
記住我

Vaccinations for COVID-19 (severe acute respiratory syndrome coronavirus 2 [SARS-CoV-2] infection) are increasing across the US population, partly because of the September 2021 federal mandate requiring vaccination for some civil employees, subsequent employer-driven mandates, ongoing effort to administer booster vaccinations, and expansion of vaccinations into the pediatric population. This is coincident with the return of patients to hospitals and imaging centers for non–COVID-19-related routine, surveillance, and screening imaging, many of which were postponed during the height of the pandemic.
In December 2020, both manufacturers of messenger RNA (mRNA) vaccines widely in use in the United States (Pfizer-BioNTech and Moderna) included lymphadenopathy/axillary swelling and tenderness as nonserious adverse events (AEs) in safety data reports for the Centers for Disease Control and Prevention (CDC).1,2 However, the potential impact of this phenomenon on medical care was not widely appreciated by the medical community or the lay public at that time.
At our large urban academic medical center in one of the largest first- and second-surge COVID epicenters, we followed New York State Department of Health guidelines and began to offer vaccines to hospital staff in December 2020 and to high-risk patients on January 11, 2021, including those older than 65 years or with high-risk comorbidities such as cancer.
Soon after initiating vaccinations, we noticed unexpected unilateral asymmetric axillary and subpectoral adenopathy on chest computed tomography (CT) in patients outside of clinical settings where adenopathy might occur (lymphoma, breast cancer, connective tissue disease). Contemporaneously, case series of unilateral axillary adenopathy at breast imaging concerning for breast malignancy, but which proved to be transient and temporally related to the administration of vaccination for COVID, were reported.3,4
Electronic medical record (EMR) review confirmed that many patients with unilateral axillary adenopathy, a few of whom were in fact imaged for axillary or chest wall pain or mass, had recently been vaccinated in the ipsilateral arm. These clinical observations prompted the hypothesis that asymmetric axillary or subpectoral lymph nodes at chest CT ipsilateral to the arm of vaccine administration may occur more frequently than reported to the CDC.
To explore the hypothesis, we performed a retrospective study, as no large series had evaluated the frequency of COVID-19 vaccine–related adenopathy on CT chest, and previous studies were confined to the breast imaging literature.
MATERIALS AND METHODSThis retrospective study was performed with institutional review board waiver of authorization and consent (i21-00263).
Study PopulationThe institution EMR (Epic Systems, Verona, Wisconsin) was searched for outpatients older than 18 years who had a chest CT 2 to 25 days after receiving at least one dose of COVID-19 vaccine, between December 15, 2020, and February 12, 2021. Search terms based on “imaging studies” included CT chest, lung screening, CT chest with IV contrast, and CT chest without IV contrast, and the “immunizations administered” search term was COVID-19 vaccine.
Study CohortWe included consecutive outpatients who received SARS-CoV-2 vaccination(s) in the same site, administered at our institution with details recorded directly in our EMR by our administering staff (not patient recollection), 2 to 25 days before a chest CT scan. Exclusion criteria include age less than 18 years, inpatients, and vaccine administered in contralateral arms or at an outside facility. All other patients were included in this study (Table 1).
TABLE 1 - Inclusion and Exclusion Criteria Inclusion Criteria Exclusion Criteria Age ≥18 y Age <18 y Men and women Outpatients Inpatients Contrast or noncontrast chest CT 2–25 d after the initial or 2nd vaccine dose Vaccine doses administered same arm Vaccine doses administered contralateral arms Vaccine administered at home institution; details recorded directly into EMR by staff Vaccine administered outside institutionThe EMR was searched for the following data: age and sex, vaccine administration date and manufacturer, anatomic site of administration of initial and second doses of SARS-CoV-2 vaccine, CT scan date(s), and underlying health conditions in conjunction with indications for imaging.
Imaging ReviewTwo-millimeter-thick axial chest CT slices on soft tissue window settings (W/L 350/50) were reviewed in a blinded fashion by 2 fellowship-trained thoracic radiologists with 17 years' (G.B.-A.) and 11 years' (J.P.A.) of experience, with discrepancies adjudicated by a third fellowship-trained thoracic radiologist (W.H.M.) with 16 years' experience. Reviewers knew subjects had received COVID-19 vaccinations but were blinded to other clinical details, including date and side of vaccine administration.
Reviewers recorded the longest bidirectional orthogonal measures, including the fatty hilum if present, of the largest axillary and subpectoral lymph node ≥3 mm bilaterally (Fig. 1), and the image number and series where measurements were obtained. If the largest lymph nodes were less than 3 mm in size, this was recorded as “no nodes.” A >30% discrepancy in measurements between reviewers was adjudicated by the third fellowship-trained thoracic radiologist.
