vestibular rehabilitation following surgery. M.W. reports having experienced no dizziness or imbalance in the intervening 10 years.
In March 2021, M.W. was diagnosed with COVID-19 and subsequently hospitalized in the ICU for 5 days. After discharge, she required supplemental oxygen use via nasal cannula at home for 13 weeks but was no longer using at the time of initial evaluation. M.W. presented to the clinic in August 2021 with complaints of persistent dizziness and imbalance, which she reported had been ongoing for approximately 4 months. M.W. reported that her new symptoms of dizziness and imbalance began several weeks following discharge from the hospital, while recovering at home from COVID-19 and had not subsided. At this time M.W. had no complaints of ongoing COVID-19 symptoms (ie, fatigue, difficulty breathing) or visually induced dizziness. M.W. denied hearing loss or lightheadedness with position changes but stated that she “feels like she was back to where she was before vestibular rehab ten years ago following her surgery.” Per patient report, her neurologist ruled out medical causes of her vertigo and recommended vestibular therapy.
At the initial examination, the patient was ambulating independently with no use of an assistive device. Positional testing for benign paroxysmal positional vertigo was performed and found to be negative throughout. Visual observation of facial muscle function, along with conjugacy of gaze and extraocular movements, revealed no apparent deficits; therefore, cranial nerve testing was not performed. M.W. completed the following questionnaires: Dizziness Handicap Inventory (DHI, range from 0 to 100, with higher scores indicating higher disability),20 Activities-specific Based Confidence Scale (ABC, range from 0% to 100%, with higher scores indicating higher confidence),21 UAB Life Space Assessment (LSA, range from 0 to 120, with higher score indicating a larger life space),22 and visual analog scale (recorded with a 10-cm visual analog scale for dizziness and unsteadiness; score is determined by measuring from the left limit to the patient’s mark; and higher score indicates greater intensity of symptoms).23 Performance-based measures gathered at the initial examination included the MiniBEST (range from 0 to 28, with higher scores indicating better balance performance),24 2-Minute Walk Test (2MW, with greater distance indicating greater gait capacity),25 video head impulse test26 (vHIT; ICS Otometrics, Natus Medical Incorporated, Denmark), and computerized dynamic visual acuity (cDVA).27 Assessment and treatment protocol was approved by The University of Utah Institutional Review Board. M.W. provided written consent prior to assessment and data collection.
Initial AssessmentResults of all patient-reported and performance-based measures collected at the initial examination are shown in the Table.
