2. Methods 2.1. Study Design and Setting
A retrospective cohort study was conducted at BC Cancer Vancouver Centre . Tumor molecular data and clinical variables were collected from May 2020 to June 2021. This study, #H18-03295-A009, was approved by the BC Cancer Institutional Research Ethics Board.
2.2. Participants and Data SourcesA retrospective analysis was conducted using prospectively collected demographic and tumor molecular data for NSCLC patients from the BC Cancer Genomic Lab dataset whose tumor tissue was subject to NGS during the 12-month study period (18 May 2020–1 June 2021). All patients had late stage or recurrent NSCLC (based on the American Joint Commission on Cancer [AJCC] Staging 8th Edition) [
27], and as such, they were eligible for molecular testing through the BC Cancer CGL via the standard of care. Patients with squamous NSCLC were eligible for NGS only if they were never-smokers. Additional variables retrieved retrospectively from the medical record included: smoking status (never, former, or current) and immunohistochemistry for PD-L1 (reported as 50%). 2.3. Primary Outcomes
Patients with clinically actionable NSCLC genetic alterations were identified. Actionable driver mutations were defined as those with targeted therapies available in North America. EGFR mutations were interpreted as common sensitizing mutations (EGFR Exon 19 deletion and EGFR L858R), uncommon sensitizing mutations (E709X, G719X, S768I, L861Q, and EGFR co-mutations of the latter), and uncommon non-sensitizing mutations (exon 20 insertion, Denovo T970M). Health authority was determined geographically with tabulation of the participants’ residential postal codes. Time to treatment was defined as the time from the date of the diagnostic procedure to the date of first NSCLC treatment.
2.4. Targeted NGS Panels for NSCLC Genetic AlterationsThe DNA-based hybrid-capture multiplex NGS assay (“OncoPanel”,BC Cancer Vancouver Centre) from the Cancer Genetics and Genomic Laboratory (CGL) at BC Cancer Vancouver Centre was utilized for the cohort. Details regarding the CGK OncoPanel and gene targets are available at
http://cancergeneticslab.ca/genes/oncopanel/ and in the
supplementary data section. In brief, genomic DNA was extracted using an automated system (Promega Maxwell) followed by FFPE repair, ligation-based library construction, PCR amplification, hybridization capture, and sequencing on a HiSeq2500 platform (Illumina, San Diego, USA). Single-strand consensus sequences were generated from UMI-indexed reads using fgbio and aligned with the GRCh37 human genome reference using BWA. Variant calling of DNA mutations and insertions/deletions (INDELs) was performed using samtools and VarScan2. Annotation and filtering of variants was performed using Agilent’s Alissa Interpret platform. For gene fusions, immunohistochemistry (IHC) was employed to determine the aberrant protein expression of ALK, RET, and ROS1 status from matched FFPE slides. 2.5. Statistical Methods
Continuous variables were summarized using means and standard deviations and analyzed using the Student’s t-test. Categorical variables were expressed as frequencies and percentages and compared using the Chi-square or Fisher’s exact tests if appropriate. Single-factor and multi-factor analyses in relation to outcomes (EGFR, for example) required the use of logistic regression. Variables identified to include in the model based on the literature search included female sex and smoking status as these have known associations with sensitizing EGFRm+ expression18. Missing data were not imputed, and out of province records were treated as missing data.
A Cox-Proportional Hazard analysis was performed to assess the differences in time-to-treatment among the health authorities. The model was adjusted for age, sex, type of treatment, and stage at presentation. The conventional level of statistical significance (p < 0.05) was used throughout the study as an indicator of a potential effect. All tests were two-sided. Statistical analyses were performed with Stata17 (StataCorp. 2021. Stata Statistical Software: Release 17. College Station, TX: StataCorp LLC.) and R (R Core Team 2020, R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria).
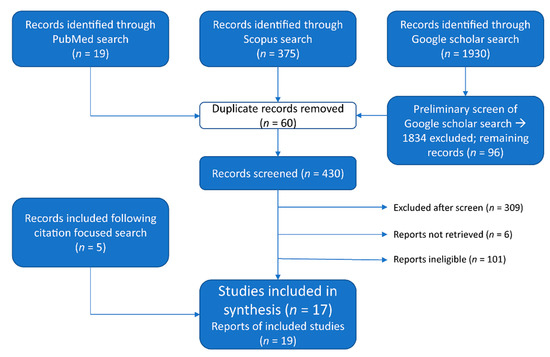
3. ResultsA total of 593 NSCLC patients met eligibility criteria, of which 333 (56.2%) were female, with a median age of 72 (65, 78). VCHA (143, 24.1%) and FHA (213, 35.9%) harbored the majority of study participants as depicted in
Figure 1. There were 11 (1.9%) out of province records excluded from the comparative analysis. A molecular alteration was detected in tumor tissue in 540 (92.8%) of the 582 patients who underwent analysis. A clinically actionable moleculat alteration was identified in 264 (45.4%) of the patients.Adenocarcinoma was the most common NSCLC subtype (482, 82.8%). Of the 582 study participants, 257 (44.2%) were found to have clinically actionable molecular alterations with testing, and 185 (32%) presented with late stage metastatic disease. Demographics and NSCLC tumor characteristics are summarized in
Table 1. There was a significantly higher proportion of never and former smokers in the VCHA and FHA (pp = 0.03). All other characteristics noted were reasonably balanced between HAs, including PD-L1.A summary of the incidence of actionable molecular alterations identified using oncopanel and IHC during the study period are summarized in
Table 2. Any EGFR mutation was detected in 105 patients, and KRAS G12C mutations were identified in 108 (18.6%) individuals. A patient’s tumor expressed multiple mutations in several instances; in particular, co-mutations were observed in the uncommon sensitizing EGFR mutations. EGFR and KRAS mutations were mutually exclusive. ALK fusions detected by IHC were noted to co-occur with KRAS mutations in our cohort.
