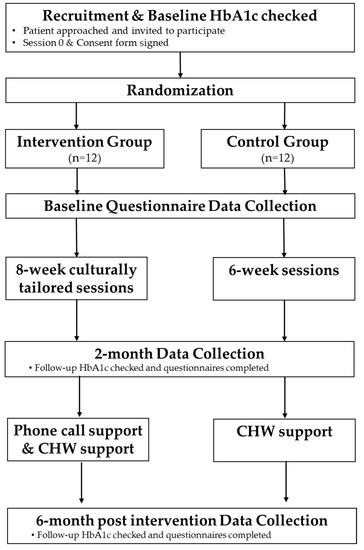
3.1. Search ResultsThe initial search of Medline, Embase, and IPA returned 259 records which were narrowed to 48 following deduplication and applying limitations of English language and excluding review articles. An additional search of the CINAHL initially returned 49 records, with 48 being deemed eligible for further review after limiting to English language. A search of ScienceDirect was conducted which returned 1245 records. Limitations of research articles, medicine and dentistry, pharmacology, toxicology and pharmaceutical science, and nursing and health professions were applied, leaving 336 records eligible for further review. After initial screening 15 potential records remained, 11 of which met eligibility criteria (
Figure 2) and were included in this review. Evaluated studies included seven randomized placebo-controlled trials, one randomized non placebo-controlled trial, one case study, one observational retrospective study, and one quasi-experimental cross-sectional study [
19,
20,
21,
22,
23,
24,
25,
26,
27,
28,
29]. Resultant records included seven randomized placebo-controlled trials, one randomized non placebo-controlled trial, one case study, one observational retrospective study, and one quasi-experimental cross-sectional study that assessed the effect of EPO alone or in combination with other supplements or medications in peripartum persons during parturition [
19,
20,
21,
22,
23,
24,
25,
26,
27,
28,
29]. The type of intervention and control (if used), study design, population, study location, and duration are reported in
Table 1.Dove and Johnson (1999) conducted a single-center, quasi-experimental, superiority study designed to investigate the effects of EP on the length of pregnancy and pregnancy outcomes in low-risk nulliparous peripartum persons [
19]. The study took place from January 1991 to September 1998. Included were individuals who had accurate gestational dating, cephalic presentation, low-risk status, and delivered between 38 and 42 weeks gestation. There were no exclusion criteria listed due to the retrospective nature of this study. The primary outcome was mean time in labor, with results reported in
Table 2. Safety outcomes were not reported in this study. Authors concluded that EPO does not shorten the length of labor or gestation. The case report authored by Wedig et al., (2008) described a healthy, 31-year-old who was given oxytocin and gave birth to a female who was born at 38 weeks and four days gestation weighing 2885 g [
20]. This case report provides relevant safety data, reported in
Table 3. The infant was born after 16 h of labor and had Apgar scores of nine. Diffuse ecchymoses and petechiae appeared on the neonate’s trunk, extremities, and face at 17 h of age. A physical examination was unremarkable except for mild jaundice. She was transferred to the neonatal intensive care unit (NICU) for observation, where platelet count, head ultrasound, and urinalysis were normal. In the NICU, no new ecchymoses were seen and she was discharged at five days of age. The authors concluded that EPO has not been proven safe and effective and should be further studied.Zahran et al., (2009) conducted a double-blind, superiority randomized controlled trial (RCT) which sought to determine whether outpatient administration of EPO was a safe and effective method of labor induction in women with postdate pregnancy [
21]. The study took place at the Women’s Health Centre of Assiut University from January 2008 to July 2009. Patients were included if they had a gestational age of at least 40 weeks, without an urgent indication for labor induction, a singleton living fetus with average amniotic fluid and a non-reactive stress test with Bishop score eight or less. Excluded were those with medical or obstetric indications for termination, fetuses larger than 4000 g, presence of fetal anomalies, intrauterine growth retardation, previous uterine scarring, premature membrane rupture, cephalopelvic disproportion, and presence of any other contraindications to vaginal delivery. The primary outcome was frequency of successful induction, with a secondary outcome measure being a change in Bishop score from admission to labor. Results of the secondary outcome are reported in
Table 2. Regarding the primary outcome, frequency of successful induction defined as birth within 14 days of drug administration, the mean number of days from drug use to birth was 7.4 ± 1.2 and 8.4 ± 1.4 for the EP and placebo groups, respectively. Safety data is reported in
Table 3. Authors of the study concluded that EPO is well tolerated in this patient population with negligible complications, but that it was not beneficial in shortening gestation or improving the Bishop score. Jahdi et al., (2016) conducted a triple-blind, superiority RCT to determine the effectiveness of oral EPO on the ripening and softening of the cervix in nulliparous peripartum persons [
22]. The study was conducted from August to December 2015. Included were healthy, low-risk peripartum persons from Iran with a gestational age of between 40 weeks to 40 weeks and six days, a Bishop score less than 4, a healthy membrane, no drug use, and those who avoided intercourse and did not use enemas, laxatives, or herbals during the study. Exclusion criteria were not listed. The primary outcome was the Bishop score, with results reported in
Table 2. Safety data was not reported in this study. Authors concluded that taking one EPO capsule every twelve hours did not have a statistically significant difference on the Bishop score.Diansuy N et al., (2017) conducted a cross-sectional quasi-experimental study to determine the efficacy of EPO capsules for cervical ripening amid induction of labor [
23]. The study was conducted from May to July of 2016. Inclusion patients were 18 years or older with accurate gestational age, singleton term pregnancy, cephalic presentation, Bishop score of four or less, intact amniotic membranes, biophysical profile of 100%, and those with stable maternal conditions. Excluded were those with contraindications to vaginal delivery due to placenta previa, previous uterine scarring, or an estimated fetal weight greater than or equal to 4000 g. The primary outcome was the Bishop score, with results reported in
