Title and abstract1(a) Indicate the study’s design with a commonly used term in the title or the abstract1A population-based retrospective cohort study(b) Provide in the abstract an informative and balanced summary of what was done and what was found1
Introduction Background/rationale2Explain the scientific background and rationale for the investigation being reported1-2 Objectives3State specific objectives, including any prespecified hypotheses2We conducted a detailed, population-based analysis to better understand the variability in LC outcomes across Ontario and define patient, disease, and system factors that contribute to regional differences
Methods Study design4Present key elements of study design early in the paper2–32. Study Design and MethodsSetting5Describe the setting, locations, and relevant dates, including periods of recruitment, exposure, follow-up, and data collection3new diagnosis of LC between January 1st, 2007 and December 31st, 2017
Maximum follow-up date was December 31st, 2019, at death, or end of OHIP eligibilityParticipants6(a) Cohort study—Give the eligibility criteria, and the sources and methods of selection of participants. Describe methods of follow-up
Case-control study—Give the eligibility criteria, and the sources and methods of case ascertainment and control selection. Give the rationale for the choice of cases and controls
Cross-sectional study—Give the eligibility criteria, and the sources and methods of selection of participants2–3
Table 1,
Figure 12.1. Case Definitions, Demographics and Study Outcomes(b) Cohort study—For matched studies, give matching criteria and number of exposed and unexposed
Case-control study—For matched studies, give matching criteria and the number of controls per case N/AVariables7Clearly define all outcomes, exposures, predictors, potential confounders, and effect modifiers. Give diagnostic criteria, if applicable32.1. Case Definitions, Demographics and Study OutcomesData sources/ measurement8 * For each variable of interest, give sources of data and details of methods of assessment (measurement). Describe comparability of assessment methods if there is more than one group2
Table 1Cases were defined as patients over 18 years of age with a new diagnosis of LC between January 1st, 2007 and December 31st, 2017, by topography coding consistent with LC in OCR (C34) and exclusion of pathology not consistent with LC (e.g., hematopoietic malignancies, melanoma and Kaposi sarcoma), which is in keeping with Cancer Care Ontario’s definition. Additional patients were identified if LC was listed as cause or comorbidity on the death certificate, if not already captured in OCR data.Bias9Describe any efforts to address potential sources of bias3cancer-specific 5-year survival for LC across LHINs, adjusted for patient age, sex, income quintile, rurality index, distance to nearest hospital (in kilometres), nearest hospital type (academic, community, small, unknown), LC stage at diagnosis, LC histology, co-morbidity status by ACG, timeliness of care (divided into 5 quintiles), and assessment by medical or radiation oncology. For this analysis, timeliness of treatment, radiation and medical oncology visits were modelled as time-varying covariates.Study size10Explain how the study size was arrived at3–4
Figure 1Quantitative variables11Explain how quantitative variables were handled in the analyses. If applicable, describe which groupings were chosen and why3Cox-ModelStatistical methods12(a) Describe all statistical methods, including those used to control for confounding3We used a Cox-model approach to compare overall and cancer-specific 5-year survival for LC across LHINs, adjusted for patient age, sex, income quintile, rurality index, distance to nearest hospital (in kilometers), nearest hospital type (academic, community, small, unknown), LC stage at diagnosis, LC histology, co-morbidity status by ACG, timeliness of care (divided into 5 quintiles), and assessment by medical or radiation oncology. For this analysis, timeliness of treatment, radiation and medical oncology visits were modelled as time-varying covariates. The Wald Chi-Square test was used to assess for statistical differences between groups.(b) Describe any methods used to examine subgroups and interactions (c) Explain how missing data were addressed3Patients with missing data were excluded from relevant analysis. E.g. lung cancer survival estimate excluded patients with no prior OCR record and diagnosed at death as cancer was only identified at time of death(d) Cohort study—If applicable, explain how loss to follow-up was addressed
Case-control study—If applicable, explain how matching of cases and controls was addressed
Cross-sectional study—If applicable, describe analytical methods taking account of sampling strategy (e) Describe any sensitivity analyses N/A
