1. IntroductionPoor oral health conditions, such as periodontitis, carious teeth, or loss of teeth, are frequent health problems in the general population [
1]. These poor oral health conditions not only adversely affect oral health but can also be systematically associated with or trigger the occurrence of various diseases [
2]. For example, periodontitis causes a local inflammatory reaction in the oral cavity and triggers systemic inflammatory responses. Additionally, the loss of teeth and oral hygiene behaviors are associated with the increased or decreased risk of various systemic diseases, including diabetes, cardiovascular diseases, certain cancers and neurodegenerative diseases [
1,
3,
4,
5].Meniere’s disease is accompanied by recurrent rotatory vertigo attacks, tinnitus and hearing loss, possibly caused by an endolymphatic accumulation in the cochlear duct and a decrease in the endocochlear potential of the vestibular labyrinth [
6,
7]. Reports suggest a prevalence of 17 and 43 per 100,000 people in studies conducted in Japan and Finland, respectively [
8,
9]. Despite the high prevalence of the disease, its causes, related factors and mechanisms are not well-known. Several suggested factors for Meniere’s disease include systemic inflammation, infection, obesity, salt, caffeine and alcohol consumption, smoking, stress, trauma and autoimmune disease [
10].Previous studies have found that poor oral hygiene and periodontitis are associated with systemic inflammation. Regarding the association between Meniere’s disease and oral health, previous case reports show that Meniere’s disease may be caused by tooth- related maxilla or mandibular pathology [
11].
However, to date, there have been few longitudinal studies on the link between the occurrence of Meniere’s disease and general oral health or related behaviors, such as loss of teeth, tooth brushing and dental scaling in the general population. Identifying the risk of Meniere’s disease associated with oral health would provide evidence to support the importance in preventing this disease. This may reduce the burden of Meniere’s disease and related complications.
We hypothesized that a poor oral health status is related to an increased risk of Meniere’s disease and better oral hygiene behavior is associated with a decreased risk for this condition. Therefore, this study aimed to longitudinally investigate the relationship between the occurrence of Meniere’s disease and oral health examination estimates in a nationwide cohort database.
2. Methods 2.1. Data SourceThe National Health Insurance Database of the Korean National Health Insurance Service (NHIS), a public data source representing the entire South Korean population, was used in the present study. The South Korean government supervises and supports the NHIS, which covers nearly 97% of South Koreans. The rest of the population is covered by the Medical Aid Program, administered by the NHIS [
12,
13]. The NHIS collected Korean national health information data and provided this research database to make useful data available to health researchers. Health researchers can access this research database with the NHIS approval. To obtain approval for the database, we requested access via an application form, research proposal and application from the institutional review board on the National Health Insurance Sharing Service homepage. Access to the dataset was approved after review by the NHIS (dataset number: NHIS -2022-01-313).NHIS members are recommended to undergo a standardized health checkup, including oral health screening every 1–2 years. From the NHIS database, the adult participants (aged ≥ 20 years) who had oral health screenings between January 2003 and December 2003 (n = 2,415,963) were included in the present study. The database included the claims database of diagnoses, treatments, prescriptions, demographics and socioeconomic information. It also contained individual health screening information, including body mass index, blood pressure and laboratory tests. Individuals were requested to answer questionnaires about their lifestyle, including their oral hygiene behaviors. During the health screening, dentists examined the participants for dental problems, such as tooth loss. The number of missing teeth (regardless of etiology) was classified as 0, 1–7, 8–14, or ≥15 according to a quartile [
1,
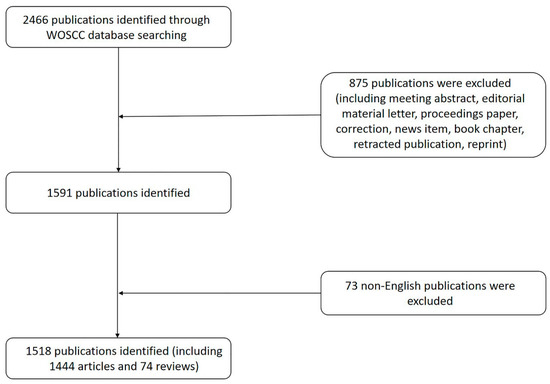
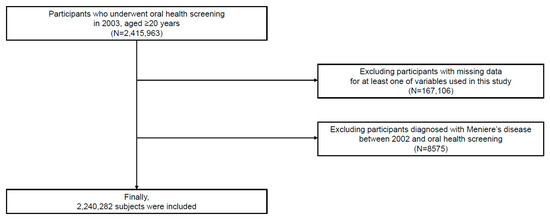
14]. The institutional review board approved this study (2021–07–034) and informed consent was waived owing to the anonymity of the data. 2.2. Study PopulationAmong the participants (n = 2,415,963), the participants whose data were missed on at least one variable of interest (n =167,106) were excluded. Further, the participants with a history of Meniere’s disease between January 2002 and the time of the oral health examination were excluded (n = 8575). Ultimately, the study included 2,240,282 participants (
Figure 1). 2.3. Definition and VariablesThe date of the oral health examination was set as the index date. The data on the baseline characteristics, such as age, sex, household income and body mass index, were collected at the index date. The information on smoking habits (never, former smoker and current smoker), alcohol consumption (frequency per week) and regular physical exercise (frequency per week) was obtained by questionnaires. The comorbidities of the individuals were identified between January 2002 and the index date using the claim of diagnosis (International Classification of Diseases, Tenth Revision, ICD-10), prescription, laboratory test results or self-reported information in the questionnaire (
