
記住我

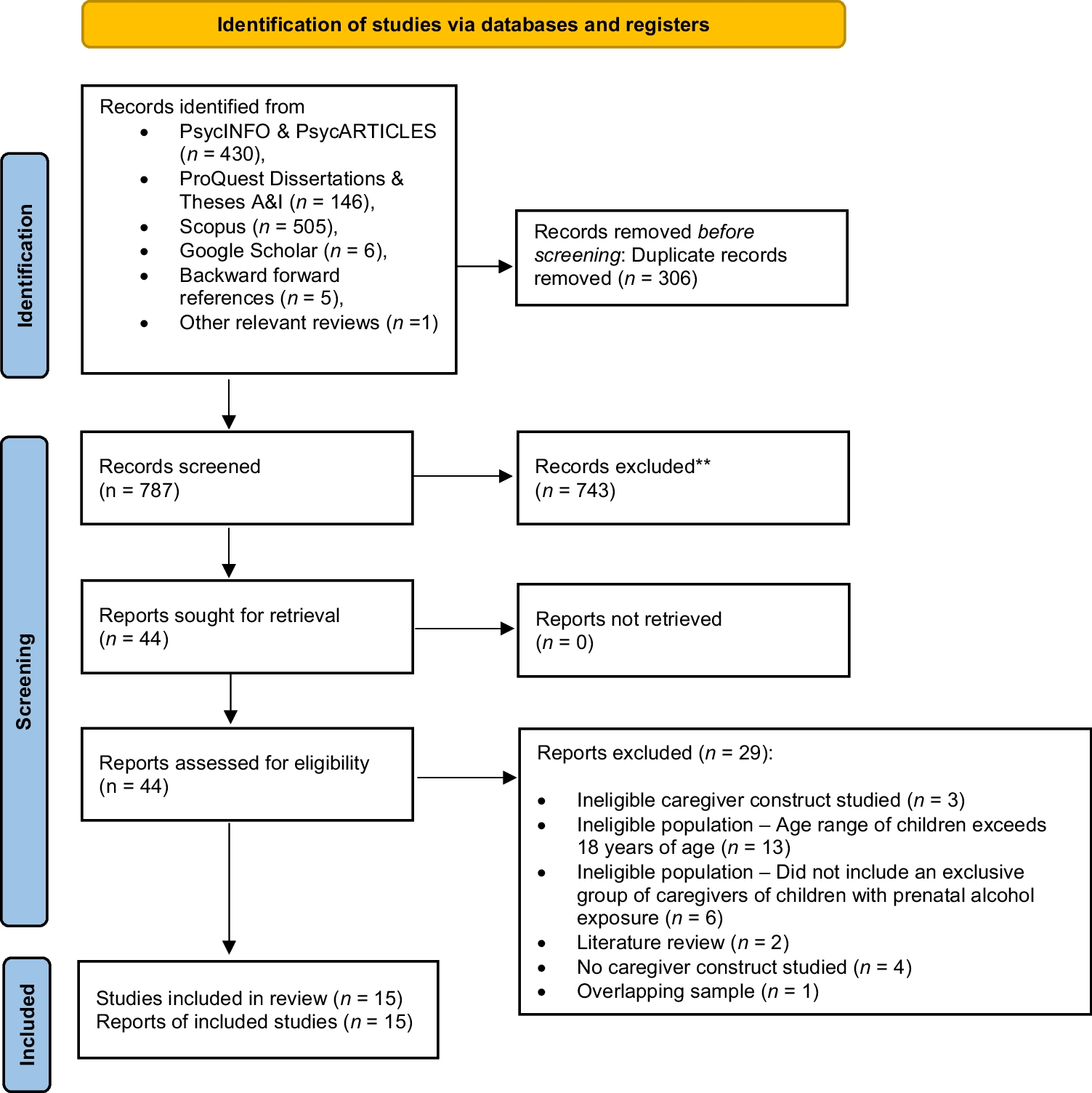
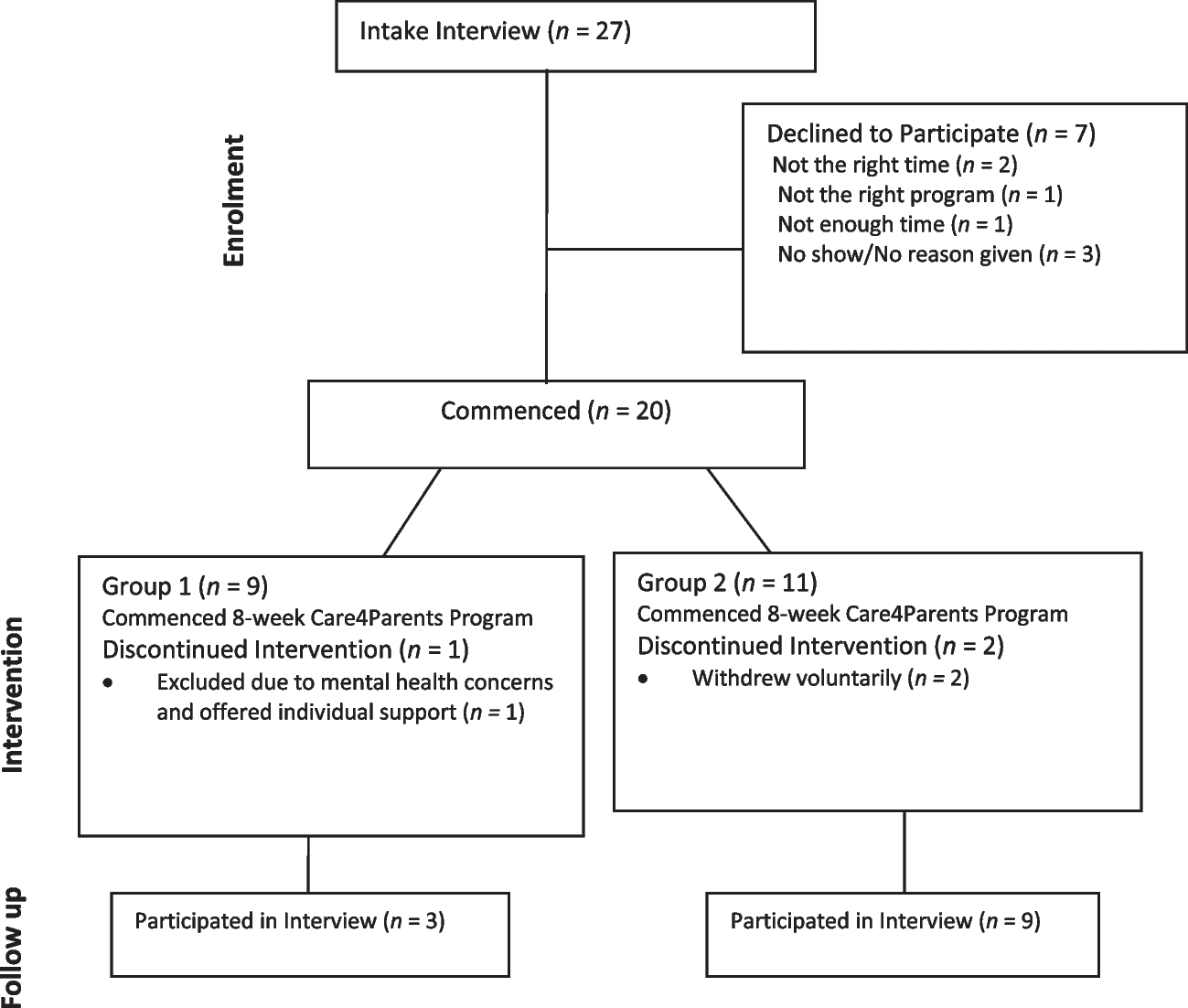



Detailed information on participants and procedures reported in the original study by Singh et al. (2020c) are briefly summarized here to provide the context for this study. A total of 216 caregivers were randomized into a mindfulness program, a psychoeducation program, or a control group program (i.e., inservice training-as-usual). Seventy-two participants were assigned to each experimental condition, clustered by group homes to avoid contamination of training across the three experimental conditions. Each group home had 6 caregivers, and thus, 12 clusters were assigned to each experimental condition. Those who participated in the mindfulness condition had an average age of 40.68 years (range = 19 to 61), had an average service of 15.11 years (range = 1 to 37), and included 42 females. Those in the psychoeducational condition had an average age of 37.89 years (range = 19 to 61), had an average service of 13.76 years (range = 1 to 35), and included 38 females. The participants in the control condition had an average age of 39.61 years (range = 19 to 61), had an average service of 15.17 years (range = 1 to 39), and included 39 females. There were no statistically significant differences in age, years of service, or sex distribution across the three groups (p > 0.05). Some participants in each experimental condition were lost during implementation, i.e., 3, 5, and 9 in the mindfulness, psychoeducation, and inservice training-as-usual conditions, respectively. Figure 1 presents a CONSORT participant flow diagram.
