
記住我
Blue nevi and related melanocytic proliferations (Table 1) are a heterogenous group of congenital and acquired melanocytic lesions, which have in common several clinical, histologic, and immunochemical features. They have been termed dermal dendritic melanocytic proliferations because they are usually composed, at least in part, of dendritic melanocytes within the dermis. Clinically, many of the lesions exhibit a blue-gray color, attributed to the deep (dermal) location of abundant melanin pigment in conjunction with the Tyndall effect. The latter is the selective absorption of longer wavelength components of light by dermal melanin pigment with reflection of shorter wavelength (blue) components from the skin.
 TABLE 1:
TABLE 1: Classification of Dermal Dendritic Melanocytic Proliferations
HistogenesisHistologically, many of the lesions contain spindled and dendritic melanocytes, which are thought to resemble immature melanocytic cells migrating from the neural crest to the skin during embryonic development. It is hypothesized that the lesions arise due to arrested migration within the dermis of these immature cells. Although it is widely believed that the cells are immature melanocytes, it has also been suggested that they could be Schwann cells exhibiting melanocytic differentiation or a common neural crest-derived cell exhibiting differentiation along both melanocytic and Schwann cell lines.1
CONGENITAL DERMAL MELANOCYTOSESThe congenital dermal melanocytoses are hamartomatous lesions and include Mongolian spot, nevus of Ito, nevus of Ota, nevus fusocaeruleus zygomaticus, acquired dermal melanocytosis of the face and extremities, and dermal melanocyte hamartoma. They all present as blue-gray macules and are histologically very similar, being characterized by scattered dendritic melanocytes within the reticular dermis. Unlike blue nevi, there is no associated stromal sclerosis. They tend to be hypocellular lesions, which are very subtle histopathologically and the diagnosis may easily be missed, particularly if inadequate clinical information is provided to the pathologist at the time the sections are interpreted or insufficient attention is given to the clinical presentation. Distinction between the various congenital dermal melanocytoses is based on their clinical features, which have been reviewed in detail elsewhere.2
BLUE NEVUSThe term “blue nevus” was originally used by Jadassohn to describe dark blue lesions of the skin and was introduced into the literature in 1906 by Max Tièche.3 In 1949, Allen4 first used the term “cellular blue nevus” (CBN) for a “benign variant of the blue nevus which, because of its rich cellularity and striking abundance of melanin pigment, often is misdiagnosed as melanosarcoma.” In his textbook published in 1961, Lever5 referred to 2 types of histologic appearance that blue nevi may present: a common type (that described by Tièche) and a cellular type (as described by Allen). Many variants of blue nevus have since been reported, but so-called common blue nevi and CBN are the major and most common subtypes.
The so-called common blue nevus is composed predominantly of dendritic melanocytes. Although the adjective “common” is applied to these lesions, they are not necessarily the most common of the blue nevus variants, and furthermore, variable degrees of overlap exist between so-called common blue nevi and CBN. Consequently, they will be referred to as dendritic blue nevi (DBN) in this review.
In our experience, blue nevi commonly show histologic overlap between DBN and CBN. It is our practice to categorize them as one or other subtype on the basis of the predominant component (ie, ≥50% of the lesion).
Dendritic Blue Nevus (So-called Common Blue Nevus, Jadassohn-Tièche Type) Clinical FeaturesDBNs are usually acquired, but may be congenital in rare instances. They may arise at any age (present at birth to 79 y), but are biopsied most often during young adulthood (mean 38.6 y).6 They present as well-demarcated, slightly raised papules, often <1 cm in diameter, ranging in color from blue to gray to blue-black to black.2,7 Most occur in skin, commonly on the extremities and the face. Rare cases of DBN have also been reported in extracutaneous locations, such as the subungual region,8,9 the orbit and conjunctiva,10–13 oral cavity,14–20 sinonasal mucosa,21–23 bronchus,24 esophagus,25 lymph nodes,26–28 vagina,29 uterine cervix,30–37 endometrium,38 penis,39 and prostate40–43 and we have observed cases at almost all of these as well as some other sites.