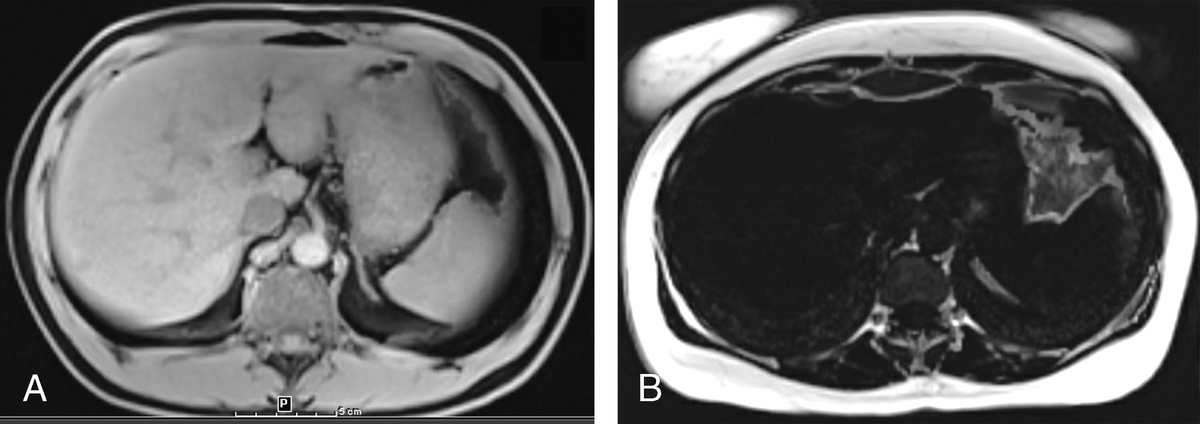
 FIGURE 1:
FIGURE 1: Nodal measurement technique. A 67-year-old female recipient of right arm vaccination 20 and 3 days before CT. The longest orthogonal measures were recorded for the largest node in each station, inclusive of the fatty hilum, and then averaged to obtain the mean nodal diameter. Note the absence of enlarged nodes in the left axilla contralateral to vaccine administration.
Orthogonal measurements were averaged to determine a mean nodal diameter, as reactive nodes are often nonround (Fig. 1), as opposed to typically rounded malignant nodes.5,6 To use therefore only short-axis measures would underestimate the reactive nodal response. Because cortical thickness measures are inaccurate at a single axial level, we measured longest orthogonal diameters of the node, inclusive of the fatty hilum, if present, rather than cortical thickness.
Statistical AnalysisStatistics were performed on IBM SPSS Statistics, Armonk, New York.
The difference in the mean nodal diameter of the largest axillary and subpectoral node, as compared with the contralateral side, was calculated. Correlation between the side of vaccination and the difference in the mean nodal diameter was performed using a Spearman rank correlation; a subsequent Spearman rank correlation was performed excluding patients with underlying disease as detailed previously.
A P value of <0.05 was considered statistically significant.
RESULTSThe search criteria identified 183 subjects. Fourteen subjects with vaccinations administered at outside facilities were excluded, as the side (laterality) of vaccination was not recorded in the EMR. Thirty-one subjects were excluded because of contralateral first and second vaccine administrations. Two subjects who received only a single vaccine dose were included. Of the remaining 138 patients included in the analysis, 25 had vaccine administered in the right arm and 113 had vaccine administered in the left arm, in the deltoid muscle in all cases (Fig. 2). All vaccines were manufactured by Pfizer-BioNTech, administered under Food and Drug Administration (FDA) Emergency Use Authorization at our institution, with details recorded directly into the EMR by our staff; otherwise, subjects were excluded (Fig. 3).
 FIGURE 2:
FIGURE 2: Flowchart of subject inclusion and exclusion.