Table. - Outcome Measures Taken Before and After 6 Weeks of Vestibular Physical Therapya Pretreatment Posttreatment Percent Change (Pre to Post) VAS: dizziness 29/100 0/100 100% decrease VAS: unsteadiness 30/100 4/100 86.7% decrease DHI 46 14 69.6% decrease ABC (%) 90.3 97.19 7.6% increase LSA (0-120) 120 100 16.7% decrease MiniBEST (maximum 28) 19 25 31.6% increase Anticipatory Subscore 6/6 6/6 No change Reactive Postural Subscore 3/6 6/6 100% increase Sensory Orientation Subscore 2/6 4/6 102.1% increase Dynamic Gait Subscore 8/10 9/10 12.5% increase 2MW, m 158 275 74.1% increase Post-2MW VAS: dizziness 50/100 0/100 100% decrease Post-2MW VAS: unsteadiness 45/100 0/100 100% decrease DVA: left dynamic difference −0.40 −0.38 5% decrease DVA: right dynamic difference −0.42 −0.24 43% decrease vHIT gain-LH (mean/SD) 0.63/.05 0.73/0.08 15.9% increase vHIT gain-RH (mean/SD) 0.93/.03 0.99/0.03 6.5% increase vHIT gain-LA (mean/SD) 0.51/0.05 0.58/0.13 13.7% increase vHIT gain-RA (mean/SD) 0.91/0.09 1.09/0.04 20.9% increase vHIT gain-LP (mean/SD) 0.57/0.06 0.72/0.06 26.3% increase vHIT gain-RP (mean/SD) 0.72/0.06 0.86/0.06 19.4% increase Compensatory saccade frequency (Sacc/head impulse) LH 1.86 1.6 13.9% decrease RH 1.05 0.83 21% decrease LA 1.08 1.05 2.8% decrease RA 0.5 0.57 14% increase LP 0.67 0.71 5.9% increase RP 0.23 0.42 82.6% increase Compensatory saccade latency (ms, mean/SD) LH 163/67.7 151.7/73.9 6.7% decrease RH 201.6/63.9 178.1/27.7 11.4% decrease LA 174.6/30.6 145.9/38.5 16.6% decrease RA 65.6/53.1 184.0/163.9 180.5% increase LP 95.3/64.5 156.8/86.3 64.5% increase RP 140.0/0.0 168.5/87.2 20.4% increaseAbbreviations: ABC, Activity-specific Balance Confidence Scale; DHI, Dizziness Handicap Inventory; DVA, dynamic visual acuity; LA, left anterior canal; LH, left horizontal canal; LP, left posterior canal; LSA, Life Space Assessment; MCID, Minimal Clinically Important Difference; RA, right anterior canal; RH, right horizontal canal; RP, right posterior canal; 2MW, 2-Minute Walk Test; VAS, visual analog scale; vHIT, video head impulse test.
a2MW normative values for women 18 to 54 years of age = 180.8-185.3 m. DHI MCID = 18; ABC MCID = 18.1%; 2MW MCID = 42.5 m; and MiniBEST MCID = 4 points.
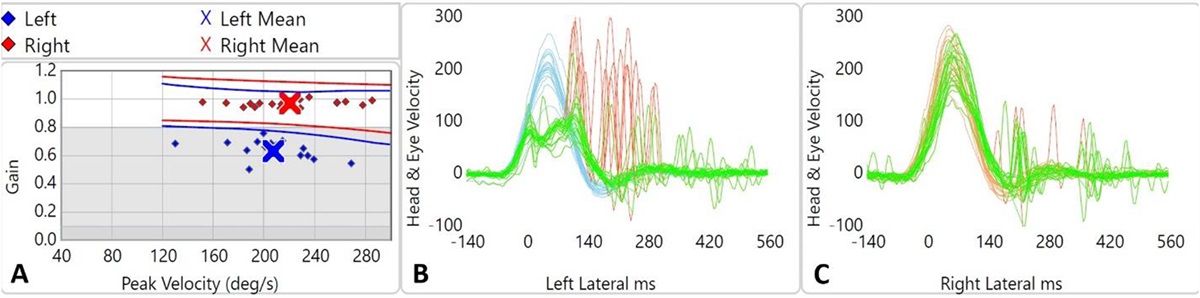
The cDVA and 6-canal vHIT were used to assess the integrity of VOR. Left and right cDVA logMAR scores (0.34, 0.36) were similar and correspond to a 4-line loss compared with static score (−0.06). The VOR was assessed using vHIT, a valid and reliable measure of vestibular function that allows for assessment of each of the 6 semicircular canals independently.28 Metrics assessed were the VOR gain, which is calculated as the eye velocity/head velocity (1.0 = perfect) and corrective saccade metrics of frequency and latency. VOR gain values below what is considered normal (<0.7)29,30 were detected on the affected left (ipsilesional) but not on the right (contralesional). Specifically, on the ipsilesional side, the A-SCC canal was observed to be the weakest (0.51), the P-SCC had the second lowest gain (0.57), while the horizontal semicircular canal (H-SCC) was found to be the strongest (0.63). These reduced gains indicate that the eyes are not moving at a velocity high enough to maintain steady visual fixation during rapid head movements toward the ipsilesional side, likely contributing to the reported symptoms. Compensatory covert (occurring during the head movement) and overt (occurring after the head movement) saccades were present during head thrusts toward both the ipsilesional and contralesional sides. These saccades are fast phase eye movements generated to overcome deficits in the VOR, and changes in the latency and the frequency of saccade recruitment indicate plastic changes in the system. The tracings from the vHIT testing are shown in Figure 1.