Amelanotic blue nevus, also referred to as hypopigmented blue nevus,44–46 is an uncommon variant, accounting for 2.7% of all blue nevi in 1 series.47 It shows a similar age and sex distribution to DBN and may occur at any body site.
Rare patients present with multiple DBNs which may occur in a familial setting,48 in the setting of LAMB syndrome49 (Lentigenes, Atrial and Mucocutaneous myxomas and multiple Blue nevi) or NAME syndrome50 (blue Nevi, Atrial myxomas, Myxoid neurofibromas, Ephelides), or apparently sporadically, in which case they may be diffusely distributed51–55 or grouped in a circumscribed anatomic area (so-called agminated blue nevi).56–58 Other clinical variants include eruptive,54,59 linear,60 and target61 blue nevi. The relationship of the very rarely reported LAMB syndrome and NAME syndrome to the Carney complex (which shows some overlap in its phenotypic features—epithelioid blue nevi (EBN), psammomatous melanotic schwannoma, mucocutaneous lentigenes, multiple myxomas at a variety of sites, adrenal hyperplasia, and large cell calcifying Sertoli cell tumor)62–64 has not, to our knowledge, been established but appears likely.
Pathologic FeaturesDBNs are characterized by a dermal or submucosal proliferation of elongated, bipolar, spindle-shaped cells, sometimes grouped in short fascicles, often with an intervening grenz zone. The melanocytes show elongated dendritic processes and contain variable amounts of melanin pigment in the cytoplasm, including within the dendritic processes. Some dermal sclerosis is present and variable amounts of collagen are interspersed with the melanocytes. Usually there are also scattered melanophages (Fig. 1). Cellular atypia is minimal and mitotic figures are almost never seen.2,6,7 Very rare cases of DBN associated with multiple adjacent similar satellite lesions and termed “agminated blue nevi” by some authors56–58 (postulated to be due to perivascular spread of nevus cells), but lacking evidence of malignant behavior, have been described.65–67
 FIGURE 1.:
FIGURE 1.: Examples of dendritic blue nevus. A, Poorly circumscribed dermal spindle cell proliferation separated from the overlying epidermis by a grenz zone. B, Bipolar melanocytes with elongated dendritic processes, some containing cytoplasmic melanin pigment, along with scattered melanophages. C, More cellular example composed of a dermal spindle cell proliferation separated from the overlying epidermis by a grenz zone. D, Bipolar melanocytes with elongated dendritic processes, many containing cytoplasmic melanin pigment, along with scattered epithelioid melanophages.
Amelanotic blue nevus may show a variety of architectural patterns: spindle cell proliferations with entrapment of collagen identical to DBN; sclerotic fibroma-like pattern composed of a proliferation of spindle cells interspersed with thick collagen bundles (similar to sclerosing blue nevi); or a pattern resembling a scar. In contrast to DBN, they are characterized by absent or minimal melanin pigment within the spindle melanocytic cells and a paucity of melanophages (Fig. 2).45,47 Amelanotic blue nevi may be misdiagnosed (as occurred in almost three-quarters of cases in 1 series47) as other entities such as dermatofibroma, scar, dermal Spitz nevus, desmoplastic nevus or amelanotic melanoma.47,68 Each of these entities is readily distinguished from blue nevi with a combination of clinical correlation, careful examination of the morphologic features, and immunohistochemical studies.
 FIGURE 2.:
FIGURE 2.: Amelanotic/hypomelanotic/hypopigmented blue nevus. Proliferation of spindle cells lacking pigment, interspersed with thick collagen bundles.
