4.1. Principal Findings
This study aimed to identify factors associated with the prevalence and severity of menstrual-related symptoms. As a result, significant ORs were observed for some of the physical characteristics, menstrual characteristics, and lifestyle factors.
Regarding physical characteristics, age and BMI were significantly associated with the prevalence of PD, and BMI was associated with the severity of PD. PD is known to be more common during the late teens compared to during the early twenties, peaking around age 20 and decreasing thereafter [
138]. Two of the studies included in the present meta-analysis, both of which involved university students in their teens and twenties, revealed that the prevalence of PD decreased with increasing age. This supports the findings of a previous study [
138]. Considering low BMI values, it is known that normal reproductive development and menarche require adequate body fat mass. A previous study reported that a body fat percentage of at least 17% should be maintained for the onset of menarche and at least 22% is required for regular menstruation [
139]. In addition, low available energy, which is associated with low BMI, leads to the disruption of the hypothalamus–pituitary system [
139,
140]. Disorders of the hypothalamus–pituitary system cause amenorrhea and abnormal menstruation by inhibiting the secretion of luteinizing hormone and follicle-stimulating hormone from the pituitary gland and blocking stimulation of the ovaries [
139,
140]. Furthermore, Ju et al. [
141] reported a U-shaped relationship between the body fat percentage and the prevalence of PD; high BMI has been reported to cause early menarche, irregular menstrual cycles, rare menstruation, amenorrhea, and chronic anovulation [
142]. This suggests that, in addition to low BMI, high BMI may also increase the prevalence and severity of PD. Therefore, maintaining an appropriate BMI may reduce the prevalence and severity of PD.Regarding the characteristics of menstruation, the number of menstrual days, menstrual cycle, and family history of PD were significantly associated with the prevalence of PD. PD is known to result from uterine contractions caused by pain-inducing prostaglandins [
143]. Prostaglandins are normally secreted during menstruation to expel the endometrium. However, prostaglandins also cause local vasoconstriction, and excessive prostaglandin secretion causes uterine ischemia and pain, resulting in PD [
143]. In addition, longer menstrual periods increase the duration of prostaglandin secretion, which may lead to longer durations and more severe pain. The disruption of the hypothalamus–pituitary system and the blockage of ovarian stimulation cause discontinuation of estrogen production. When the production of estrogen is disrupted, the balance of female hormones is disturbed, resulting in an irregular menstrual cycle [
139,
144]. Pertaining to family history of PD, Jahanfar et al. [
105] examined the genetic factors in menstruation-related problems in monozygotic and dizygotic twins and reported that 40−50% were related to genetic factors. It may also be relevant that approximately 56% of information sources regarding girls’ pain management and menstruation are mothers [
145].For lifestyle factors, stress, sleep duration, and sleeping time were significantly associated with the prevalence of PD. Smoking was also associated with the prevalence of PMS. Female reproductive organs are believed to be highly sensitive to stress, and intense stress could have detrimental effects on health [
40,
146]. Activation of the corticotropin-releasing hormone system by elevated stress levels inhibits the release of follicle-stimulating hormone and luteinizing hormone, thereby inhibiting follicle development [
40,
146]. Stress-related hormones such as adrenaline and cortisol can also increase prostaglandin synthesis and cause PD [
146]. Additionally, short sleep duration was suggested to lead to a decrease in melatonin secretion [
147]. Regarding the effects of melatonin on sexual function, a pituitary−gonadal function is reduced during winter, when melatonin secretion is lower [
148], and melatonin administration to neonates causes sexual prematurity [
149,
150]. Therefore, melatonin secretion may affect reproductive function. In contrast, the occurrence of PD itself was reported to reduce sleep duration; therefore, a causal relationship is unclear [
20].
The present study revealed no significant ORs for physical activity, alcohol consumption, caffeine intake, and breakfast skipping.