 Figure 1: Video head impulse test (vHIT) results at initial evaluation. A: Left and right vestibulo-ocular reflex gain across peak head velocity during HIT. B and C: Head velocity (blue lines), slow phase eye velocity (ie, vestibular driven) eye movements (green lines), and saccadic eye movement (red lines) during HIT for the left (B) and right (C) horizontal canal. This figure is available in color online (www.jnpt.org).
Figure 1: Video head impulse test (vHIT) results at initial evaluation. A: Left and right vestibulo-ocular reflex gain across peak head velocity during HIT. B and C: Head velocity (blue lines), slow phase eye velocity (ie, vestibular driven) eye movements (green lines), and saccadic eye movement (red lines) during HIT for the left (B) and right (C) horizontal canal. This figure is available in color online (www.jnpt.org).The presence of unilateral VOR gain weakness, impaired DVA, reports of dizziness, impaired static and dynamic balance as shown on the MiniBEST, and reported functional limitations, recorded on initial examination, supported the presence of UVH. This was hypothesized to be caused by a decompensation associated with prolonged COVID-19 infection. The presence of UVH prompted the initiation of a physical therapy plan of care consistent with the clinical practice guidelines for management of vestibular hypofunction.18
InterventionM.W. participated in biweekly vestibular rehabilitation for 6 weeks. Vestibular rehabilitation included gaze stability, static balance, and dynamic balance exercises, detailed in Supplemental Digital Content Table A, available at: https://links.lww.com/JNPT/A461.
Gaze stability exercises included active sinusoidal head rotation in vertical and horizontal planes prescribed at high frequencies ranging between 140 and 170 bpm depending on the patient’s tolerance, directed by the use of a phone-based metronome, while keeping a visual target stable (target at arm’s length distance away and at eye level). Symptoms were assessed after each bout; if M.W. reported no increase in symptoms and the target remained in focus, the speed was increased by 10 beats per minute. Rest between repetitions was provided to allow symptoms to return to baseline. Static balance exercises sought to challenge postural stability and require slight corrections to maintain balance and avoid stepping corrections. Dynamic balance exercises sought to challenge M.W.’s dynamic postural stability as well as provoke mild symptoms during dynamic exercises. If the exercises did not provide an appropriate challenge or symptom response, they were progressed or modified on the basis of the Frequency, Intensity, Time, Type principle.31
Home exercises were monitored with a flow sheet and the patient was instructed to perform the exercises 3 times a day. The home program included a gaze stability exercise, along with a static and dynamic balance exercise that was performed in clinic and observed to be moderately challenging or produced mild symptoms. No specific habituation exercises were prescribed as it was expected that the patient would derive reduced sensitivity to motion as a result of the yaw and pitch plane gaze stability exercises.32 Each week, a progressively more difficult set of exercises was performed in person and at home while monitoring M.W.’s symptoms in response to treatment.
OUTCOMESM.W. demonstrated improvement on the DHI and the ABC compared with her initial assessment scores. Interestingly, despite improvements in dizziness handicap and balance confidence, a reduction in LSA score was observed. The distance walked during the 2MW and the score on the MiniBEST test both showed a clinically significant improvement from baseline without an increase of symptoms.24,25 Computerized DVA improved with turns toward the contralesional side (40% reduction in dynamic difference), while turns to the ipsilesional side did not show the same magnitude improvement (9.5% reduction in dynamic difference). vHIT testing at the posttreatment assessment demonstrated improved VOR function as a result of improved VOR gain in all ipsilesional canals (H-SCC = 15.9%, A-SCC = 13.7%, and P-SCC = 26.3%), while the contralesional side also demonstrated improved gains in all canals (Figure 2 ). Recruitment of corrective saccades (frequency and latency of the first saccade) also changed across all canals on both the ipsilesional and contralesional sides. Results for all measures collected at the pre- and posttreatment assessments, as well as percent change in each measure, are shown in the Table.