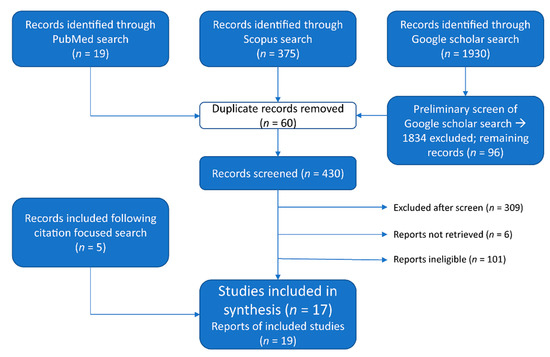
ResultsParticipants13 *(a) Report numbers of individuals at each stage of study—eg numbers potentially eligible, examined for eligibility, confirmed eligible, included in the study, completing follow-up, and analysed4
Figure 1(b) Give reasons for non-participation at each stage N/A(c) Consider use of a flow diagram
Figure 1Descriptive data14 *(a) Give characteristics of study participants (eg demographic, clinical, social) and information on exposures and potential confounders4-5
Table 2(b) Indicate number of participants with missing data for each variable of interest N/A(c) Cohort study—Summarise follow-up time (eg, average and total amount) Outcome data15 *Cohort study—Report numbers of outcome events or summary measures over time8-9
Table 4,
Table 5Case-control study—Report numbers in each exposure category, or summary measures of exposure Cross-sectional study—Report numbers of outcome events or summary measures Main results16(a) Give unadjusted estimates and, if applicable, confounder-adjusted estimates and their precision (eg, 95% confidence interval). Make clear which confounders were adjusted for and why they were included8-9
Table 4,
Table 5(b) Report category boundaries when continuous variables were categorized (c) If relevant, consider translating estimates of relative risk into absolute risk for a meaningful time period Other analyses17Report other analyses done—eg analyses of subgroups and interactions, and sensitivity analyses N/A
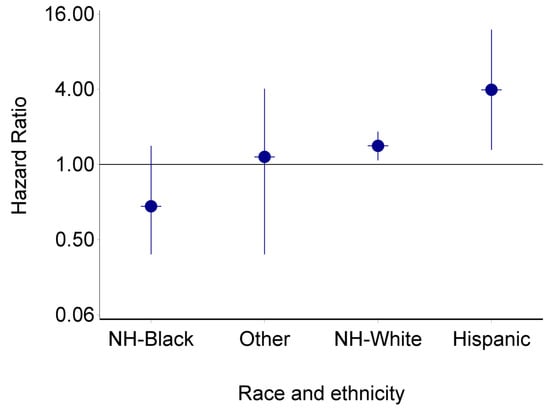
DiscussionKey results18Summarise key results with reference to study objectives11Significant variability in LC survival exists across health regions in Ontario. Our data demonstrate that both patient- and disease-related characteristics contribute significantly to this observed variability in survival, with LC stage at diagnosis and histologic subtype exhibiting the greatest impact on survival. However, variability in patient and disease characteristics between health regions did not account for all the observed variability in adjusted cancer-specific survival across LHINs, suggesting that other system factors may play a contributing role. We adjusted for several system factors in a multivariate analysis including timeliness of care, size of closest hospital, and specialist consultation, yet variability in survival across health regions persisted.Limitations19Discuss limitations of the study, taking into account sources of potential bias or imprecision. Discuss both direction and magnitude of any potential bias13One limitation of our study was the inability to obtain LHIN level smoking rates or patient access to smoking cessation counselling.
Another limitation is related to the imperfect nature of database cohort analyses, recognizing that coding of information is not always accurate.
Our cohort definition was in keeping with Cancer Care Ontario’s definition, in an effort to minimize inaccuracies. Interpretation20Give a cautious overall interpretation of results considering objectives, limitations, multiplicity of analyses, results from similar studies, and other relevant evidence14Significant variability in LC survival exists across health regions in Ontario, not completely accounted for by variability in those patient and disease characteristics available in our data, suggesting that other patient or system factors play a contributing role. A regional approach to improvement efforts will be required to identify the root causes contributing to unique regional system factors that influence survival to develop targeted improvement strategies. Governing bodies should consider the uniqueness of individual health regions to ensure that resources are equitably distributed in such a way that address unique regional needs and should consider tracking additional quality metrics, beyond timeliness of care, that have the most potential to impact LC survival.Generalisability21Discuss the generalisability (external validity) of the study results14Finally, since there is no reason to believe that these variations across regions is unique to the province of Ontario, our findings are likely relevant to other jurisdictions with similar health care systems in Canada and elsewhere.
Other information Funding22Give the source of funding and the role of the funders for the present study and, if applicable, for the original study on which the present article is based14Funding: William M. Spear Endowment Fund in Pulmonary Research and the Richard K. Start Memorial Fund, Queen’s University, Ontario, Canada. This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care (MOHLTC). Parts of this material are based on data and information compiled and provided by CIHI and Ontario Health. The analyses, conclusions, opinions and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred








留言 (0)