Univariate analyses showed that there was a significantly higher proportion of common sensitizing EGFR mutations (EGFR exon 19 deletion and EGFR L858R, for example) identified in VCHA and FHA compared to other health authorities (p < 0.001). There was no appreciable difference in the proportion of uncommon sensitizing and uncommon non-sensitizing EGFR mutations among the HAs. As anticipated, counts for these uncommon EGFR mutations in the cohort were low overall. A persistent strong association with these HAs remained when the multivariable analysis adjusted for the association of sensitizing EGFR mutations with the female sex (OR 0.65; 95% CI 0.54, 0.80; p < 0.001). However, after adjusting for never smoker status, the observed association between the higher proportion of sensitizing EGFR mutations in VCHA and FHA was weakened (OR 0.75; 95% CI 0.62, 0.92; p = 0.005).
There was an overall difference in KRAS mutation incidences observed between health authorities on univariable analysis. There was no significant difference observed following multivariable analysis and adjusting for smoker status on KRAS incidence by health authority (OR 1.1; 95% CI 0.97, 1.3; p = 0.14).
There were otherwise no appreciable differences in incidences of MET exon 14 skip, ERRB2 (HER2), and BRAF V600E mutations or fusion profiles among HAs, although counts for these mutations in the study cohort were low.
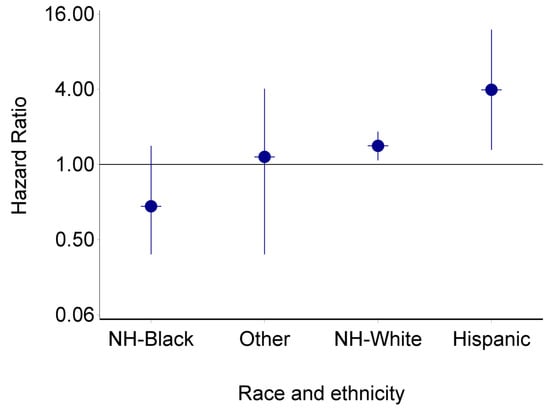
The Cox Proportional Hazard analysis suggests that NSCLC patients residing in regions within IHA (HR 0.60; 95% CI 0.38, 0.95), NHA (HR 0.45; 95% CI 0.21–0.96), and isHA (HR 0.57; 95% CI 0.35, 0.93), experience greater treatment wait times than that of VCHA and FHA when adjusting for sex, age, treatment type, and stage at presentation. There was no significant difference between wait times in VCHA and FHA (HR 0.77; 95% CI 0.52,1.12).
4. DiscussionNSCLC mutations govern the disease’s associated survival and response to treatment, including mutation-targeted and immune-therapy [
28]. Apart from its subtype, NSCLC’s driving mutation(s) are argued to be the most clinically significant disease characteristic. This is particularly true for EGFR mutations given recent advances in the development of its targeted therapies. The favourable outcomes reported for both late stage and early stage cancer from tyrosine kinase inhibitors (TKIs) targeted for EGFR mutated NSCLC highlight the importance of summarizing the frequency of such mutations among populations [
4]. Although an individual patients’ journey with targeted therapy may begin with an oncology specialist referral to the Cancer Genomics and Genetics labs, knowledge translation and resource allocation is managed by regional health authority systems which rely on population data and mapping. To our knowledge, this is the first study to describe the molecular epidemiology of clinically actionable molecular alterations with HA subgroup analyses for the province of BC. In May 2022, BC Cancer launched Canada’s first province-wide lung cancer screening program, providing access to eligible individuals at 36 provincial sites [
29]. Typically, a higher rate of early-stage disease is often captured when screening programs are initiated, which allows for curative intent therapy. In the context of the promising results of adjuvant and neoadjuvant TKIs use for improving overall and disease-free survival, early detection of lung cancer is likely to provide additional survival benefits in the contemporary management of lung cancer. This study provides a mapping of EGFR mutation frequencies among BC’s health authorities, and it may subsequently aid to allot physician education and patient resources accordingly to maximize the quality of provincial NSCLC care.This retrospective review of NSCLC genomics data from the BC Cancer Genomic Lab Oncopanel Dataset summarizes the frequency of actionable driver mutations (EGFR, KRAS G12C, MET Exon 14 skip, ALK fusion, and ROS1 fusion), PDL-1 expression, and treatment wait times among five health authorities. EGFR mutations were present in 106 (17.9%) participants, which is similar to proportions described in contemporary literature. The incidence of EGFR mutations in NSCLC has been shown to vary among ethnicities, occurring at a rate of 15–20% in North Americans [
25,
30,
31], 5–12% in Europeans [
32,
33], 19% in African Americans [
34], and 26–51% among Asian populations, such as those with Chinese, Korean, or Japanese backgrounds [
35,
36,
37]. Common EGFR mutations, defined as exon 19 deletion and exon 21 codon 858 point mutation (L858R), were present in 80.8% of the patients with EGFR mutations, which aligns with rates described among other groups [
32,
38]. Significantly higher proportions of all EGFR mutations were identified in VCHA and FHA compared to other health authorities, which may be driven by differences in never smoker status population demographics across the province. Asian ethnicity is associated with a greater likelihood of having EGFR mutations NSCLC [