 Figure 2: Video head impulse test (vHIT) results at posttreatment assessment. A: Left and right vestibulo-ocular reflex (VOR) gain across peak head velocity during HIT. B and C: Head velocity (blue lines), VOR velocity (green lines), and saccadic eye movement (red lines) during HIT for the left (B) and right (C) horizontal canal. This figure is available in color online (www.jnpt.org).
Figure 2: Video head impulse test (vHIT) results at posttreatment assessment. A: Left and right vestibulo-ocular reflex (VOR) gain across peak head velocity during HIT. B and C: Head velocity (blue lines), VOR velocity (green lines), and saccadic eye movement (red lines) during HIT for the left (B) and right (C) horizontal canal. This figure is available in color online (www.jnpt.org).Finally, M.W. reported subjective improvement in dizziness and oscillopsia; she returned to the leisure activity of tennis without any increase in symptoms.
DISCUSSIONThe goal of this case study was to describe the reemergence, persistence, and response to rehabilitation for vestibular hypofunction signs and symptoms following hospitalization and substantial reduction in mobility from a COVID-19 infection in a patient with surgical history of VSR. Using patient-reported measures, performance-based measures of gaze stability, postural stability, and mobility (2MW), we documented deficits compared with normative values in this individual and report improvement following vestibular rehabilitation.
Based on the unique medical history of M.W. (unilateral VSR and prolonged inactivity as a result of COVID-19 infection) as well as the anatomical presentation of SCC weakness of vHIT testing, the authors hypothesize that the observed vestibular dysfunction was a result of decompensation of a prior compensated system. Compensation of the vestibular system and recovery of VOR is activity dependent33 and occurs through adaptation of the central nervous system. Decompensation has previously been used to describe recurrent vertigo.34 However, in this case decompensation is used to describe the reappearance of signs and symptoms consistent with UVH that were initially present post VSR. Through animal studies, we understand that following vestibular damage inactivity inhibits compensation and may lead to decompensation.35,36 Thus, for a person who has previously recovered from iatrogenic vestibular loss, maintenance of compensated vestibular system is dependent upon appropriate stimulation of the system.
To our knowledge there have been no reported cases of protracted vestibular decompensation in humans following prolonged hospitalization. In this case, the occurrence of a COVID-19 infection resulted in a 5-day ICU stay, followed by 13 weeks of at-home use of supplemental oxygen and requisite tubing, thereby greatly limiting head motion and functional mobility for the duration of this time, as reported by the patient. We hypothesize that this protracted period of limited mobility removed the needed multimodal stimulus for maintenance of vestibular compensation, resulting in the observed clinical presentation. Other hypotheses include vestibular dysfunction resulting from vestibular neuritis or dysautonomia, both linked to the SARS-COV-2 infection.4-7,37-39 However, clinical presentation and patient-reported history did not strongly support either of these alternative hypotheses.
Regardless of contributing mechanism, M.W. had a persistent, months long period of dizziness, oscillopsia, and imbalance that reflected alteration in her vestibular function. Her return to life activities following recovery from COVID-19 resulted in an increase in her symptoms and by itself was not a sufficient stimulus to facilitate recovery to her prehospitalization level of function. Thus, based on M.W.’s history and our examination findings, our clinical hypothesis guided the design of a vestibular rehabilitation program targeted at reducing DHI scores, improving ABC scores, and improving gaze and postural stability performance. Following the clinical practice guidelines18 for management of vestibular hypofunction this bout of rehabilitation likely resulted in the positive patient-reported outcomes as well as improvement in measures of gaze and postural stability often thought to be fixed following VSR.