Fig. 1 ProcedureExperimental Design
ProcedureExperimental DesignA three-arm cluster RCT design was used, with two active experimental conditions and a control condition: a mindfulness program, a psychoeducation program, and an inservice training-as-usual program. Training in each of the three programs was for 3 days, followed by implementation of the programs for 32 weeks.
Experimental ConditionsMindfulness Program. The mindfulness experimental condition used the 3-day stepped-care mindfulness component from the full MBPBS program to teach basic meditations and related contemplative practices (Singh et al., 2020b). The mindfulness program included the following standard Buddhist meditation practices: (1) Samatha, walking, and insight meditations; (2) five hindrances (i.e., sensory desire, ill will, sloth and torpor, restlessness and remorse, and doubt); (3) the four immeasurables (i.e., lovingkindness, compassion, empathetic joy, and equanimity [equipoise]); (4) the three poisons (i.e., attachment, anger, and ignorance [doubt]); (5) beginner’s mind; (6) informal mindfulness practices; and (7) practicing ethical precepts (e.g., refrain from harming anyone, taking that which is not given, and incorrect or false speech). Following instructions in the meditation practices, the caregivers were encouraged to develop a daily formal meditation practice for about 20 min that involved focused meditation and different combinations of the other meditations.
Psychoeducational Program. A psychoeducational program was developed specifically for this condition. The program had two key functions. First, it was designed to teach caregivers key aspects of workplace stress, how to recognize it, and how to reduce it. Second, it was designed to educate caregivers on how to meet the needs of individuals with ID and ASD. This included information on positive methods of responding to the behavioral excesses and deficits of the individuals and their social and instructional relationships with the individuals. The program emphasized the following: (1) how to relate skillfully with the individuals (i.e., effective communication that is positive, attentive, and nonjudgmental); (2) how to be accepting of the individual, especially when they are engaged in behaviors that the caregivers found challenging to manage (i.e., reducing automatic negative responses, no use of aversive or punishing consequences, responding in a calm manner that showed the caregiver understood the behavioral functions of the challenging behaviors, as well as the role of emotion dysregulation in their behavior); and (3) how to use evidence-based and practice-based evidence for the treatment of individuals with ID and ASD.
Inservice Training-as-Usual Program. The agency responsible for the group homes provided their standard inservice training on the care and management of individuals with ID and ASD, as well as booster sessions to supplement the new employee training. The yearly updated training curriculum included (1) behavior management; (2) crisis intervention plans; (3) 1-on-1 staffing interventions; (4) emergency medications for severe aggressive behavior to self, peers, and staff; (5) physical restraints; (6) aversive contingencies and punishment strategies; and (7) skills training. All newly employed caregivers receive the basic and supplemental new employee training regardless of additional program-specific training that they may later receive as employees of the agency. Thus, the caregivers in all three arms of the study had received the standard inservice training as part of their new employee training. The caregivers in the control condition received an additional three days of Inservice Training-as-Usual program to equalize the training conditions across the three arms of the study.
MeasuresData on caregiver quality of life variables were obtained from the agency’s Human Resources Department personnel file. These data were recorded by each caregiver’s supervisor and verified by staff from the Human Resources Department. Data on client quality of life variables were obtained from the agency’s Quality Assurance Department. The data were verified by the group home supervisor or discipline-specific supervisors for occurrence and accuracy of reporting.
Caregiver VariablesProgressive Discipline. This was used as a risk management system by the agency. It allowed and supported a caregiver disciplinary system that provided a graduated range of agency responses to unsatisfactory employee performance or behavioral issues. By policy, progressive discipline consisted of a 5-step process that included a verbal warning, a written warning, a poor performance evaluation, a performance improvement plan, and separation (i.e., termination).
Call-In. This was defined as an unplanned absence on a specific day when a caregiver calls in as soon as possible but no less than 2 h before the start of the shift to notify their immediate supervisor of an absence from work. It also included unscheduled leave requests.
Days Absent. This was defined as unauthorized absence from work beyond legitimate requests for unplanned leave (e.g., family and/or medical issues) or unexpected events (e.g., car problems).
Medical Referral. This was defined as a written order from the caregiver’s primary care doctor or specialist clinical professional (e.g., psychiatrist) to obtain specified medical services due to work-related issues.
Hospitalization. This was defined as the level of care in a hospital as an inpatient requiring at least an overnight stay due to work-related issues.
Caregiver Turnover. This was defined as caregiver separation from the agency due to work-related issues. Separation due to regular life events, such as family relocation, were not counted as caregiver turnover.