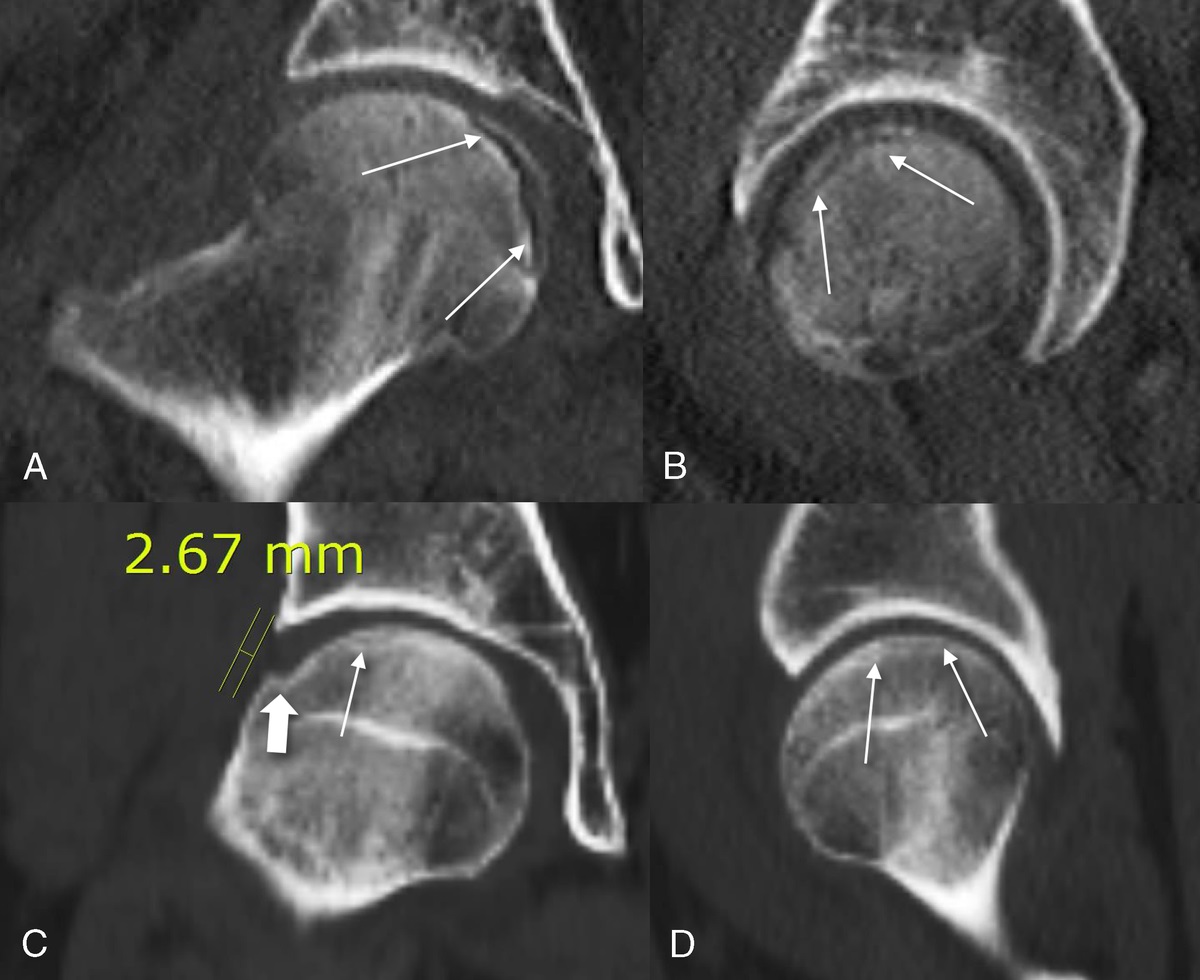
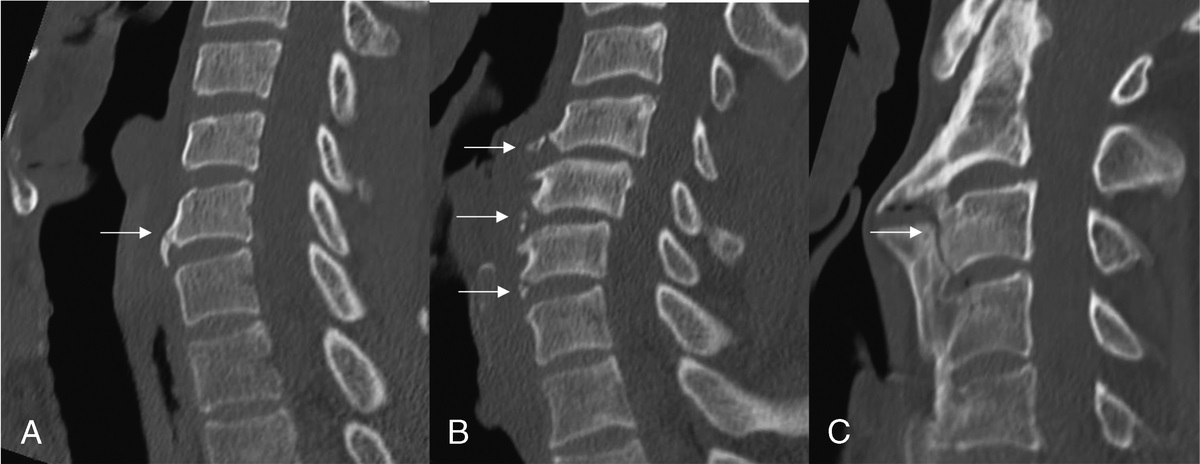
 FIGURE 3:
FIGURE 3: Asymmetric right axillary adenopathy in a 58-year-old woman after left lower lobectomy for a benign pneumocytoma. Vaccinated on January 24, 2021, and February 15, 2021, at an outside facility, site not recorded. Axillary (A) and coronal (B) CTs performed on February 15, 2021, depict asymmetric right axillary adenopathy (arrow). C, Prevaccination CT performed on June 10, 2020, shows absence of axillary adenopathy. The subject was excluded from study cohort because of unconfirmed laterality of vaccine administration. Prospective knowledge of vaccine laterality may favor follow-up rather than further workup.