Following completion of 6 weeks of vestibular rehabilitation M.W. experienced clinically meaningful reduction in DHI score (Minimal Clinically Important Difference (MCID) = 1820) and self-reported levels of dizziness and imbalance (visual analog scales23) as well as a clinically meaningful improvement in 2MW distance (MCID = 42.5 m25). Furthermore, M.W. reported returning to prior daily and recreational activities and demonstrated improved balance and function. These findings may point to the usefulness of vestibular rehabilitation in this unique case, despite the continued presence of gaze stability limitations (vHIT and DVA).40 Previous work completed by Millar et al40 also demonstrated that improvement in self-reported function following vestibular rehabilitation for vestibular neuritis was not mediated by improved VOR function. However, it is worth noting that in this case despite continued presence of VOR gain deficits, improvements in gain considered to be greater than clinically meaningful (0.06) were observed across all SCC.41 This finding of improved VOR gain following rehabilitation is of specific relevance as VOR gain has previously been shown to typically remain stable over time in individuals with UVH.42 Thus, the observed changes in M.W. further support the potential utility of vestibular rehab to create meaningful change in the case of a decompensated unilateral loss.
Changes in slow-phase, vestibular-driven eye movements (ie, VOR) have been shown to work in conjunction with compensatory saccades to improve gaze stability following recovery from vestibular injury.43 In addition to increases in VOR gain, changes were also observed in ipsilesional saccade recruitment (latency and frequency). Both the left H-SCC and the A-SCC had decreased frequency of saccades with a corresponding decrease in the latency of the first saccade, following rehab. Such findings are considered typical or consistent with the expected reciprocal relationship between increased VOR gain and reduced frequency of saccades.44 Interestingly, despite a substantial improvement in VOR gain in the left P-SCC following rehabilitation, an increased frequency of saccades and a longer latency of the first saccade were also observed. Similar findings were also observed in the right (contralesional) A-SCC and P-SCC. These paradoxical findings speak to the variability in motor response to vestibular rehabilitation, and previous studies have documented varied saccadic responses following vestibular rehabilitation.45-48 While only a single case study, such observations support the ability for rehabilitation, in the context of M.W.’s decompensated gaze stabilization system, to contribute to change in gaze stabilization mechanisms that are typically considered fairly static beyond the early acute stage after loss.49 Most importantly, functional use of gaze stabilization mechanisms as measured by DVA improved and self-reported dizziness handicap as measured by DHI diminished.
A limitation of this case report is a lack of objective findings of M.W.’s vestibular function in the period after her recovery from VSR and prior to her COVID infection. Meeting her goal of returning to previous baseline function is based on the subjective report that she had a full recovery without dizziness or imbalance after VSR recovery. Second, we acknowledge that we are unable to completely rule out these deficits resulting from vestibular nerve neuritis, considering the time course of symptoms and presentation to the rehabilitation clinic. However, the improvement following rehabilitation points to the potential value of vestibular rehabilitation in M.W. regardless of contributing mechanism.
SUMMARYIn conclusion, this case describes the plausible presentation of vestibular decompensation that occurred following an abrupt and significant decrease in functional mobility caused by hospitalization and subsequent supplemental oxygen treatment for COVID-19 infection. Vestibular rehabilitation targeted at gaze and postural stability and habituation was effective in reducing symptoms and facilitating recovery to M.W.’s pre-COVID-19 level of function. This case study adds valuable information to the limited literature on vestibular decompensation and treatment.