DBN in which there is a preponderance of central fibrosis and hyaline sclerosis have been termed “sclerosing blue nevi.”2
Nodal DBN are rare and are usually located in the capsule, sometimes with extension into perinodal adipose tissue. Their distinction from metastatic melanoma may be problematic, particularly in sentinel lymph node specimens.69–71 They are composed of a combination of elongated cells with dendritic processes and pigment-laden melanophages, and histologically resemble their cutaneous counterparts.26–28
Differential DiagnosisCutaneous and extracutaneous DBN exhibiting typical morphologic features including melanin pigment are not usually difficult to diagnose. The appearances of hypopigmented DBN may raise other bland spindle cell proliferations in the differential diagnosis, such as dermatofibroma or fibroblastic scar tissue. Immunohistochemistry for melanocytic markers will clarify the diagnosis in morphologically equivocal lesions. Sclerosing DBN may resemble desmoplastic melanoma or other dermal spindle cell proliferations, but can be distinguished by its negligible cytologic atypia and the characteristic HMB-45 (and usually S-100) positive dendritic cells, which contrasts with melanoma.2,72,73
Nodal DBNs are composed of capsular aggregates of dendritic cells with associated melanophages. The most common melanocytic lesions occurring in lymph nodes are nevus cell aggregates, which are also located in the capsule, but in contrast to DBNs, are composed of small round to oval cells with round to oval nuclei and scant cytoplasm, devoid of significant cytologic atypia and largely lacking pigment.26 In contrast, melanoma cells in lymph nodes are usually located in the subcapsular sinus or parenchymal regions and show greater cell size, nuclear variability, vesicular chromatin and prominent nucleoli, and may show mitotic activity.70,71
Cellular Blue Nevus Clinical FeaturesCBN may be diagnosed at any age (range, 6-85 y), but most commonly in adults under 40 years of age. Females are more frequently affected than males (ratio 2.2:1).6 CBN present as pigmented nodules ranging from a few millimeters to a number of centimeters in size. The commonest sites of involvement are the scalp, lower back, and buttocks, but they may occur on the limbs and in other locations,6,74 and have also been reported in mucosal6,75,76 and subungual77 locations. The duration of the lesion before diagnosis ranges from months to years, and in some cases, the lesion is present at birth.6,74 Rare cases of congenital giant CBN occurring on the scalp have been reported.78–80