There were 81 women and 57 men, with a mean ± SD age of 74.4 ±11.7 years.
Chest CT scans were obtained 14.1 ± 9.6 days after vaccine administration; after the first dose, the mean was 18.8 ± 7.6 days, and after the second dose, the mean was 12.9 ± 10.0 days. A total of 142 scans were obtained, 43 subjects had a CT scan after the first vaccine dose, 91 subjects had a CT scan after the second vaccine dose, and 4 subjects had scans after both the first and second vaccine doses—in these cases, only the second CT was used in analysis. Fifty-five CTs were performed after administration of intravenous contrast.
Choice of Threshold Level of Nodal Mean Diameter AsymmetryBecause symmetric axillary lymph nodes may be seen in a range of settings and because nonenlarged positron emission tomography (PET) avid nodes associated with COVID-19 vaccine have been reported,7–9discrepancy, rather than a threshold nodal size, was used as a determinant of abnormality. The mean nodal size discrepancy considered as positive for asymmetry was set by analyzing the range of mean diameter nodal differences between 5 and 9 mm, correlated with percentage of lymph nodes ipsilateral and contralateral to the side of injection in the 138 subjects (Table 2).
TABLE 2 - Number (Percentage) Asymmetric Lymph Nodes Correlated With Side of Vaccine Administration at a Range of Mean Nodal Diameter Size Differences Difference in mean nodal diameter between sides, mm ≥5 ≥6 ≥7 ≥8 ≥9 Asymmetric larger lymph nodes ipsilateral to vaccination 60 (43.8) 46 (33.3) 32 (23.3) 9 (18.8) 10 (7.2) Asymmetric larger lymph nodes contralateral to vaccination 7 (5.1) 6 (4.3) 5 (3.6) 3 (2.2) 2 (1.4) r and P values r = 0.26; P = 0.002 r = 0.26; P = 0.003 r = 0.34; P < 0.001 r = 0.17; P = 0.042 r = 0.33; P = 0.047Some patients had asymmetric nodes in both stations; hence, absolute numbers exceed the number of patients.
A mean diameter nodal discrepancy of 6 mm or greater was set as the threshold to define asymmetry, providing a reasonably large sample of both ipsilateral and contralateral asymmetric nodes. Thus, subjects were categorized as positive for asymmetric lymph nodes if there was a discrepancy of ≥6 mm between the largest mean nodal diameters in contralateral nodal stations. Subjects were otherwise classified as negative for asymmetric lymph nodes, for each nodal station.
Using a discrepancy of ≥6 mm in mean nodal diameters between corresponding contralateral nodal stations, 48 of 138 subjects (34.7%) showed asymmetric axillary or subpectoral lymph nodes.
A total of 46 asymmetric lymph nodes in 42 patients were identified ipsilateral to the side of vaccination (Table 3; Figs. 4, 5). A total of 6 asymmetric lymph nodes were identified in 6 patients contralateral to the side of vaccination; 4 of these 6 patients also had smaller ipsilateral nodes. There is a significant correlation of the side of asymmetric lymph nodes with the side of vaccination (r = 0.26; P = 0.003; Table 2).
TABLE 3 - Number of Asymmetric Lymph Nodes and Number of Patients With Asymmetric Lymph Nodes (≥6-mm Difference in Mean Nodal Size) Correlated With Side of Injection Vaccination Site Asymmetric Right Axillary Nodes Asymmetric Right Subpectoral Nodes Asymmetric Left Axillary Nodes Asymmetric Left Subpectoral Nodes Ipsilateral Asymmetric Lymph Nodes Asymmetric Right Nodes Per Patient Asymmetric Left Nodes Per Patient Right (n = 25) 1* 4* 0 0 5 5* 0 Left (n = 113) 4 2 18* 23* 41 6 37* FIGURE 4:
FIGURE 4: Asymmetric ipsilateral left axillary lymph nodes in a 91-year-old woman vaccinated on January 14, 2021, and February 4, 2021, in the left arm. CT performed on February 16, 2021, depicts asymmetric left axillary lymph nodes and stranding (arrow).