REFERENCES 1. Katsarkas A, Segal BN. Unilateral loss of peripheral vestibular function in patients: degree of compensation and factors causing decompensation. Otolaryngol Head Neck Surg. 1988;98(1):45-47. doi:10.1177/019459988809800108. 2. Reber A, Courjon JH, Denise P, Clément G. Vestibular decompensation in labyrinthectomized rats placed in weightlessness during parabolic flight. Neurosci Lett. 2003;344(2):122-126. doi:10.1016/S0304-3940(03)00433-6. 3. Wu F, Zhao S, Yu B, et al. A new coronavirus associated with human respiratory disease in China. Nature. 2020;579(7798):265-269. doi:10.1038/s41586-020-2008-3. 4. Giannantonio S, Scorpecci A, Montemurri B, Marsella P. Case of COVID-19-induced vestibular neuritis in a child. BMJ Case Rep. 2021;14(6):e242978. doi:10.1136/bcr-2021-242978. 5. Malayala SV, Raza A. A case of COVID-19-induced vestibular neuritis. Cureus. 2020;12(6):e8918. doi:10.7759/cureus.8918. 6. Motawea KR, Monib FA. New onset vertigo after COVID-19 infection. A case report. Indian J Otolaryngol Head Neck Surg. 2022;74(suppl 2):3009-3011. doi:10.1007/s12070-021-02715-5. 7. Saniasiaya J, Kulasegarah J. Dizziness and COVID-19. Ear Nose Throat J. 2021;100(1):29-30. doi:10.1177/0145561320959573. 8. Manzari L, Princi AA, De Angelis S, Tramontano M. Clinical value of the video head impulse test in patients with vestibular neuritis: a systematic review. Eur Arch Otorhinolaryngol. 2021;278(11):4155-4167. doi:10.1007/S00405-021-06803-8. 9. Guan Q, Zhang L, Hong W, et al. Video head impulse test for early diagnosis of vestibular neuritis among acute vertigo. Can J Neurol Sci. 2017;44(5):556-561. doi:10.1017/CJN.2017.202. 10. Cousins S, Cutfield NJ, Kaski D, et al. Visual dependency and dizziness after vestibular neuritis. PLoS One. 2014;9(9):e105426. doi:10.1371/JOURNAL.PONE.0105426. 11. Gupta VK, Thakker A, Gupta K. Vestibular schwannoma: what we know and where we are heading. Head Neck Pathol. 2020;14(4):1058-1066. doi:10.1007/s12105-020-01155-x. 12. Passier L, Doherty D, Smith J, McPhail SM. Vestibular rehabilitation following the removal of an acoustic neuroma: a systematic review of randomized trials. Head Neck Oncol. 2012;4(2):1-13. 13. Dutheil S, Lacour M, Tighilet B. Neurogenic potential of the vestibular nuclei and behavioural recovery time course in the adult cat are governed by the nature of the vestibular damage. PLoS One. 2011;6(8):e22262. doi:10.1371/JOURNAL.PONE.0022262. 14. Sadeghi SG, Minor LB, Cullen KE. Neural correlates of motor learning in the vestibulo-ocular reflex: dynamic regulation of multimodal integration in the macaque vestibular system. J Neurosci. 2010;30(30):10158-10168. doi:10.1523/JNEUROSCI.1368-10.2010. 15. Sadeghi SG, Minor LB, Cullen KE. Multimodal integration after unilateral labyrinthine lesion: single vestibular nuclei neuron responses and implications for postural compensation. J Neurophysiol. 2011;105(2):661-673. doi:10.1152/JN.00788.2010. 16. Peterka RJ, Statler KD, Wrisley DM, Horak FB. Postural compensation for unilateral vestibular loss. Front Neurol. 2011;2:57. doi:10.3389/FNEUR.2011.00057. 17. Lacour M, Helmchen C, Vidal PP. Vestibular compensation: the neuro-otologist’s best friend. J Neurol. 2016;263(suppl 1):S54-S64. doi:10.1007/s00415-015-7903-4. 