1. IntroductionPatients with end stage kidney disease undergoing dialysis are at a high risk of experiencing adverse drug events and other negative outcomes due to polypharmacy and multiple comorbidities [
1]. Dialysis patients have the highest pill burden of all chronically ill patient populations with an estimated daily average of 12 medications [
2]. Consequently, they are at extremely high risk of experiencing drug therapy problems (DTPs), defined as an actual or potential undesirable incident related to medication that affects the goals of therapy [
3]. Integrating pharmacists into the care of hemodialysis patients has been shown to reduce mortality, medication use and length of hospitalizations [
4].The COVID-19 pandemic introduced unprecedented challenges to direct patient care in the ambulatory setting. Telepharmacy gained popularity as a method of supporting pharmacist medication management while maintaining social distancing [
5]. A pre-COVID systematic review of 34 studies demonstrated that clinical pharmacy telemedicine interventions in the outpatient or ambulatory setting, primarily via phone, had an overall positive impact on chronic disease management [
6], a finding corroborated by a systematic review of inpatient intensive care unit (ICU) and non-ICU telepharmacy services published in the same year [
7]. The evidence supporting telepharmacy in the ambulatory care setting has continued to grow since the COVID-19 pandemic, with studies showing benefit of telepharmacy interventions in chronic diseases such as hypertension [
8], diabetes [
9,
10] and in the management of anticoagulation medications [
11]. Unfortunately, there are no published studies of telepharmacy interventions in chronic kidney disease (CKD) or dialysis patients to date. Studies have shown that in-person pharmacist medication reviews in patients with chronic kidney disease (CKD) lead to a reduction of DTPs and improvement in management of chronic diseases, such as anemia, diabetes, hypertension and dyslipidemia [
12,
13]; however, it is unknown if there is a similar benefit with telephone-based medication reviews [
13].
The Home Dialysis Clinic located at the Saint John Regional Hospital (Saint John, NB, Canada) provides care to home dialysis patients (peritoneal dialysis and home hemodialysis) within New Brunswick’s Horizon Health Network. Restrictions arising from the COVID-19 pandemic required a transition from in-person clinic visits to telephone clinic visits for home dialysis patients. Pharmacists therefore had to adapt patient care practices in order to transition from in-person medication reviews to telephone medication reviews.
Based on the positive outcomes seen with telephone-based pharmacy interventions in other chronic disease populations, we hypothesized that similar outcomes would be observed with telephone medication reviews versus in-person medication reviews in home dialysis patients.
The purpose of this study was therefore to evaluate whether differences in quality of care existed between in-person pharmacist medication reviews versus telephone pharmacist medication reviews for home dialysis patients.
4. DiscussionOur study provides evidence suggesting that telephone medication reviews by a pharmacist provide similar quality of care to in-person pharmacist medication reviews in home dialysis patients. Within our study cohort, we found no difference in the number of DTPs identified per patient between in-person and telephone medication reviews. Although the number of pharmacist recommendations did not differ between modalities, physician acceptance of pharmacist recommendations was higher with in-person visits. Patients reported a similar quality of care with telephone medication reviews and found them to be convenient and effective. This study supports existing literature that pharmacists have a positive impact on clinical outcomes and maintain clinical services with telephone-based care, with evidence from individual studies and systematic reviews indicating this positive impact existing across clinical care disciplines and in both outpatient and inpatient settings [
6,
7,
8,
9,
10,
15,
16].
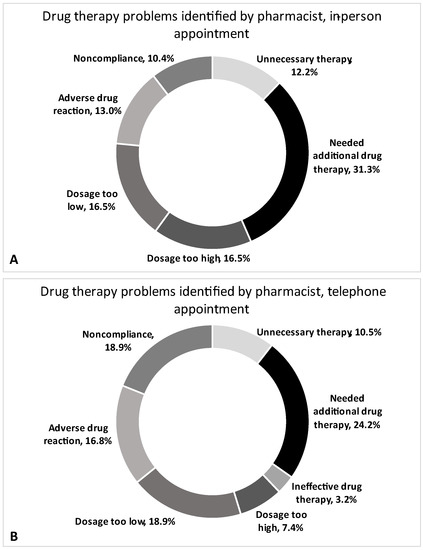
To our knowledge, this is the first study to compare in-person versus telephone medication reviews by a pharmacist in a dialysis population. Pharmacists identified an average of 2.5 DTPs during in-person medication reviews compared to an average of 2.1 DTPs during telephone reviews (p = 0.431). The types of DTPs identified were similar between groups, with the top three categories being “Needed additional therapy” (24.2–31.3%), “Dosage too low” (16.5–18.9%) and “Adverse drug reaction” (13.0–16.8%).
