1. IntroductionPeriampullary tumors arise within 2 cm of the ampulla of the duodenum and include ampullary tumors, pancreatic head cancer, lower common bile duct cancer, ampullary cancer, and periampullary duodenal cancer [
1]. Periampullary neuroendocrine neoplasms (NENs) are extremely rare tumors, accounting for less than 1% of all gastrointestinal neuroendocrine tumors and less than 2% of all tumors of the ampullary region [
2]. Periampullary NENs are heterogeneous tumors that originate from the neuroendocrine cells of the gastrointestinal tract or pancreas [
3,
4]. According to the updated World Health Organization (WHO) classification, NENs include low-grade neuroendocrine tumors (NETs) and high-grade neuroendocrine carcinomas (NECs) [
5]. The prevalence of periampullary NENs has been consistently increasing, which may be attributable to improvements in the way NENs are diagnosed, including better imaging tests and endoscopy, and increased awareness of these tumors [
3,
6].The complexity of the periampullary anatomy makes it difficult to determine the origin of these tumors [
7]. Fortunately, advances in techniques have helped with diagnosis as well as with defining the extent of the lesion and potential resectability. For periampullary tumors, surgery is the recommended treatment, and pancreaticoduodenectomy (PD) is the classic procedure. Endoscopic removal is being extended to different lesions with encouraging preliminary results [
8,
9]. At present, there are very few studies on periampullary NENs. A retrospective study of 101 patients with ampullary and duodenal NETs demonstrated lymph nodal involvement to be common among those >1 cm in size, and resection with lymphadenectomy for these larger tumors is recommended [
10]. Another National Cancer Database (NCDB)-based study compared patients with ampullary, duodenal, or pancreatic head NETs; this study was, however, limited by unknown data [
11]. Nevertheless, there is no individual prediction model to evaluate the prognosis of patients with periampullary NENs. The American Joint Committee on Cancer (AJCC) staging system is the most frequently used system to evaluate prognosis in patients with NENs. It can be inferred from research on NETs involving other sites that the major limitations of the AJCC stage include low accuracy, disregard of other factors, and poor performance in predicting individual survival risk [
12,
13].
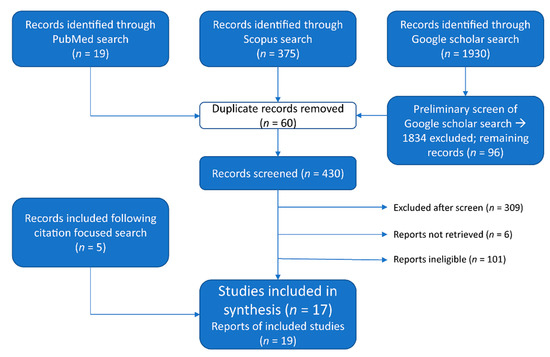
Given the rarity of periampullary NENs, and in particular NENs of the ampulla, there is a clear gap in knowledge in the current literature, which is limited to primarily small case series. In the present study, using the dataset from the Surveillance, Epidemiology and End Results (SEER) database, we aimed to identify prognostic factors for patients with periampullary NENs, and then to develop and validate nomogram prognostic models to visually predict the overall survival (OS) and cancer-specific survival (CSS) in patients with periampullary NENs.
4. Discussions
Periampullary NENs are relatively rare tumors, with little clinical evidence regarding prognosis. This study constructed and validated prognostic nomogram models for both the OS and CSS of periampullary NENs based on the public database SEER. By both internal and external validation, the nomograms used displayed comparable outcomes to those of the TNM stage and SEER stage. Seven variables were selected by Cox regression and incorporated into the nomogram. Measured by standard deviation along with nomogram scales, the degree of differentiation and surgery were the most important factors, with the remaining factors being age, tumor size, pathological type, N stage, and M stage. This was the first study to establish prognostic models for patients with periampullary NENs. The prognostic nomograms could facilitate clinical prognostic evaluation and personalized treatment.