Physical activity promotes the release of endorphins in the blood that reduces pain, exerts a relaxing effect on muscle [
151], reduces cortisol levels, and reduces the synthesis of prostaglandins that cause pain [
152]. For these reasons, physical activity has been shown to be effective in improving PD, suggesting an association between physical activity and PD [
151]. However, no association was identified in the present study. The reason could be attributed to differences in exercise intensity. The results of the present study by age group indicated that more studies involving teenagers and participants in the twenties suggested an association with PD and PMS than studies targeting those aged ≥30 years. This may be attributed to the fact that the definition of exercise differed according to the age group. Especially, studies of women in their teens and twenties defined high-intensity exercise, such as performing sports club activities, while studies of women in their thirties and older defined and included low-intensity exercises, such as walking. In a previous study that examined factors associated with the prevalence of PD in female athletes and non-athletes, only non-athletes showed an association between exercise and the prevalence of PD, and the reason for this association might have been exercise intensity [
153]. Therefore, exercise intensity should be considered when examining the association between physical activity or exercise and prevalence and severity of PD and PMS. For alcohol and caffeine intake, over-contraction of the uterus has been shown to decrease blood flow in the uterus and cause pain [
154,
155]. Caffeine has been demonstrated to increase uterine contractions [
156], and alcohol consumption reduces uterine arterial blood flow by approximately 40% [
157]. However, no significant ORs were identified in the meta-analysis of the present study. This difference could be attributed to varying definitions of alcohol and caffeine consumption. Specifically, among the studies included in the present meta-analysis, the criterion of a study [
6] of Chinese university students was one glass of wine per month in the past 6 months (approximately 250 mL), whereas the criterion for having alcohol consumption in a study including Turkish university student was ≥1 drink/week [
56]. Regarding caffeine intake, one criterion was ≥300 mg of caffeinated soft drinks, coffee, decaf coffee, black tea, chocolate milk, and chocolate bars in a study involving Iranian university students [
5], whereas in another study involving Chinese university students, the criterion was the consumption of three or more caffeine-containing substances, such as coffee, tea, and chocolate in the past month [
6]. These differences in definitions may have led to the conflicting results.Skipping breakfast also leads to a lower intake of certain foods, and it is suggested that nutritional imbalances may lead to PD [
20]. In addition, dairy products and dietary fiber, which are commonly consumed at breakfast, show a significant association with PD, and a lower intake of these nutrients may increase the risk of PD [
84,
158,
159]. Additionally, it was noted that missing breakfast may interfere with diurnal rhythms and negatively affect reproductive function [
159], and there may be a link between eating habits and the development of PD and PMS. However, no significant ORs were identified in the present meta-analysis. The first reason for this discrepancy could be the effect of cultural background. Three studies were included in the meta-analysis regarding skipping breakfast: one study of Iranian university students [
5], another of Chinese university students [
6], and the other of Japanese junior high school students [
20]. These cultural differences may be related to the lack of association. Second, each study had a different definition of skipping breakfast. The study of Iranian university students defined skipping breakfast as having breakfast ≤ 1 time per week, whereas the definition in the study involving Chinese university students was not eating breakfast more than once in the past week; the definition used in the study of Japanese junior high school students was occasional or no breakfast intake. Therefore, in the future, consideration of the cultural background with the associated definition of skipping breakfast is necessary to assess the association of each item with the occurrence and severity of symptoms associated with menstruation. 4.2. Strengths and LimitationsMany studies have investigated the factors associated with menstrual symptoms in the past few decades. Most of them focus on dysmenorrhea occurring during menstruation [
5,
6,
10,
20,
28,
34,
38,
58,
66,
68,
83] or premenstrual syndrome occurring before menstruation [
32,
43,
70]. However, many women experience symptoms associated with menstruation both before and during menstruation, rather than only before or during menstruation. Moreover, the discrimination between premenstrual and menstrual symptoms was suggested to be meaningless because the types of symptoms were similar [
160]. Furthermore, several factors were associated with the development of menstrual symptoms, and the degree of influence of these factors should be clarified. Therefore, the present systematic review and meta-analysis tried to synthesize the findings of previous publications on pre-menstrual syndromes, which occurs before menstruation, and dysmenorrhea, which occurs during menstruation. To our knowledge, our study is the first to identify factors associated with the prevalence and severity of these symptoms. Nevertheless, this study has several limitations. First, many of the symptoms associated with menstruation are self-reported and may include conditions such as organic dysmenorrhea. Of the 34 studies [
5,
6,
9,
10,
12,
20,
22,
23,
24,
28,
29,
30,
32,
34,
35,
37,
38,
41,
43,
49,
55,
58,
59,
60,
61,
65,
66,
68,
69,
70,
72,
75,
80,
83] from which meta-analysis data could be extracted for this study, 21 studies [
5,
6,
9,
12,
20,
29,
30,
32,
34,
37,
38,
43,
58,
59,
66,
68,
70,
72,
75,
80,
83] used a self-response questionnaire, and PD and PMS were assessed by the participant, without being examined by a physician. Second, causality of the factors associated with menstrual symptoms is unclear. Many of the studies accepted for inclusion in the systematic review of this study were cross-sectional studies and did not examine causality. For case-control studies [
10,
22,
23,
24,
28,
33,
35,
41,
49,
55,
60,
61,
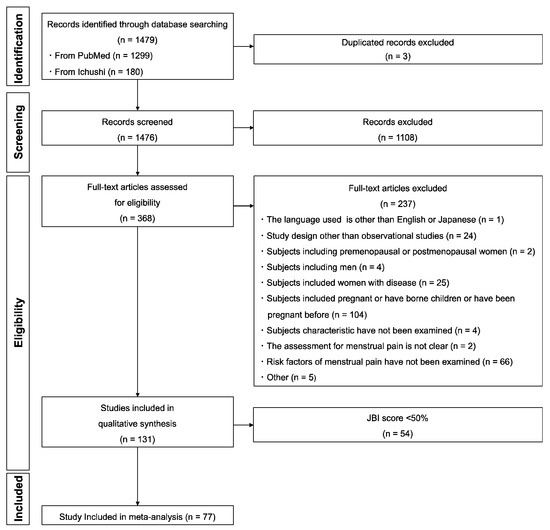
65], only cross-sectional data at the start of the study were extracted. Third, racial and ethnic differences are not considered. The study participants of the included studies in the present systematic review were predominantly from the United States and Turkey. Finally, only 34 of the 77 studies were included in the meta-analysis because we could extract comparable data for the meta-analysis concerning three topics: physical characteristics, menstrual characteristics, and lifestyle. Each analysis had a small number of studies. Therefore, generalizability of the present study is limited.

留言 (0)