Patient population
We performed a multicenter case-control study. The entire cohort included 155 consecutive KS patients and 95 age-matched healthy controls. Inclusion criteria were: (i) a documented KS karyotype (47,XXY) for patients and (ii) written informed consent for both groups. KS patients with total testosterone levels lower than 12 mol/l received testosterone replacement treatment according to the current guidelines [15, 16]. Medical students, residents, physicians, nurses, and administrative staff were enrolled as healthy controls. Patients underwent a complete medical and family history evaluation. KS patients and controls were recruited from the 4 Italian centers involved; none of the centers were in high goiter risk areas. Thyroid function and thyroid antibodies (Ab) were assessed. Study participants who had elevated plasma Thyroid Peroxidase (TPO) Ab and Thyroglobulin (Tg) Ab above 350 IU/ml as well as thyroid parenchyma heterogeneity with reduced echogenicity were considered Hashimoto’s thyroiditis (HT) patients. The study was approved by the Ethics Committee of the University of Campania “L. Vanvitelli”–University of Campania L. Vanvitelli” Hospital-AORN Ospedale dei Colli” (no. 1489, 26.10.2015).
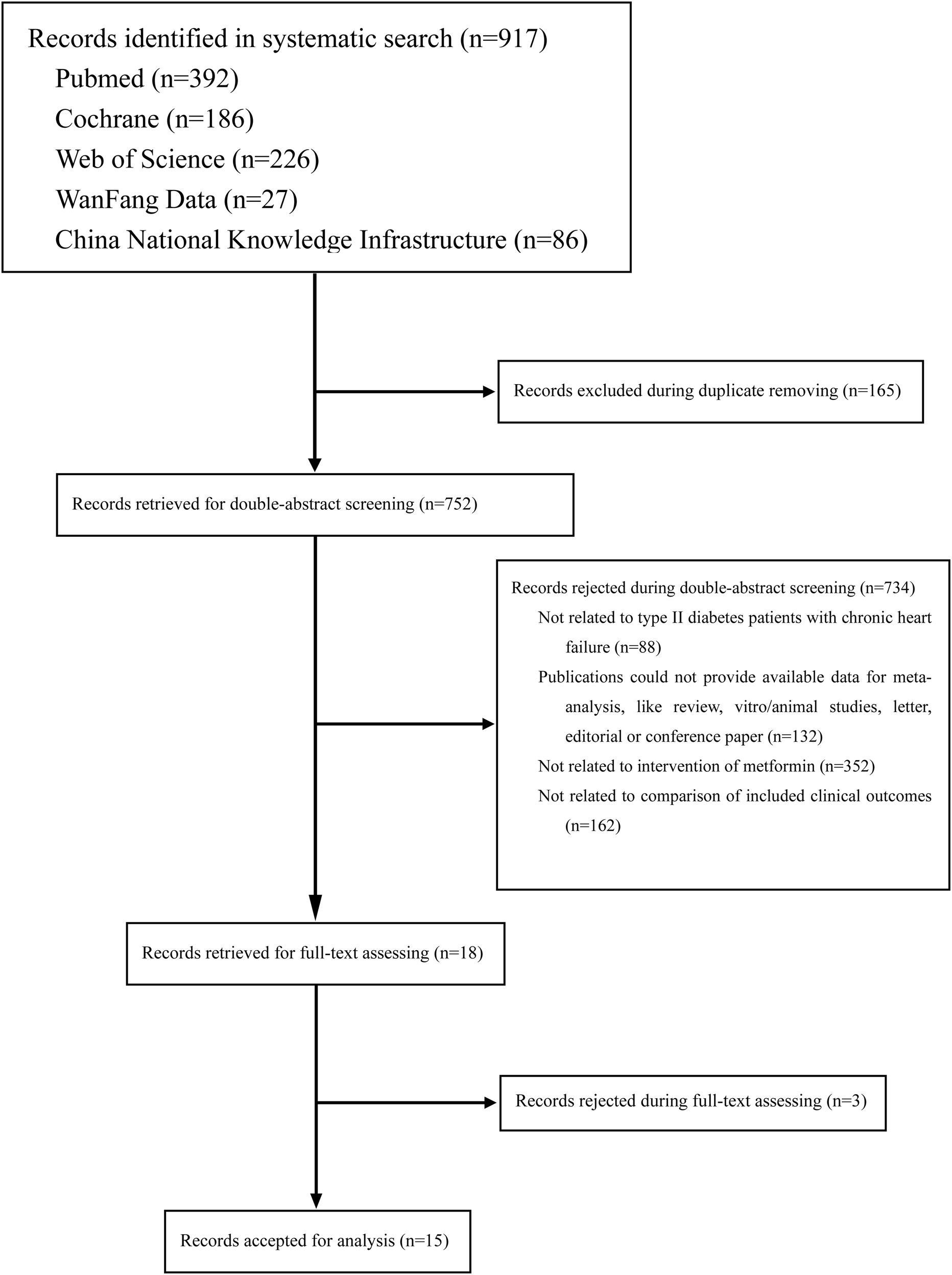
Thirty three patients were excluded due to lack of complete data or because they were lost to follow-up.