Appendix A).Periodontitis was identified according to the following criteria between January 2002 and the index date: (1) two or more claims of the ICD-10 codes K052-054 (acute periodontitis [K052], chronic periodontitis [K053] and periodontitis [K054]) with at least one claim of related treatment codes (
Appendix B) or (2) periodontal pocket detection by a dentist during the oral health screening [
15,
16]. A dentist assessed the number of missing teeth during the oral examination. The oral hygiene behaviors collected via the questionnaires showed the frequency of daily tooth brushing and dental scaling within the past year. The most recent data were applied to the analysis if the participant received more than two oral health examinations. 2.4. Study OutcomesThe study outcome was the development for Meniere’s disease based on two or more claims of the diagnostic code H810 with a previous audiometric examination (claim code: E6931–E6937, F6341–F6348) [
17,
18]. The participants were followed up one day after the date of the oral health examination until the occurrence of Meniere’s disease, death or December 2020, whichever came first. 2.5. Statistical Analysis
The baseline characteristics of the periodontitis-positive and periodontitis-negative groups were compared using the chi-square test and an independent t-test. Since the statistics for analyzing the differences between the groups are based on sample size, false positives can occur with chi-square tests and independent t-tests for data with large sample sizes. Therefore, we used the standardized differences and considered those >0.1 to be noteworthy.
The Kaplan–Meier survival curves and the log-rank test were used to evaluate the association between the oral health status and the oral hygiene behaviors for the incident risk of Meniere’s disease. To estimate the incidence of Meniere’s disease, the number of Meniere’s disease events was divided by the sum of person-years. Cox’s proportional hazard regression was used and the hazard ratios (HRs) and 95% confidence intervals (CIs) were estimated to determine the effect of the oral health parameters on the occurrence of Meniere’s disease. A multivariable regression model was constructed with adjustments for age, sex, body mass index, household income, alcohol consumption, smoking status, regular physical activity and comorbidities (hypertension, diabetes mellitus, dyslipidemia, atrial fibrillation, cancer and renal disease). The oral health parameters were adjusted separately in a multivariable analysis due to the multicollinearity.
A subgroup analysis was conducted to determine the association between the presence of periodontitis and the development of Meniere’s disease according to age, sex and covariates. For the sensitivity analysis, we excluded the participants with Meniere’s disease occurring within 1 year from the index date to minimize the possibility of reverse causality and performed multivariable analyses (landmark analyses). Schoenfeld’s residuals were used to examine the assumption of the hazard proportionality. The proportional hazard assumption was not violated. All the statistical analyses were performed using the statistical analysis system software (SAS version 9.2, SAS Institute, Cary, NC, USA). All the values were considered to be statistically significant when the p-values < 0.05.
3. ResultsAmong the 2,240,282 participants, the average age of the included participants was 42.3 ± 12.8 years and 66.4% were male. Of the sample body, 13,957 (0.6%) participants had more than 15 missing teeth, 923,661 (41.2%) brushed their teeth at least three times a day and 512,833 (22.9%) underwent dental scaling within the last year. The baseline characteristics and a comparative analysis between the periodontitis-positive and the periodontitis-negative groups are shown in
Table 1.Meniere’s disease occurred in 112,106 (5.0%) participants within a median duration of 16.7 (interquartile range 16.2–17.2) years. The Kaplan–Meier survival curves of the participants without Meniere’s disease according to the oral health parameters are shown in
Figure 2. The risk of Meniere’s disease increased in the participants with periodontitis (ppp
Supplementary Table S1).In the multivariable analysis, periodontitis was associated with the occurrence of Meniere’s disease (adjusted HR 1.18, 95% CI 1.14–1.22, ppp for trend pp for trend p = 0.003) (
Table 2). A subgroup analysis showed that the presence of periodontitis and oral health parameters were consistently associated with the occurrence of Meniere’s disease, regardless of covariates (
Figure 3). The presence of periodontitis was more strongly associated with Meniere’s disease in the participants The sensitivity analysis showed that the presence of periodontitis, the number of missing teeth, the frequency of tooth brushing and dental scaling within one year were consistently associated with the occurrence of Meniere’s disease, even in the landmark analysis (
Supplementary Tables S2 and S3). 4. Discussion
The main findings of the present study were that periodontitis and increased tooth loss were correlated with an increased risk of the occurrence of Meniere’s disease. However, increased tooth brushing and dental scaling showed a lower risk of Meniere’s disease. Based on the results, the hypothesis that poor oral health status was related to an increased risk of Meniere’s disease and better oral hygiene behavior with a decreased risk of Meniere’s disease was accepted.