 FIGURE 5:
FIGURE 5: Asymmetric ipsilateral level III left subpectoral and axillary lymph nodes with soft tissue stranding in a 77-year-old woman vaccinated on January 14, 2021, and February 2, 2021, in the left arm. A, Axillary CT performed on February 5, 2021, at the level of the clavicular heads depicts asymmetric left level III subpectoral (open arrow) and axillary lymph nodes (arrow) and soft tissue stranding extend into the subcutaneous tissue (arrow). B, More inferiorly, at the level of the aortic arch vessels, asymmetric left axillary nodes are present (arrow) with stranding of the axillary fat (arrowhead) extending into the soft tissues of the arm (arrows). Follow-up CT performed on August 4, 2021 (6 months later), at the same levels demonstrates disappearance of the level III subpectoral nodes (C), and regression of axillary lymph nodes and stranding (D).
To eliminate potentially confounding effects of underlying conditions that may be associated with axillary or subpectoral adenopathy, we reexamined the data after exclusion of 29 subjects with breast cancer, lymphoma, sarcoidosis, and connective tissue diseases (Fig. 6; Table 4).
 FIGURE 6:
FIGURE 6: Asymmetric left axillary and subpectoral lymph nodes in a 38-year-old woman with systemic lupus erythematosus vaccinated on December 16, 2020, and January 9, 2021, in the left arm. A, Chest CT performed on February 1, 2021, depicts asymmetric benign-appearing left axillary (arrow) and subpectoral (open arrow) lymph nodes with central hilar fat. B, Prevaccination chest CT performed on October 9, 2019, depicts similar although smaller left axillary (arrow) and subpectoral (open arrow) lymph nodes. The subject was excluded from the second tranche analysis because of a preexisting disease associated with axillary adenopathy.
TABLE 4 - Diagnoses Associated With Axillary or Subpectoral Adenopathy in 29 Patients Excluded in Second Analysis Underlying Diagnosis N = 29 Breast cancer 8 Breast cancer + lymphoma 2 Lymphoma 4 Lymphoma + RA 1 RA 6 RA + Sjogrens syndrome 1 Sjogrens syndrome 1 Sclerodema 2 Systemic lupus erythematosis 2 Sarcoidosis 1 Sarcoidosis + lymphoma 1RA indicates rheumatoid arthritis.
The prevalence of asymmetric lymph nodes ipsilateral and contralateral to vaccine administration was similar in this subcohort of 109 patients. Thirty-six enlarged lymph nodes in 32 patients were identified that correlated with the side of vaccination (Table 5). Five asymmetric lymph nodes were identified in 5 patients contralateral to the side of vaccination (Table 5). There is a significant correlation of the side of asymmetric lymph nodes with the side vaccination (r = 0.31; P = 0.002).
TABLE 5 - Number of Asymmetric Lymph Nodes and Number of Patients With Asymmetric Lymph Nodes (≥6-mm Difference in Mean Nodal Size) Correlated With Side of Injection in 109 Patients Vaccination Site Asymmetric Right Axillary Nodes Asymmetric Right Subpectoral Nodes Asymmetric Left Axillary Nodes Asymmetric Left Subpectoral Nodes IpsilateralThis study is the first to report the high prevalence at chest CT of axillary and subpectoral lymph nodes correlated with SARS-CoV-2 vaccination incidentally detected outside the setting of malignancy screening or surveillance. Thirty-five percent of subjects had asymmetric lymph node enlargement in the axillary or subpectoral nodal stations at chest CT, in 30% ipsilateral to COVID-19 vaccine administration and therefore plausibly related to the vaccine, and in 4% contralateral to vaccine administration. Furthering the credible association between vaccine administration and adenopathy in our study, only subjects with vaccine administration details recorded directly into the EMR at our institution were included. In some studies, associating adenopathy with vaccines administration laterality was not examined,10 was not described,3 or relied on patient recollections.4
This prevalence is significantly higher than that reported to the CDC by Pfizer-BioNTech (Pfizer) and Moderna around the time of the Emergency Use Authorization. In December 2020, Pfizer-BioNTech reported this nonserious AE in 11% and 15% of subjects after initial and second doses of vaccine, respectively; Moderna reported similar rates at 12% and 16%, respectively, in subjects aged 16 to 64 years, and 6% and 8%, respectively, in subjects 65 years and older.1,2
The significantly higher prevalence of vaccine-related nodal enlargement in our series versus FDA reported AEs likely reflects the more sensitive detection of lymph nodes at CT as compared with subject self-reporting. In contradistinction to our quantitative imaging data based on lymph node measurements, subjective swelling or pain was collected among solicited (Moderna) and unsolicited (Pfizer) non serious AEs that trial participants were asked to qualitatively record in symptom diaries during the 7 days after vaccination.1,2 In the Pfizer cohort, because lymphadenopathy was an unsolicited AE, the true incidence rate may be higher.11 Accessible reports made to the CDC do not clarify whether vaccine recipients were specifically asked to palpate these areas or just note the presence of perceived pain and swelling.