Sample collection
Venous blood (2 mL) from study participants was collected from blood banks at KING center hospitals during the same period of KS and control recruitment. Samples, blind of identification, were immediately sent to the laboratory facility in each hospital for analysis of TSH, FT4, FT3, TPOAb, TgAb, and total testosterone. The measurements were done on the same day in primary tubes after blood centrifugation at 3200 rpm for 15 min.
Biochemical data
As patients attending different centers institutions were recruited, different methods were used to obtain biochemical data. In most cases, serum TSH, FT4, and FT3 concentrations were measured by chemiluminescent immunometric assay (Roche Diagnostics, Mannheim, Germany), as previously described [1]. The manufacturer’s reference limits were: TSH (0.35–5.5 mIU/L), FT4 (10.2–31 pmol/L), and FT3 (3.5–6.5 pmol/L). Detection limit for TSH was 0.005 μIU/mL, and functional sensitivity 0.014 μIU/mL. Thyroid function alteration was classified according to American Thyroid Association guidelines [17]. Clinically overt hyperthyroidism was classified as TSH undetectable to less than 0.1 mIU/liter and FT3 and FT4 above the normal range; subclinical hyperthyroidism as TSH undetectable to less than 0.1 mIU/liter and FT3 and FT4 in the normal range without exogenous T4 intake; clinically overt hypothyroidism as TSH above the upper limit of the normal range (5 mIU/liter in our assay) and FT4 below 10.2 pmol/L; subclinical hypothyroidism as TSH above the upper limit of the normal range and FT4 in the normal range [11, 12]. Total testosterone was measured by immunoassay using a commercially available automated immunoassay system (LIASON Analyzer; DiaSorin, Saluggia, Italy).
Exclusion criteria
KS patients with mosaic forms of chromosomal aneuploidy or any other structural or numerical karyotype anomaly, with AZF microdeletions were excluded from the study, as previously described [1]. A further exclusion criterion was secondary hypothyroidism defined as TSH undetectable to less than 0.1 mIU/liter and FT4 and FT3 in the lower range without exogenous T4 intake. Enrolled participants with clinically overt thyroid dysfunction or with a personal or family history of thyroid disease were also excluded.
Thyroid ultrasound and fine needle aspiration
Thyroid US was performed by the same blinded investigator in each center. US and color flow Doppler examinations were mainly performed with a LOGIQ 9 system (GE Healthcare, Chalfont St. Giles, England), a commercially available real-time US system equipped with 5–14 MHz (M12L) and 2.5–7 MHz (7 L) linear array transducers. During the examination, the patient remained in the supine position, and US heads were applied to the right and left side of the thyroid. Four US images were acquired for each participant. The following US characteristics were recorded for each nodule: round shape (ratio of short axis to long axis >0.5), abnormal echogenicity, calcification, cystic aspect, and a peripheral color Doppler pattern.
A conventional 23 G needle was used to collect FNA samples. All sampling procedures were performed by single operator to eliminate operator bias. Sample collection was carried out as follows: (i) neck skin was sterilized with the proper antiseptic; (ii) a clear US view of the most suspicious solid thyroid nodules (based on ACR-TIRADS score) was obtained in the center of the field of view; (iii) each nodule was evaluated in terms of size, vascularity, echogenicity, and calcifications, and data were recorded and archived. FNA was performed when indicated based on nodule characteristics and size following guidelines [17, 18]. Thyroid US was performed by the same blinded investigator in each center in both patients and controls. The same reporting method was used in all centers. Specifically, US risk-stratification system was applied to assess the risk of malignancy and the need for biopsy based on nodule characteristics and size and the data were collected in a standard excel-file used in all the centers.
Statistical analysis
Data were analyzed using SPSS software (version 17). Mean and standard deviation were calculated for continuous variables. Statistical analyses were performed using Student’s t-test. TSH and testosterone levels were compared using Mann–Whitney test, and TPO antibodies using chi-square test.




留言 (0)