Periodontitis and poor oral health have systemic inflammatory implications and are associated with various systemic diseases. Periodontitis reportedly increased the risk of cardiovascular and several vascular diseases [
19,
20]. Tooth loss, an indicator of poor oral health, was positively correlated with a higher risk of hypertension [
21] and stroke [
22]. Studies showed that the bacteremia can be caused by periodontitis and poor oral hygiene, [
23] and inflammation induced by oral infection produced pro-inflammatory cytokines [
24]. Evidence revealed that pro-inflammatory cytokines, such as tumor necrosis factors and interleukins, play a role in the development of Meniere’s disease [
7]. However, there have been few longitudinal studies on the relationship between Meniere’s disease and oral inflammation in a large population. A case report suggested that intraosseous dental pathology was the cause of Meniere’s disease, but the evidence was insufficient. The results of our study are meaningful because they demonstrate a novel association between oral inflammation and Meniere’s disease in a population-based cohort in a longitudinal setting.Conversely, behaviors that decrease oral inflammation, such as professional dental care and tooth brushing, can reduce the risk of certain systemic diseases. An increased number of tooth brushing significantly reduced the occurrence of cardiovascular disease in patients with hypertension [
4] and attenuated the risk of diabetes [
15]. Dental scaling decreased the risk of end-stage renal disease [
25]. A recent meta-analysis showed that dental scaling could reduce the risk of atrial fibrillation [
26]. Improved oral hygiene with brushing and dental scaling may also reduce the risk of Meniere’s disease through changes in the oral microbiome and a reduced inflammatory burden. Since periodontal pathogens and the production of pro-inflammatory cytokines are significantly reduced by dental scaling or brushing [
27,
28], a reduced inflammatory response through improved oral hygiene may reduce the risk of Meniere’s disease. Our study was consistent with previous research and provided new information on the association between Meniere’s disease and oral health behaviors, suggesting that individuals with better oral hygiene behaviors have a reduced risk of Meniere’s disease.A subgroup analysis showed that periodontitis was more strongly associated with Meniere’s disease in younger and low BMI subgroups in this study. Meniere’s disease showed a higher prevalence in older and obese individuals [
10]. Epidemiological studies reported obesity and old age as risk indicators for periodontitis [
29,
30]. Our findings suggested that, although Meniere’s disease and periodontitis are less common in young and non-obese individuals, the systemic inflammation associated with periodontitis may significantly influence the development of Meniere’s disease in younger individuals and individuals with a low BMI.This study had several limitations. First, our dataset did not include residual confounders that could affect the occurrence of Meniere’s disease. Carious teeth were excluded from the analyses due to the relationship between dental caries and systemic inflammation was unclear [
31]. Second, the study included only Korean subjects; hence, the results may differ for other races/ethnicities. Third, the periodontitis participants accounted for only 3.3% of all the participants. This finding may be attributed to the strict definition of periodontitis (defined as two or more diagnostic and treatment codes) and the ages of the included participants (age ≥ 20 years) [
32]. Fourth, the study could not evaluate the different degrees of periodontitis severity due to the lack of information on the detailed attachment loss. Fifth, since the oral health behaviors were based on a self-reported questionnaire, there could be a response bias, such as social desirability bias. Sixth, our study design could not suggest a causal relationship as a retrospective observational study. However, the strength of this study is that we used a long-tracked, large nationally representative database to elucidate the link between oral health and the occurrence of Meniere’s disease. The results of this study provided evidence that supports the role of better oral hygiene and behavior in the prevention of Meniere’s disease.
In conclusion, oral health management, including frequent tooth brushing and professional dental scaling, are associated with a decreased risk of Meniere’s disease. Poor oral health, such as the presence of periodontitis and the loss of multiple teeth, may increase the incidence of Meniere’s disease.



留言 (0)