Table 2. Safety data was not reported on in this study. Authors concluded that using vaginal EPO in singleton pregnant peripartum persons was promising for cervical ripening, but additional research was warranted.Kalati et al., (2018) conducted a triple-blind, single center, superiority RCT to evaluate the effectiveness of EPO on the duration of pregnancy and labor [
24]. The study was conducted from March 2014 to August 2015. Inclusion criteria were nulliparous Iranian individuals at least 40 weeks gestation with a low-risk singleton pregnancy, cephalic presentation, Bishop score less than 4, BMI between 19–25 kg/m2 and an estimated fetal weight of 2500 to 4000 g. Excluded were those with high risk pregnancies, complications during pregnancy; presence of serious maternal systemic disorders; history of drug use; vaginal bleeding; fetal distress; ruptured membranes; use of other methods for cervical ripening; or development of adverse effects from the study drug. The primary outcome was the Bishop score, with results reported in
Table 2. Safety data is reported in
Table 3. Authors concluded that there is insufficient evidence to support the effectiveness of EPO for cervical ripening.Najafi et al., (2019) conducted a double-blind, single center, superiority RCT designed to determine the impact of vaginal EP capsules on the Bishop score in nulliparous peripartum persons at term [
25]. The study was conducted from November 2017 to May 2018. Patients were included if they were between 18–35 years of age and had a vaginal delivery, at least 38 weeks gestation, nulliparous with an intact amniotic sac, and a singleton fetus with a live and healthy embryo. Excluded were those not using a vaginal EP capsule for two consecutive times, allergic to the capsule, with an indication for urgent medical intervention for maternal or fetal needs, use of enemas, laxatives, or herbal capsules, or patients engaging in intercourse to facilitate delivery. The primary outcome was the change in Bishop score during the stages of labor, with results reported in
Table 2. Safety outcomes are reported in
Table 3. Authors concluded that use of vaginal EP capsules may be an effective, safe, and affordable way to facilitate cervical ripening in nulliparous peripartum persons at full term. Hashemnejad et al., (2019) conducted a triple-blind, single-center, superiority RCT to investigate the effectiveness of vaginal administration of EP in inducing delivery [
26]. The study was conducted during 2019. Inclusion criteria were peripartum persons at 37 weeks gestation in patients who had no previous hospitalizations prior to giving birth, Bishop score less than four, without an indication for emergency delivery. Excluded were who declined to participate in the study for any reason. The primary outcome measures were delivery pain commencement, labor duration, and delivery time. Mean interval between administration and onset of pain were 19.06 and 13.4 h for the EP and control groups, respectively. The mean interval between administration and delivery were 73.83 and 60.68 h, respectively. Safety data was not mentioned in the study. Authors concluded that vaginal administration of EP capsules was not effective in cervix preparation. Authors noted that further research is needed to adequately determine the effects of EPO. Bahmani et al., (2019) conducted a single-blind, single center, superiority RCT to compare the effects of vaginal EPO capsules and vaginal misoprostol on cervical ripening in nulliparous peripartum persons, during post-term pregnancy [
27]. This study was conducted in 2018. Inclusion were healthy, willing, and nulliparous individuals with a single pregnancy, 40 weeks and six days gestational age, with no contraindications to EPO or misoprostol, no structural cervical abnormalities, Bishop score of four or less, and presence of a live fetus. Excluded from the study were those who used enemas, laxatives, or herbal medicines prior to the study, those unwilling to cooperate at any point, need for cesarean section, or the development of adverse effects from the study drug. The primary outcome measure was the Bishop score, with the results reported in
Table 2. Safety data was not mentioned in the study. Authors concluded that use of vaginal EPO with misoprostol was more effective in reducing the Bishop score and improving cervical ripening in this population, compared to the use of misoprostol alone. Mirzadeh et al., (2020) conducted a single-center, single-blind, superiority RCT comparing the effects of vaginal misoprostol tablets with vaginal EP capsules in cervical ripening in nulliparous peripartum persons [
28]. The study was conducted from April to November 2018. Peripartum individuals aged 18–30 years old with a low-risk first pregnancy and a gestational age of 40 weeks to 40 weeks and six days, live cephalic fetus, Bishop score less than four, intact amniotic sac, and estimated fetal weight of 2500 to 4000 g. Excluded from the study were those with a vaginal exam 24 h prior to the study, used other herbal medication, or engagement in sexual intercourse during the study. The primary outcomes were mean Bishop score at admission and comparison of the Bishop score components at admission, with results reported in
Table 2. Cervical dilatation and consistency at time of admission were significantly improved in the EP group (p
Table 3. Authors of this study concluded that vaginal EP capsules could be effective regarding cervical ripening and dilatation. Azad et al. (2022), performed a single-center, double-blind, superiority RCT to assess the effects of EPO on ripening of the cervix in post-term pregnant women [
29]. The study occurred between November 2018 to December 2019. Included in the study were peripartum individuals aged 18–35 years during their first pregnancy with a live singleton baby; gestational age of 41 weeks or greater; cephalic presentation with intact membranes; and a Bishop score of four or less. All cases of major fetal anomaly, fetal growth restriction, fetal distress, uterine anomaly, abnormal vaginal bleeding, or history of uterine surgery were excluded from the study. The primary outcome was the Bishop score, with results reported in
Table 2. Safety data is reported in
Table 3. Authors of this study concluded that vaginally administering a single 1000 mg dose of EPO at 41 weeks gestation significantly improved the Bishop score, as well as reduced post-term parturition time. Authors noted that further studies would help optimize EPO dosing for cervical ripening.







留言 (0)