Importantly, in our study, even when subjects with underlying conditions that might predispose them to axillary or subpectoral adenopathy were excluded from the analysis, the prevalence of asymmetric ipsilateral mean diameter nodal measurements remained almost identically elevated (29.4% [32/109] of subjects) above manufacturers' reported rates, indicating that this observation likely relates to hyperplasia from the vaccine, rather than underlying causes, including malignancy (Fig. 7).
 FIGURE 7:
FIGURE 7: Asymmetric left subpectoral and axillary lymph nodes in a 75-year-old woman with stage IB lung cancer treated with left lower lobectomy in August 2020 without evidence of recurrence and vaccinated on January 15, 2021, and February 4, 2021, in the left arm. A, Axillary CT performed on February 23, 2021, depicts new asymmetric left axillary and interpectoral lymph nodes, which, in the absence of correlation with vaccination history, might raise concern for tumor recurrence. B, Prevaccination CT performed July 20, 2020, shows absence of nodes. C, Follow-up CT performed on August 18, 2021, demonstrates that asymmetric nodes are smaller but persist for 6 months after the final vaccine dose. No evidence of cancer recurrence.
Interestingly, our prevalence rate of nodes ipsilateral to vaccine administration at 29% to 30% is significantly higher than the 9% at chest CT in patients with thoracic malignancy reported by Nishino et al12 but is lower than that reported on a recent breast imaging study at 44%.10
Lymph node enlargement as a sequela of SARS-CoV-2 vaccination has been widely reported at imaging inclusive of the axilla and subpectoral regions, notably breast imaging3,4 and PET-CT.7–9 Several imaging societies and institutions therefore proposed management guidelines after detection of possible COVID vaccine–related adenopathy.11,13–17
Earliest reports of vaccine-related adenopathy in the breast imaging literature led to the February 2021 Society of Breast Imaging recommendation that routine breast imaging should be scheduled before or 4 to 6 weeks after the second vaccine dose.9 A subsequent report questioned whether follow-up should be lengthened to 12 to 16 weeks after vaccination.18 More recently, a breast imaging study by Wolfson et al10 with longer follow-up of postvaccination patients reported that in the 44% of patients with axillary adenopathy on at least one study, adenopathy resolution was variable, persisting up to 43 weeks after vaccination. These authors suggest therefore that there should be no delay in screening mammography due to recent vaccination. Subsequently, the Society of Breast Imaging issued a revised recommendation in February 2022 that screening mammography in asymptomatic average-risk women should not be delayed around COVID-19 vaccinations.17
Igual-Rouilleault et al19 prospectively performed axillary ultrasounds 1 week before and a week after the first and second Pfizer vaccine doses, and found an increase in total visible nodes, maximum diameter, and cortical thickness of nodes in almost all patients after vaccination. A more significant lymph node response occurred after the second vaccination and in SARS-CoV-2–naive patients compared with those who were previously infected.
Radiotracer uptake as a sequela of SARS-CoV-2 vaccination, usually in the absence of nodal enlargement, is increasingly reported; nodal uptake was seen in 54% of 140 subjects8 and 46% of 728 subjects, in which only 10% of nodes were enlarged.9 In another series, only 1 FDG avid node was abnormally enlarged based on short-axis diameter >10 mm.7
It is important that imagers, particularly thoracic imagers, are aware of SARS-CoV-2 vaccine–related nodal response and include post–SARS-CoV-2 vaccination in the broad differential for unilateral axillary and subpectoral asymmetric lymph nodes. Correlation with the dates and laterality of SARS-CoV-2 vaccination when available should be included in imaging reports, as some nonimager clinicians may not yet be aware of this phenomenon.
Pragmatic management should be tailored to clinical scenarios. A conservative approach is warranted in low-risk patients, such as in screening studies, versus adenopathy in settings such as oncologic surveillance, which should consider the patient's pretest probability of metastases versus benign reaction to the vaccination in management (Figs. 6, 7).13 Some guidelines address reporting and management based on risk stratification12 or that vaccine be administered contralateral to the side of known breast and head and neck cancers.13
Adenopathy consequent to vaccinations is a recognized phenomenon, described after smallpox,20 Bacille Calmette-Guerin,21,22 human papillomavirus,23 and H1N1 influenza A virus vaccines.20,23 Hyperplastic adenopathy is more common after vaccines that evoke a robust immune response, such as the Pfizer mRNA vaccines in use at our institution. Hyperplastic adenopathy recognized by these vaccine developers1,2 was reported to the FDA as a nonserious AE attributed to local reactions and systemic effects.