It is important to highlight that the format and depth of the pharmacist telephone medication reviews were similar to in-person reviews. Implementation of telephone medication reviews led to more robust pharmacist documentation as the interdisciplinary team transitioned from paper documentation to electronic documentation of clinic visits. This was necessary to facilitate communication between team members working remotely, including between pharmacists and nephrologists. Pharmacists communicated their recommendations to the nephrologist through documentation in the electronic chart. The nephrologist would read assessments and recommendations from the pharmacist and other care team members (nursing, dietitian) prior to completing a telephone visit with the patient. Although a standard telephone clinic process was developed over the beginning of the pandemic, physician acceptance of pharmacist recommendations was lower with telephone visits versus in person. This was an unexpected finding. Before the pandemic, in-person visits allowed pharmacists more opportunity to discuss recommendations with nephrologists face-to-face and in real time. We hypothesize that the loss of opportunity for in-person discussions following adoption of a virtual clinic model led to a lower physician acceptance of pharmacist recommendations. This is supported by the findings of a retrospective study of acceptance factors for hospital pharmacist interventions [
17]. Pharmacist recommendations were accepted more often when communicated verbally to physicians (either in-person or by phone) rather than by text through a hospital software system (+27.7%, 95% CI: +23.2 to +32.1%) [
17]. Alternatively, in a study by Bruns et al. investigating the control of blood pressure, all recommendations made, regardless of appointment type, were accepted by the care team [
8]. This difference in findings between studies indicates further work should be performed to identify if acceptance of pharmacist recommendations is based on the type of review and recommendation format, the team dynamic, the clinical care area, or the type of pharmacist intervention/recommendation being made. As a telephone model of care becomes standard practice and pandemic operations normalize, future work should also reinvestigate this finding to identify if physician acceptance rates reach parity between telephone visits and in-person. Interestingly, our DTP results differ from prior studies in the general population. A recent retrospective observational cohort study by McNamara et al. of primary care patients found that significantly more DTPs were identified during pharmacist in-person reviews vs. telephone reviews, whereas our study found no difference [
18]. Most patient encounters were unique between treatment groups in the McNamara et al. study [
18]. Only 26 study patients were reviewed by a pharmacist during both an in-person and telephone visit [
18]. In contrast, participants in our study were required to have two in-person medication reviews and two telephone medication reviews to be included. By comparing the same patients between medication review methods, we have mitigated the confounding that may have been introduced by participants themselves. By having some participants present for both visit types and others for only one of the two modalities, confounding may be introduced in studies like McNamara et al. where independence between comparator groups cannot be ensured. This may account for observed differences in DTP findings between our study and theirs. Another possible factor for observed differences may be that McNamara et al. did not follow a standardized process when switching to telehealth given the urgency for change at the beginning of the pandemic [
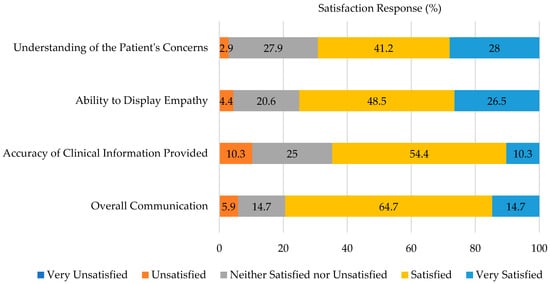
18]. Practices varied from provider to provider and department to department. In contrast, our clinic was able to adopt a standardized telephone clinic process early on due to our smaller program size. It is possible that COVID-19 may have impacted DTPs in our study as patients were less likely to see other health care professionals in-person during the telephone medication review data collection period, however, future work should ultimately look at the long-term drug therapy patient outcomes following the pandemic as this was not a variable of interest for our study. Most patients surveyed in our study were satisfied with pharmacist telephone medication reviews. Patients reported a similar quality of care with telephone medication reviews compared to in-person reviews and found them to be convenient and effective. These findings are supported by a survey of 235 non-dialysis CKD patients from Ontario, Canada, who were converted from in-person to telephone visits with their nephrologist in response to the COVID-19 pandemic [
19]. In our study, patients were very comfortable with telephone consultation and felt their concerns and preferences were addressed equally well compared with in-person visits. Most patients preferred telephone consultation as it reduced waiting periods, travel time and travel costs. Patients who preferred in-person visits felt that telephone consultation limited interpersonal relationship development with their nephrologist.
This study has several limitations. First, chart review and classification of DTPs was completed by one reviewer due to limited resources. Having multiple independent reviewers of DTPs would have provided a more robust dataset. Second, the patient satisfaction survey was not validated as there was no existing survey that adequately addressed the goals of this study. The survey was piloted by a small group of transplant and hemodialysis patients for readability, however there is still a risk of response bias with a non-validated survey. It is also recognized that single-centre, retrospective studies on small regional samples inherently limit our ability to generalize our results broadly to health centres in other jurisdictions within or outside Canada. We therefore recommend future studies assess the use of in-person, telephone, or other virtual modalities for pharmacist medication reviews in CKD patients through multi-centre or randomized controlled trial designs to provide strong evidence towards patient care management decisions. Lastly, the survey was offered over the telephone or online, though most respondents chose to complete the survey over the telephone with the primary investigator reading the questions and completing the survey online for the participants. This increases the risk of observation or acquiescence bias as respondents may have been more likely to agree to statements read by an investigator.
Future work should reassess patient satisfaction to ensure continued acceptance of a telephone-based model of care, especially now that many COVID pandemic restrictions that were in place within healthcare systems during our study have been lifted. Because our study was focused on a pharmacist-led medication review for CKD patients, our main outcomes related to the process measures and the patient satisfaction of such a service. We therefore recommend future work to investigate CKD patient outcomes following in-person or telephone pharmacist-led medication reviews, to provide vital context towards differences in their impact on mortality or morbidity patient outcomes. Patients reported satisfaction with telephone pharmacist care, although not all felt that the telephone could replace in-person visits completely. Future research should focus on quality of pharmacist telephone care and patient outcomes 1–2 years post-pandemic onset to assess whether there are differences in DTPs after care teams are more established in their telephone/virtual care processes.







留言 (0)