Rehospitalization Events After Aortic Valve Replacement: Insights From the PARTNER Trial
Background:
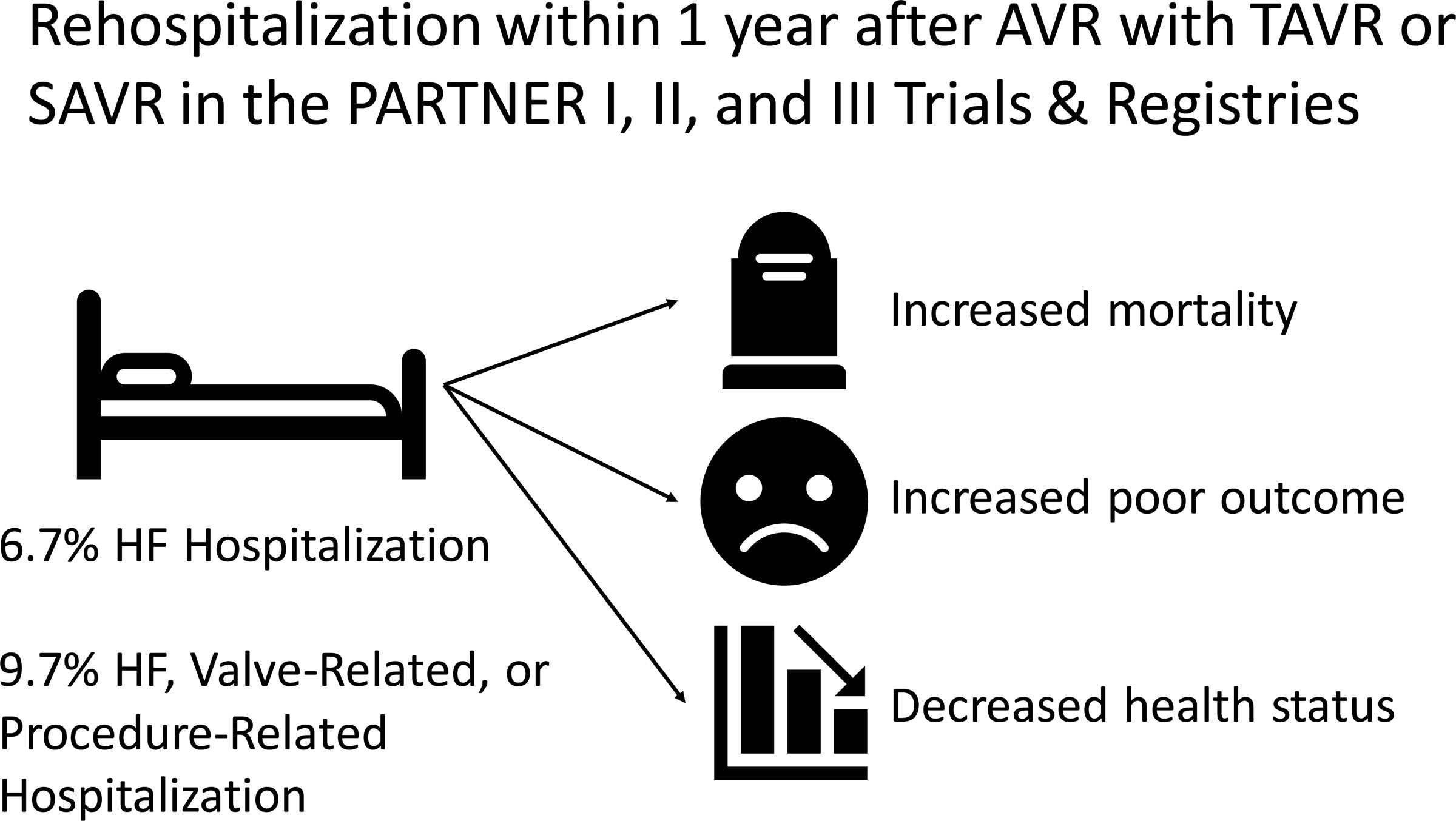
Rehospitalization is a common end point in clinical trials of structural heart interventions, but whether rehospitalization is clinically and prognostically relevant in these patients is uncertain. The aim of this study was to evaluate the risk of rehospitalization events after aortic valve replacement (AVR) and their association with mortality and health status.
Methods:
The study population included patients who underwent transcatheter or surgical AVR in the PARTNER I‚ II‚ and III trials (Placement of Aortic Transcatheter Valves). Health status was assessed with the Kansas City Cardiomyopathy Questionnaire-overall summary score. The primary analysis focused on heart failure hospitalization within 1 year after AVR and its association with mortality, poor outcome (death, Kansas City Cardiomyopathy Questionnaire-overall summary score <60 or decrease by ≥10), and health status at 1 year using adjusted models. Secondary analyses examined the prognostic associations of rehospitalization due to a composite of heart failure, valve-related, or procedure-related causes.
Results:
Among 3403 patients treated with AVR (2008 transcatheter AVR, 1395 surgical AVR), the 1-year incidence was 6.7% for heart failure hospitalization and 9.7% for rehospitalization due to a composite of heart failure, valve-related, or procedure-related causes. Heart failure hospitalization after AVR was associated with increased risk of 1-year mortality (hazard ratio, 3.97 [2.48 to 6.36]; P<0.001), poor outcome (OR, 2.76 [1.73 to 4.40]; P<0.001), and worse health status (Kansas City Cardiomyopathy Questionnaire-overall summary mean difference −9.8 points [−13.8 to −5.8]; P<0.001). Rehospitalization due to a composite of heart failure, valve-related, or procedure-related causes was similarly associated with increased 1-year mortality (hazard ratio, 4.64 [3.11 to 6.92]; P<0.001), poor outcome (OR, 2.06 [1.38 to 3.07]; P=0.0004), and worse health status (Kansas City Cardiomyopathy Questionnaire-overall summary mean difference −8.8 points [−11.8 to −5.7]; P<0.001). There was no effect modification by treatment type (transcatheter AVR versus surgical AVR) for these associations.
Conclusions:
Heart failure hospitalization and rehospitalization after AVR are associated with increased risk of mortality and worse 1-year health status. These findings confirm the clinical and prognostic relevance of rehospitalization end points for trials of AVR.
Registration:
URL: https://www.clinicaltrials.gov; Unique identifier: NCT00530894.

留言 (0)