It is interesting that in 6 subjects (4.3%), asymmetric adenopathy was contralateral to the side of vaccine administration. When conditions possibly associated with axillary or subpectoral adenopathy were excluded from the cohort, this was unchanged at 4.6%, suggesting the limited impact of these diseases in this observation. The etiology of contralateral asymmetrically enlarged lymph nodes is unclear.
Limitations of Our StudyThere are several limitations to our study. We did not use an absolute size or a clinical threshold metric for nodal enlargement. Rather, we applied a level of disparity between the mean diameters of the largest lymph node at each bilateral station, to account for the frequent occurrence of axillary lymph nodes in particular, that reactive nodes are typically nonround, and that varying degrees of benign enlargement range across the population. This approach proved highly appropriate, as most asymmetric nodes were not enlarged based on standard CT criteria. That isotope-avid nodes after SARS-CoV-2 vaccination at PET-CT have overwhelmingly been reported as nonenlarged further supports this approach.7–9
When we designed our protocol, there were no studies detailing the time to appearance or persistence of nodal enlargement after vaccination; therefore, we conservatively chose 2 to 25 days after either vaccination dose as the time range for CT examinations. Vaccinated subjects with CTs outside this time frame may therefore have been missed.
We did not review follow-up CTs to determine if and when asymmetric nodes resolve after vaccination. Resolution of after vaccination supraclavicular reactive adenopathy has been reported at 2 weeks.24 Axillary adenopathy is recently reported as persisting up to 43 weeks after vaccination.10
Our study population is highly skewed toward older subjects. During this initial period of limited vaccine availability, following New York State Department of Health COVID-19 Vaccination Program Phase 1–3 guidelines, we vaccinated hospital employees, patients 65 years and older, and patients younger than 65 years with high-risk comorbidities. Although many hospital employees are younger than 65 years, few had CT examinations during the study period. Based on the data reported to the CDC by Pfizer and Moderna, reactive adenopathy may be more common in younger patients. Further study of a younger cohort may show the prevalence of reactive adenopathy in this group to be even higher than we report,9 and may be increasingly important as vaccines are rolled out to the pediatric population.
Our study includes only subjects who received a single-manufacturer mRNA vaccine (Pfizer-BioNTech). Whether results are applicable to other mRNA vaccines, as is likely, or to other vaccine platforms is not addressed.
CONCLUSIONSThe prevalence of asymmetric axillary and subpectoral lymph nodes after SARS-CoV-2 vaccination at chest CT is 2 to 3 times more frequent than initially reported to the CDC by manufacturers.
With increasing COVID-19 vaccination rates, including vaccination of pediatric populations and administration of booster doses to large segments of the population,25 correlation of asymmetric nodes to vaccine administration timing and site may preclude undue anxiety and unnecessary further testing, and allow conservative management in the low risk. Radiologists should include post–SARS-CoV-2 vaccination in the broad differential for asymmetric axillary and subpectoral adenopathy, as clinically appropriate.
REFERENCES 1. Centers for Disease Control and Prevention. Local Reactions, Systemic Reactions, Adverse Events, and Serious Adverse Events: Pfizer-BioNTech COVID-19 Vaccine. December 13, 2020. Available at: https://www.cdc.gov/vaccines/covid-19/info-by-product/pfizer/reactogenicity.html. Accessed March 30, 2021. 2. Centers for Disease Control and Prevention. Local Reactions, Systemic Reactions, Adverse Events, and Serious Adverse Events: Moderna COVID-19 Vaccine. December 20, 2020. Available at: https://www.cdc.gov/vaccines/covid-19/info-by-product/moderna/reactogenicity.html. Accessed March 30, 2021. 3. Ahn RW, Mootz AR, Brewington CC, et al. Axillary lymphadenopathy after mRNA COVID-19 vaccination. Radiol Cardiothorac Imaging. 2021;3:e210008. 