The plaque-type variant of blue nevus (PTBN) is usually considered a variant of CBN (although it is usually characterized histologically by both DBN and CBN areas). They are present at birth or arise in early childhood, and may enlarge during puberty. The majority of such lesions affect the scalp; rare cases involve the arm or hand, or mucosal sites.81 PTBN appears as a blue-gray pigmented area measuring 1 or more centimeters in diameter and is composed of a single plaque or a confluence of several small macules and/or papules.59,81–86
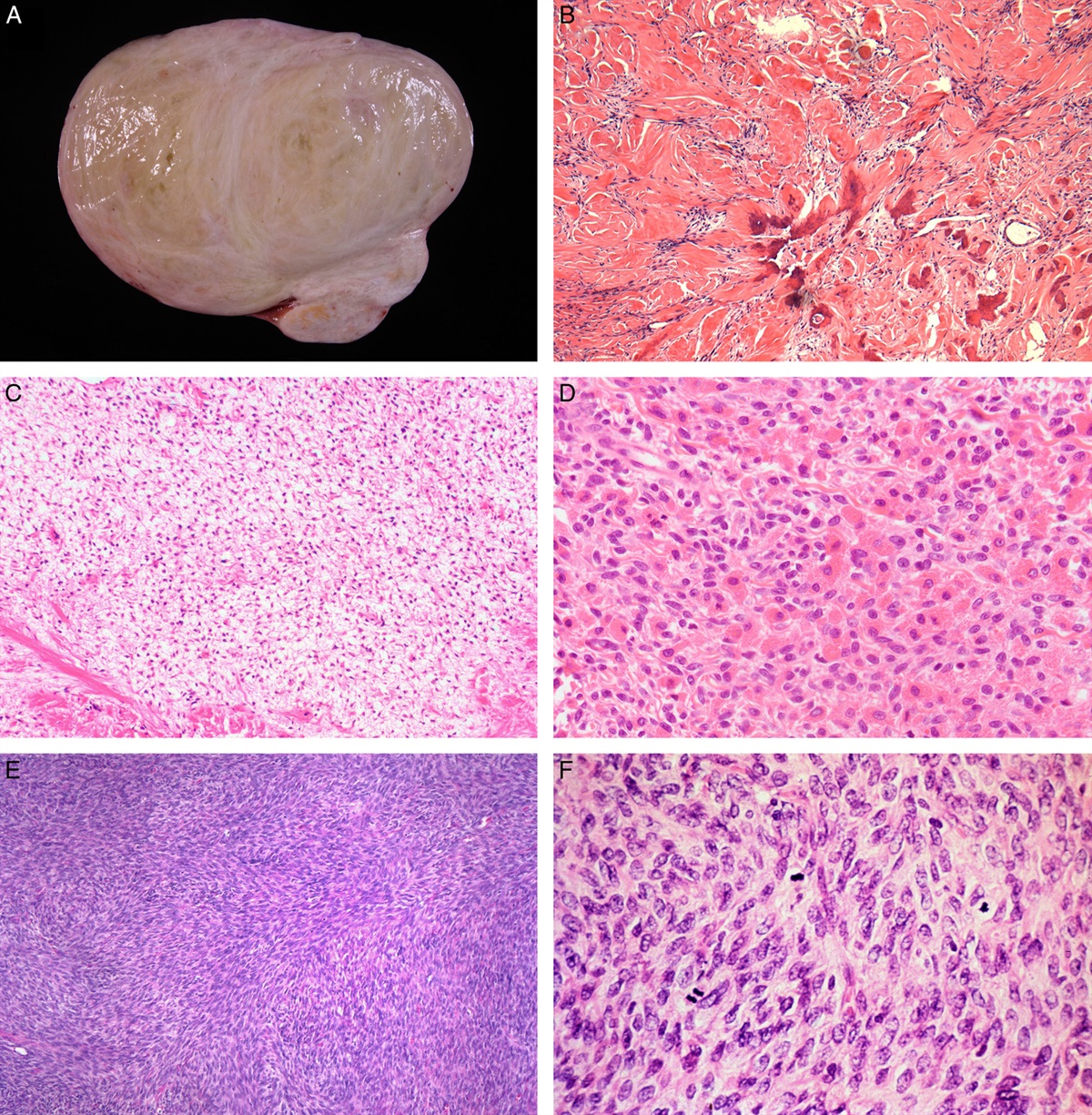
Pathologic FeaturesMacroscopically, CBN are well-circumscribed nodular dermal tumors, which are often heavily pigmented, with intact overlying epidermis.6 The majority of the pigment is in macrophages (melanophages) whereas the melanocytes are usually only lightly pigmented. CBN show considerable histologic heterogeneity. A variety of patterns have been described, but a common feature is vertically oriented, sometimes bulbous extension of the lesion into the subcutaneous adipose tissue (Fig. 3A). In the commonest (mixed biphasic) pattern, the lesion occupies the superficial and mid dermis, sometimes extending to the deep dermis and subcutis. It is composed of oval to plump spindle cells intermingled with dendritic melanocytic cells and variable numbers of melanophages (Figs. 3A, B). Sclerosis is often prominent.6,74,87 The rare amelanotic variant of CBN (Figs. 4A–C) shows similar morphologic features to classic CBN and is composed of a cellular spindle cell proliferation with little or no cytoplasmic melanin pigment and includes few, if any, admixed melanophages.47,88
 FIGURE 3.:
FIGURE 3.: Cellular blue nevus. Typical appearance, comprising a wedge-shaped lesion with extension into the subcutaneous adipose tissue (inset), composed of oval, spindle and rounded cells admixed with variable numbers of melanophages (A and B).