39]; hence, regions with increased Asian population densities are expected to harbor greater proportions of EGFR mutations. As per Canada’s most recent Census Profile (2016) [
40], 86% of British Columbia’s Asian population lives in the Vancouver census metropolitan area, legitimizing the observed difference in EGFR mutation frequencies among health authorities.Another notable observation in this study is the limited number of patients represented from BC’s Northern Health Authority. As noted above, the BC Cancer CGL dataset for the study period represents lung cancer patients who were referred for centralized NGS molecular testing following a diagnosis of metastatic or recurrent lung cancer. The small number of NHA NSCLC patients available in the dataset (31, 5%) raises the question of whether NSCLC molecular testing referral patterns are similar across health authorities and whether certain regions face disproportionate referral challenges. Despite accounting for the smaller population in NHA, its representation in the dataset is still less than expected based on regional population matching [
41]. While the scope of this study does not specifically address issues relating to referral pathways, it highlights the necessity to investigate potential disparities between health authorities as it may have implications for NSCLC patients harboring actionable driver mutations who would otherwise be eligible for life-extending therapies.Local health authorities are also responsible for appropriate treatment wait times and must allocate resources to ensure equitable cancer care throughout the province. Delayed access to therapy following diagnosis, adjusting for stage at presentation, is associated with worse overall survival [
42]. The timeliness of care for patients with lung cancer has been addressed by cancer societies across the globe. The acceptable time interval of 30–52 days from diagnosis to first treatment has been acknowledged by the British Thoracic Society [
43], UK National Health Service [
44,
45,
46], Rand Corporation [
47,
48], American College of Chest Physicians [
49], and Cancer Care Ontario [
50]. The median time to treatment, defined as the time from diagnostic procedure (CT-guided biopsy, endobronchial biopsy, pleural fluid cytology, or imaging) to first treatment (surgery, oral targeted therapy, radiation, or chemotherapy) in this study was 39 days (IQR 27, 63) across BC (
Table 3). A British Columbian retrospective study by Van de Vosse et al. reviewed wait times of lung cancer patients from southern IHA in 2010–2011. They reported a median time from biopsy to first treatment of 26 days [
51] which varies from our observed median wait time of 55 days in IHA. This difference can be explained by the geographic limitations of Van de Vosse’s study population as they only included patients from a sub-region of IHA who are closer to major thoracic oncology centers south of the region, such as Kelowna General Hospital and its cancer agency.The COX proportional hazard time-to-event analysis revealed increased wait times for NSCLC patients residing outside of FHA and VCHA regions. This may be explained by the population density of these regions and their proximity to centralized oncology care, including thoracic surgical services. NSCLC patients residing in IHA and NHA experienced the greatest wait times, with median wait times of 55 and 64 days, respectively. This study was not designed to elicit potential causes of differences in wait times, yet this is an important finding that warrants further investigation. Diagnostic and therapeutic timelines are lengthy, multidisciplinary, and complex, which creates many points at which care may be delayed. Therefore, system-wide changes are often required to address suboptimal wait times. The introduction of allied health programs, including lung cancer “nurse navigators” and the development of lung nodule rapid assessment programs, have been demonstrated to reduce surgical and medical treatment wait times for lung cancer patients [
52]. HAs may consider introducing care navigators to support patients and clinicians through the lung cancer diagnostic work-up and treatment journey.
This study is not without limitations. The analysis is retrospective in nature which subjects it to inherit bias, despite the prospective nature of molecular data acquisition. The sample size was limited by the number of patients referred for molecular testing at the CGL. A greater number of NSCLC patients will have data regarding their cancer’s genomic details as EGFR TKIs become more widely accepted for adjuvant and potentially neoadjuvant therapy, which will also enable greater sample sizes and confidence in results. Regarding the adjusted time-to-treatment analysis, certain variables could not be captured or controlled for, including system factors and delays in treatment due to patient hesitation or indecision. Furthermore, a proportion of the study cohort data was collected during the early stages of the COVID-19 pandemic which may have impacted patient treatment choice and potential delays in treatment.








留言 (0)