In predicting prognosis, we treated the NENs at all three sites as a whole. Whether or not the site of tumor origin (ampullary, duodenum, or pancreatic head) determines the prognosis has always been a concern. Previous reports have suggested that tumors arising at the ampulla of Vater are associated with a larger size, higher grade, and increased risk of nodal metastases [
15,
16]. Both prior single-institution case series [
17] and our findings show a higher rate of lymph node metastasis in ampullary NENs at diagnosis (ampullary vs. duodenum vs. pancreatic head: 54.4% vs. 15.0% vs. 37.0%, respectively, p
18]. In agreement with Schmocker RK et al., we also found no significant difference for the prognosis of NENs at different primary sites, which indicates that the tissue of origin does not appear to impact long-term outcomes. Other researchers have suggested the same [
15,
18]. Another possible reason is that a large part of the data in the SEER database has been lost, resulting in a smaller number of cases of NENs at the ampulla of Vater. Moreover, neuroendocrine tumors, especially pancreatic NENs, are difficult to detect in the early stages due to insidious onset, and are detected in most patients at an advanced stage (patients in stage IV: duodenum 3.7% vs. pancreatic head 22.9%, pWhile most subtypes are afforded independent staging systems in the latest AJCC staging system, ampullary and duodenal NENs remain combined into one group. This is in part due to anatomic proximity, and determination of the true tissue of origin at this location can be challenging. Although the head of the pancreas is a part of the pancreas, it is also close to the ampulla and the distal bile duct, and the clinical symptoms, surgical methods, and prognosis are similar to those for the duodenum and ampulla. A series of studies has shown that, although the biological behaviors of the three sites are different, this did not affect patient survival [
18], which is consistent with the results of study. Therefore, we undertook to evaluate their roles as independent prognostic factors and to build a prognostic model to predict survival by combining the three factors.Our results show that only the N stage and M stage have predictive effects on patient prognosis, whereas the T stage has no significant effect on the CSS or OS of patients. Distant metastasis measured by M stage is a recognized risk factor [
11,
15], while T stage and N stage have always had conflicting results. T stage is based on tumor size and depth of invasion. Tumor size has been regarded as a prognostic marker for adenocarcinoma of the periampullary region [
10], and a series of studies has proven that tumor size is closely related to lymph node metastasis and prognosis in gastrointestinal NENs [
19,
20]. For d-NENs, tumor size is an important factor in determining the surgical approach [
21,
22,
23]. However, studies have shown differing results. Although current studies on periampullary NENs are very limited, several small, retrospective studies have also found tumor size not to be associated with tumor recurrence and survival [
4,
15]. Whether the depth of tumor invasion is an independent prognostic factor is currently uncertain. According to the N stage, some have suggested that the presence of lymph node involvement contributes to a worse prognosis [
24], while numerous others have shown that lymph node metastases do not appear to impact survival [
10,
16,
21]. These are topics that clearly require additional study. To a certain extent, this suggests that the TNM stage may not be the most accurate tool for prognostic prediction and that the prognosis for patients at the same stage may be heterogeneous. Therefore, we urgently need to establish a prediction model to predict prognosis more accurately for patients with periampullary NENs.The choice of surgical procedure has also been considered a possible reason for the same prognosis in patients despite different tissues of origin. In our cohort, patients with a-NENs and p-NENs were more likely to choose radical surgery, while patients with d-NENs were more inclined to choose local or endoscopic excision. However, previous studies have found a high rate of lymph node metastasis in d-NENs; even given a tumor ≤ 1 cm, there is still a 40% incidence of lymph node metastasis (LNM) [
10]. Studies regarding endoscopic or surgical therapy for ampullary tumors are heterogeneous. There is still no definitive criterion for the choice of endoscopic or surgical resection. Gay-Chevallier S et al. [
25] suggested that a less invasive therapeutic strategy appeared more suitable than oncological surgery for nonmetastatic d-NENs. A small-scale comparative study conducted by Lee SW and his colleagues found that the pathologic complete response rate of lesions ≥ 11 mm in the surgical treatment group was higher than that in the endoscopic treatment group [
26]. In addition, surgical treatment was mostly beneficial among patients with p-NENs > 2 cm, a Ki-67 index ≥ 3%, and lesions located at the pancreatic head, as identification of the LNM was most common among individuals with these tumor characteristics [
27]. In contrast, data on surgical ampullectomies are very few, whether adenocarcinoma or NENs are present [
28]. Research by Beger HG et al. [
29] showed extended resection for low-risk periampullary cancer to be associated with a significant increase in procedure-related biliary and duodenal complications. In summary, the therapeutic value of radical resection remains controversial among patients undergoing surgery for periampullary NENs, despite the possibility that removal of the LNM may decrease locoregional recurrence. Additionally, consensus guidelines and national and international recommendations are lacking. Our nomograms show that, compared with radical resection, the corresponding score of local excision was lower and the survival rate was better. LNE also did not confer survival benefits to patients. The possible reason for this is that radical resection increases the occurrence of postoperative complications. The optimal surgical approach requires further exploration and has implications for individual treatment.In addition, other factors, including age, tumor differentiation, and histology, were associated with recurrence and/or survival [
11,
30,
31,
32]. The current study proved that tumor differentiation and histology were important prognostic factors for CSS and OS. Older age was significantly related to worse survival. Similar to our results, a previous study found that patients with NETs were younger than those with NECs [
33].There are several limitations to the present study. First, as a retrospective study, there exist inherent biases. The large percentage of missing data might have introduced some selection bias. Second, some important variables, such as the Ki-67 index and mitotic index, were unable to be obtained from the SEER database. The Ki-67 index and mitotic index could be used to access the aggressiveness of NETs, which have been endorsed by the European Neuroendocrine Tumor Society (ENETS) grading system [
5,
34]. Third, postoperative complications cannot be assessed in the SEER database. Large prospective studies should be conducted to verify our nomograms in future. Despite these limitations, our prognostic nomograms are important and effective models for providing an accurate and individualized survival prediction in patients with periampullary NENs.








留言 (0)