 FIGURE 4.:
FIGURE 4.: Example of amelanotic cellular blue nevus. A, Wedge-shaped lesion with bulbous extension into the subcutaneous adipose tissue. B, Alveolar pattern, characterized by well-defined nests of amelanotic oval to spindle cells. The alveolar pattern may merge with C, areas with a fascicular pattern in which the tumor is composed of fascicles of amelanotic spindle cells with clear cytoplasm, surrounded by fibrous tissue containing very occasional melanophages.
Well-defined nests of amelanotic cells surrounded by collagen and variable numbers of dendritic melanocytes and melanophages comprise the alveolar pattern of CBN (Fig. 4B). The merging of the alveolar pattern into nevoid cell sheets or areas of a fascicular pattern is common. Occasionally, the nests may be separated by areas of loose, edematous tissue, which may represent precursors to cystic change.74 In the fascicular or neuronevoid pattern, the tumor is composed of fascicles of amelanotic spindle cells with clear cytoplasm, surrounded by fibrous tissue containing dendritic melanocytes and melanophages. Neuroid structures are frequently interspersed with the tumor.74 Occasional tumors may contain balloon cells with vacuolated/foamy cytoplasm.89 Rare cases may exhibit myxoid stroma.90 Mitotic activity is usually absent and should be low (<1/mm2).74 Focal areas of necrosis have been reported as being present in rare cases of otherwise benign CBN,74 although in our view, the presence of any necrosis is an atypical finding and concerning for malignancy. If isolated mitotic activity or necrosis is present but no other atypical findings (including cell crowding, nuclear atypia, hyperchromasia, or expansile growth) are seen, we report such tumors as atypical CBN and state that it is not possible to predict the biologic behavior/malignant potential of the tumor with certainty from its morphologic features but consider the risk of aggressive behavior to be low. The cells are usually positive for S-100 and HMB-45,91,92 although we have seen some cases which are negative for S-100 and exhibit only weak or focal positivity for HMB-45. In view of the often prominent melanin pigmentation of these lesions, the use of a red chromogen for immunohistochemistry usually allows easier interpretation than a brown chromogen. A rare angiomatoid variant of CBN containing numerous dilated blood vessels has been described.93
Kazakov and Michal noted the presence of “ball in mitts” structures in CBNs, composed of a single centrally placed rounded or oval melanocyte (ball) encircled by a single dendritic cell (mitt) with an oval or spindle-shaped nucleus and slender bipolar processes containing melanin and surrounding at least a quarter of the diameter of the rounded melanocyte. They also found “microalveolar structures,” composed of 2 to 10 central rounded cells surrounded by one or more dendritic cells similar to those seen in the “ball in mitts” structures. The authors noted that similar structures may occur in combined nevi, deep penetrating nevi, acquired melanocytic nevi and in common blue nevi, and in light of this, they proposed that there may be a spectrum of evolution from common acquired nevus to combined nevus to CBN and deep penetrating nevus (DPN) through a progressive expansion and prominence of the “ball in mitts” and “microalveolar structures.”94 However, differences in the clinicopathologic characteristics of blue nevi (and their variants) and common nevi are against this hypothesis.
Histologically, PTBN shows a combination of features seen in DBN and CBN. In addition to pigmented spindle and dendritic cells, aggregates of variably pigmented epithelioid and often clear melanocytic cells are present, as are foci extending deeply into subcutaneous tissues. The dermal melanocytes are often found in a periappendageal and perivascular location (Figs. 5A, B). No significant cytologic atypia is seen and mitotic activity is rare (Fig. 5C).85,86,95 The lesional cells are positive for S-100, HMB-45 (Gp100), and Melan-A/Mart-1 (A103).84 Busam et al84 suggested that onset in childhood and the presence of heterogenous (DBN-like and CBN-like) areas are features that distinguish PTBN from CBN. However, as PTBN are composed of areas resembling CBN, histologic distinction between these entities is not possible without correlation with the clinical features. For this reason, we regard PTBN as a clinicopathologic variant of CBN characterized by large size and extension along fascial planes.