4. Mehta N, Sales RM, Babagbemi K, et al. Unilateral axillary adenopathy in the setting of COVID-19 vaccine. Clin Imaging. 2021;75:12–15. 5. Steinkamp HJ, Hosten N, Richter C, et al. Enlarged cervical lymph nodes at helical CT. Radiology. 1994;191:795–798. 6. Shin J, Shin S, Lee JH, et al. Lymph node size and its association with nodal metastasis in ductal adenocarcinoma of the pancreas. J Pathol Transl Med. 2020;54:387–395. 7. Schroeder DG, Jang S, Johnson DR, et al. Frequency and characteristics of nodal and deltoid FDG and 11C-choline uptake on PET performed after COVID-19 vaccination. AJR Am J Roentgenol. 2021;217:1–11. 8. Skawran S, Gennari AG, Dittli M, et al. [(18)F]FDG uptake of axillary lymph nodes after COVID-19 vaccination in oncological PET/CT: frequency, intensity, and potential clinical impact. Eur Radiol. 2021;22:1–9. 9. Cohen D, Krauthammer SH, Wolf I, et al. Hypermetabolic lymphadenopathy following administration of BNT162b2 mRNA Covid-19 vaccine: incidence assessed by [18F]FDG PET-CT and relevance to study interpretation. Eur J Nucl Med Mol Imaging. 2021;48:1854–1863. 10. Wolfson S, Kim E, Plaunova A, et al. Axillary adenopathy after COVID-19 vaccine: no reason to delay screening mammogram. Radiology. 2022;304:E57. 11. Grimm L, Destounis S, Dogan B, et al. Society of Breast Imaging: SBI Recommendations for the Management of Axillary Adenopathy in Patients with Recent COVID-19 Vaccination. Available at: https://www.sbi-online.org/Portals/0/Position%20Statements/2021/SBI-recommendations-for-managing-axillary-adenopathy-post-COVID-vaccination.pdf. Accessed on March 8, 2021. 12. Nishino M, Hatabu H, Ricciuti B, et al. Axillary lymphadenopathy after coronavirus disease 2019 vaccinations in patients with thoracic malignancy: incidence, predisposing factors, and imaging characteristics. J Thorac Oncol. 2022;17:154–159. 13. Lehman CD, D'Alessandro HA, Mendoza DP, et al. Unilateral lymphadenopathy post COVID-19 vaccination: a practical management plan for radiologists across specialties. J Am Coll Radiol. 2021;18:843–852. 14. Becker AS, Perez-Johnston R, Chikarmane SA, et al. Multidisciplinary recommendations regarding post-vaccine adenopathy and radiologic imaging: Radiology Scientific Expert Panel. Radiology. 2021;300:E323–E327. 15. SNMMI Statement: The Effect of COVID-19 Vaccination on FDG PET/CT. Available at: https://www.snmmi.org/NewsPublications/NewsDetail.aspx?ItemNumber=36729. Accessed March 30, 2021. 16. National Comprehensive Cancer Network. Recommendations of the NCCN COVID-19 Vaccination Advisory Committee. Available at: https://www.nccn.org/covid-19/pdf/COVID-19_Vaccination_Guidance_V2.0.pdf. Accessed on June 15, 2021. 17. Grimm L, Srini A, Dontchos B, et al. Revised Society of Breast Imaging Recommendations for the Management of Axillary Adenopathy in Patients with Recent COVID-19 Vaccination. 2022. Available at: https://www.sbi-online.org/Portals/0/Position-Statements/2022/SBI-recommendations-for-managing-axillary-adenopathy-post-COVID-vaccination_updatedFeb2022.pdf. Accessed March 30, 2021. 18. Nguyen DL, Ambinder EB, Myers KS, et al. COVID-19 vaccine–related axillary adenopathy on breast imaging: follow-up recommendations and histopathologic findings. AJR Am J Roentgenol. 2021;218:997–998. 19. Igual-Rouilleault AC, Soriano I, Quan PL, et al. Unilateral axillary adenopathy induced by COVID-19 vaccine: US follow-up evaluation. Eur Radiol. 2022;32:3199–3206. 20. Cohen J, Powderly WG, Opal SM. Infectious diseases. Elsevier Health Sci. 2017;2:145. 21. Newfield L, Naschitz JE, Yeshurun D. BCG-induced axillary lymph-adenitis in the adult. Harefuah. 1990;119:199–200. 22. Krysztopa-Grzybowska K, Paradowska-Stankiewicz I, Lutyńska A. The rate of adverse events following BCG vaccination in Poland. Przegl Epidemiol. 2012;66:465–469. 23. Studdiford J, Lamb K, Horvath K, et al. Development of unilateral cervical and supraclavicular lymphadenopathy after human papilloma virus vaccination. Pharmacotherapy. 2008;28:1194–1197. 24. Kim B, Park Y, Kim EK, et al. Supraclavicular lymphadenopathy after COVID-19 vaccination in Korea: serial follow-up using ultrasonography. Clin Imaging. 2021;79:201–203. 25. Özütemiz C, Potter DA, Özütemiz AÖ, et al. Lymphadenopathy after the third COVID-19 vaccine. Curr Probl Cancer case rep. 2021;4:100127.
留言 (0)