18. Hall CD, Herdman SJ, Whitney SL, et al. Vestibular rehabilitation for peripheral vestibular hypofunction: an evidence-based clinical practice guideline: from the American Physical Therapy Association Neurology Section. J Neurol Phys Ther. 2016;40(2):124-155. doi:10.1097/NPT.0000000000000120. 19. Brandt T, DIeterich M. The dizzy patient: don’t forget disorders of the central vestibular system. Nat Rev Neurol. 2017;13(6):352-362. doi:10.1038/NRNEUROL.2017.58. 20. Jacobson GP, Newman CW. The development of the Dizziness Handicap Inventory. Arch Otolaryngol Head Neck Surg. 1990;116(4):424-427. doi:10.1001/ARCHOTOL.1990.01870040046011. 21. Powell LE, Myers AM. The Activities-specific Balance Confidence (ABC) Scale. J Gerontol A Biol Sci Med Sci. 1995;50A(1):M28-M34. doi:10.1093/GERONA/50A.1.M28. 22. Peel C, Baker PS, Roth DL, Brown CJ, Bodner EV, Allman RM. Assessing mobility in older adults: the UAB study of aging life-space assessment. Phys Ther. 2005;85(10):1008-1119. doi:10.1093/PTJ/85.10.1008. 23. Toupet M, Ferrary E, Grayeli AB. Visual analog scale to assess vertigo and dizziness after repositioning maneuvers for benign paroxysmal positional vertigo. J Vestib Res. 2011;21(4):235-241. doi:10.3233/VES-2011-0420. 24. Godi M, Franchignoni F, Caligari M, Giordano A, Turcato AM, Nardone A. Comparison of reliability, validity, and responsiveness of the mini-BESTest and Berg Balance Scale in patients with balance disorders. Phys Ther. 2013;93(2):158-167. doi:10.2522/PTJ.20120171. 25. Bohannon RW, Wang YC, Gershon RC. Two-minute walk test performance by adults 18 to 85 years: normative values, reliability, and responsiveness. Arch Phys Med Rehabil. 2015;96(3):472-477. doi:10.1016/j.apmr.2014.10.006. 26. McGarvie LA, MacDougall HG, Halmagyi GM, Burgess AM, Weber KP, Curthoys IS. The video head impulse test (vHIT) of semicircular canal function—age-dependent normative values of VOR gain in healthy subjects. Front Neurol. 2015;6:154. doi:10.3389/fneur.2015.00154. 27. Vital D, Hegemann SCA, Straumann D, et al. A new dynamic visual acuity test to assess peripheral vestibular function. Arch Otolaryngol Head Neck Surg. 2010;136(7):686-691. doi:10.1001/archoto.2010.99. 28. Schubert MC, Tusa RJ, Grine LE, Herdman SJ. Optimizing the sensitivity of the head thrust test for identifying vestibular hypofunction. Phys Ther. 2004;84(2):151-158. doi:10.1093/PTJ/84.2.151. 29. MacDougall HG, Weber KP, McGarvie LA, Halmagyi GM, Curthoys IS. The video head impulse test: diagnostic accuracy in peripheral vestibulopathy. Neurology. 2009;73(14):1134-1141. doi:10.1212/WNL.0b013e3181bacf85. 30. Halmagyi GM, Chen L, MacDougall HG, Weber KP, McGarvie LA, Curthoys IS. The video head impulse test. Front Neurol. 2017;8:258. doi:10.3389/fneur.2017.00258. 31. American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription. 11th ed. Philadelphia, PA: Wolters Kluwer; 2022. 32. Roller RA, Hall CD. A speed-based approach to vestibular rehabilitation for peripheral vestibular hypofunction: a retrospective chart review. J Vestib Res. 2018;28(3-4):349-357. doi:10.3233/VES-180633. 33. Lacour M, Tardivet L, Thiry A. Posture deficits and recovery after unilateral vestibular loss: early rehabilitation and degree of hypofunction matter. Front Hum Neurosci. 