 FIGURE 5.:
FIGURE 5.: Plaque-type blue nevus. A, Plaque-like tumor centered in the dermis with extension around adnexal structures and B, extensive involvement of the subcutis, composed of C, largely nonpigmented aggregates of oval melanocytic cells, along with scattered pigmented dendritic cells. A deep component involving subcutaneous adipose tissue and deep fascia may predominate.
Differential DiagnosisCBNs show a range of histologic features, which may cause them to be misdiagnosed as melanoma. Rare cases of melanoma arising within preexisting CBN have also been reported.75,96 Also, congenital giant CBNs may show intracranial involvement and such tumors are associated with a high rate of malignant transformation, often occurring before puberty.78,79,97 Like melanoma, CBN is usually composed of large epithelioid and/or spindle cells, lacks maturation with depth, may extend deeply, may be pigmented, and may contain an occasional mitotic figure.6,74,98 Perineural extension and intralymphatic tumor may be seen in CBNs and does not indicate malignancy. Various histologic features have been proposed as being helpful for the discrimination of CBN and CBN-like melanoma. However, these criteria are not infallible and in those cases with some atypical but not overtly malignant features, confident prediction of likely biological behavior may not always be possible on the basis of the morphologic assessment of the primary tumor. Pathologic features reported as favoring malignancy include tumoral necrosis, cytologic atypia and pleomorphism, and frequent mitoses (>2/mm2).6 Other findings that favor melanoma over CBN include the presence of large pleomorphic epithelioid cells, cell crowding (usually associated with increased cell nuclear to cytoplasmic ratios), an “infiltrating” growth pattern (where the margins of the tumor are irregular, as opposed to the generally rounded or “pushing” margins of CBN), expansile growth, the presence of junctional activity (especially if it is atypical or shows pagetoid epidermal invasion), or the presence of a “sarcomatoid” growth component, in which sheets of spindle cells replace small fascicular aggregates and nests of melanocytes.6,74