Client VariablesLearning Objectives. These were defined as the learning objectives specified in the client’s Individualized Support Plan (ISP), which was developed by the treatment team to reflect the clinical and support needs of the client. Caregivers provided instructions as specified in the client’s ISP and recorded each learning objective that was mastered to competency by the client. Identified skills for the client were task analyzed, and each component was defined as a learning objective. Mastery criterion was provided by discipline staff (e.g., psychology, physical therapy, occupational therapy, etc.) responsible for developing the learning objective.
Behavioral Episodes. These were defined as a client hitting, biting, scratching, punching, kicking, slapping, or destroying property. Caregivers recorded each instance of a behavioral event on an incident reporting form at the point of occurrence and entered it in the agency’s incident management database.
Use of Physical Restraints. This was defined as a brief physical hold of an aggressive client by a caregiver when there was imminent danger of physical harm to the client, peers, or staff and when the behavior could not be controlled with verbal redirection. Caregivers recorded each instance of the use of physical restraint at the point of occurrence and entered it in the agency’s incident management database.
Emergency (Stat) Medication. Emergency medication was prescribed by a physician and administered by a registered nurse for behavioral or psychiatric emergencies. These medications were not prescribed for medical or other conditions. Emergency medication was prescribed for the calming of a client who was aggressive and could not be managed by other means, including physical restraints. Each administration was counted as one event as recorded by a registered nurse in the client’s Medication Administration Record.
Medical Emergencies. This was defined as a medical event that required medical examination by a physician or a nurse practitioner, as needed. It excluded those events that required only first aid treatment or resulted in hospitalization. Each medical emergency was recorded by a physician or a nurse practitioner in the client’s medical records.
Hospitalizations. This was defined as a level of care in a hospital as an inpatient requiring at least an overnight stay due to behavioral or psychiatric issues and excluded those for medical or other conditions. Each hospitalization was recorded by a registered nurse in the client’s medical records.
Aggression to Staff. This was defined as any aggressive act by a client directed at a caregiver, with physical contact, requiring medical examination, first aid, or medical care. Each instance of staff injury was recorded on an incident reporting form at the point of occurrence and entered in the agency’s incident management database.
Aggression to Peers. This was defined as any aggressive act by a client directed at a peer, with physical contact, requiring medical examination, first aid, or medical care. Each instance of peer injury was recorded on an incident reporting form at the point of occurrence and entered into the agency’s incident management database.
Level of Supervision. This was defined as the level of supervision when a client’s aggressive or destructive behavior could not be managed through clinical interventions, and the safety of the client, staff, and peers was in question. It included enhanced level of supervision (i.e., 1-to-1 or 2-to-1 staffing) required that was ordered by a physician or clinical psychologist as determined by the client’s treatment team and documented in the client’s treatment plan.
Data AnalysesThe main goal of the data analyses was to evaluate the differences across three experimental conditions in terms of caregiver and client outcome variables. Considering that the caregiver and client outcome variables represent ratio-level data, a group count for an entire condition was used instead of a count for individuals within a condition because traditional analyses for RCTs were deemed unsuitable for this study (Singh et al., 2020c). The primary reason for this is that the variables are not at the individual level, which would be required for standard RCT analyses.
To address this challenge, change across time within each condition was examined by treating each group as an n of 1. This approach enabled the computation of the count of each variable for each condition including means and SD across the 32 weeks of the study, thereby ensuring a robust analysis of the differences between conditions. Analysis of variance (ANOVA) was employed to compare the three groups. This method was chosen due to its ability to handle ratio-level data and its suitability for comparing multiple groups simultaneously. Additionally, ANOVA accounts for variance within and between groups, making it a highly reliable statistical tool for analyzing the data in this study.
Following the ANOVA, post-hoc tests were conducted to further explore the differences between the three experimental conditions. We used Welch’s ANOVA to address unequal variances across groups and Bonferroni adjustment for the number of post-hoc tests. These tests helped to identify the specific pairs of conditions that were significantly different from one another, thus providing a more detailed understanding of the results. Statistical significance was determined using a p-value threshold of <0.05. This criterion is widely accepted within the scientific community and ensures that any observed differences between groups are unlikely to have occurred by chance alone. The effect sizes were estimated using partial eta squared (η2), a measure indicating the proportion of total variance in the dependent variable attributable to each independent variable while controlling for others. Following Cohen (1988), an effect size of 0.01 was considered small, 0.06 medium, and 0.14 large. These thresholds provided an assessment of the practical significance of our findings beyond mere statistical significance.
留言 (0)