2022;15:776970. doi:10.3389/fnhum.2021.776970. 34. Ding CR, Gao YQ, Zhou YJ, Gu J, Wang J. Advantages of short-term personalized vestibular rehabilitation at home guided by professional therapist for treatment of decompensated vestibular vertigo. Curr Med Sci. 2021;41(4):687-694. doi:10.1007/s11596-021-2420-4. 35. Lacour M. Restoration of vestibular function: basic aspects and practical advances for rehabilitation. Curr Med Res Opin. 2006;22(9):1651-1659. doi:10.1185/030079906X115694. 36. Mitchell DE, Della Santina CC, Cullen KE. Plasticity within non-cerebellar pathways rapidly shapes motor performance in vivo. Nat Commun. 2016;7:11238. doi:10.1038/ncomms11238. 37. Dani M, Dirksen A, Taraborrelli P, et al. Autonomic dysfunction in ‘long COVID’: rationale, physiology and management strategies. Clin Med (Lond). 2021;21(1):e63-e67. doi:10.7861/CLINMED.2020-0896. 38. Eshak N, Abdelnabi M, Ball S, et al. Dysautonomia: an overlooked neurological manifestation in a critically ill COVID-19 patient. Am J Med Sci. 2020;360(4):427-429. doi:10.1016/j.amjms.2020.07.022. 39. Bosco J, Titano R. Severe post-COVID-19 dysautonomia: a case report. BMC Infect Dis. 2022;22(1):214. doi:10.1186/S12879-022-07181-0. 40. Millar JL, Gimmon Y, Roberts D, Schubert MC. Improvement after vestibular rehabilitation not explained by improved passive VOR gain. Front Neurol. 2020;11(February):79. doi:10.3389/fneur.2020.00079. 41. Chang TP, Schubert MC. Association of the video head impulse test with improvement of dynamic balance and fall risk in patients with dizziness. JAMA Otolaryngol Head Neck Surg. 2018;144(8):696-703. doi:10.1001/JAMAOTO.2018.0650. 42. Mahfuz MM, Millar JL, Schubert MC. Repeated video head impulse testing in patients is a stable measure of the passive vestibulo-ocular reflex. J Otol. 2021;16(3):128-137. doi:10.1016/J.JOTO.2020.12.002. 43. Schubert MC, Hall CD, Das V, Tusa RJ, Herdman SJ. Oculomotor strategies and their effect on reducing gaze position error. Otol Neurotol. 2010;31(2):228-231. doi:10.1097/MAO.0b013e3181c2dbae. 44. Schubert MC, Migliaccio AA, Santina CCD. Modification of compensatory saccades after aVOR gain recovery. J Vestib Res. 2006;16(6):285-291. doi:10.3233/ves-2006-16606. 45. Anson ER, Bigelow RT, Carey JP, et al. VOR gain is related to compensatory saccades in healthy older adults. Front Aging Neurosci. 2016;8:150. doi:10.3389/FNAGI.2016.00150. 46. Tian JR, Crane BT, Demer JL. Vestibular catch-up saccades in labyrinthine deficiency. Exp Brain Res. 2000;131(4):448-457. doi:10.1007/S002219900320. 47. Cerchiai N, Navari E, Sellari-Franceschini S, Re C, Casani AP. Predicting the outcome after acute unilateral vestibulopathy: analysis of vestibulo-ocular reflex gain and catch-up saccades. Otolaryngol Head Neck Surg. 2018;158(3):527-533. doi:10.1177/0194599817740327. 48. Navari E, Cerchiai N, Casani AP. Assessment of vestibulo-ocular reflex gain and catch-up saccades during vestibular rehabilitation. Otol Neurotol. 2018;39(10):e1111-e1117. doi:10.1097/MAO.0000000000002032. 49. Pogson JM, Taylor RL, Bradshaw AP, et al. The human vestibulo-ocular reflex and compensatory saccades in schwannoma patients before and after vestibular nerve section. Clin Neurophysiol. 2022;138:197-213. doi:10.1016/J.CLINPH.2022.02.014.
留言 (0)