A recent study documented poor interobserver reproducibility among expert pathologists in the diagnosis of atypical CBN and so-called malignant blue nevus, highlighting the lack of uniformly accepted and applied criteria for the pathologic diagnosis of these lesions.99 Further studies preferably correlated with molecular data and long patient follow-up periods are required to determine the morphologic criteria that best predict biologic behavior in these lesions.
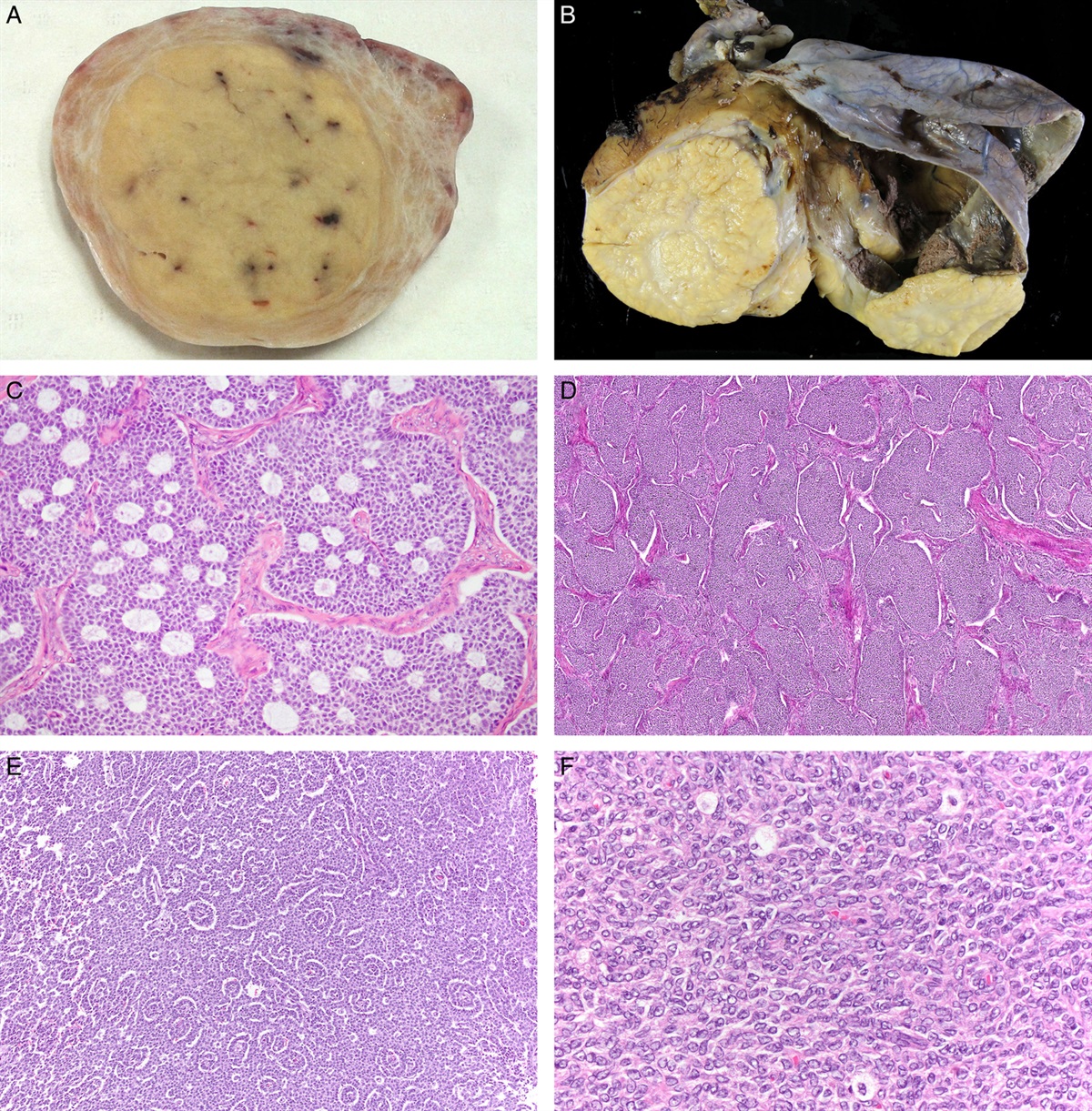
Lymph node involvement by CBN is rare.6,100 Nodal involvement often takes the form of subcapsular sinus and parenchymal deposits (Figs. 6A, B), in contrast to the predominantly capsular location of nodal nevus cell aggregates and DBN.26,74,100,101 Such deposits of CBN pose difficulties in distinction from melanoma, and the possibility that the lesion is a metastatic CBN-like melanoma cannot always be ruled out due to the relatively short follow-up period in some reported cases.102 Comparison with the histology of the primary cutaneous tumor (which is invariably present, Fig. 6C) may help in arriving at the correct diagnosis, and prevent excessive and inappropriate treatment.74 However, unequivocal distinction between nodal CBN and CBN-like melanoma is not always possible, and therefore in such cases, a guarded prognosis should be given.
 FIGURE 6.:
FIGURE 6.: Nodal cellular blue nevus. A, Large subcapsular and parenchymal deposits. B, Cellular tumor composed of round to oval cells containing variable amounts of cytoplasmic pigment. The cells show some cytological atypia and occasional mitoses are present. C, The corresponding cutaneous cellular blue nevus, which shows typical architectural (inset) and cytologic features and is devoid of significant cellular atypia.
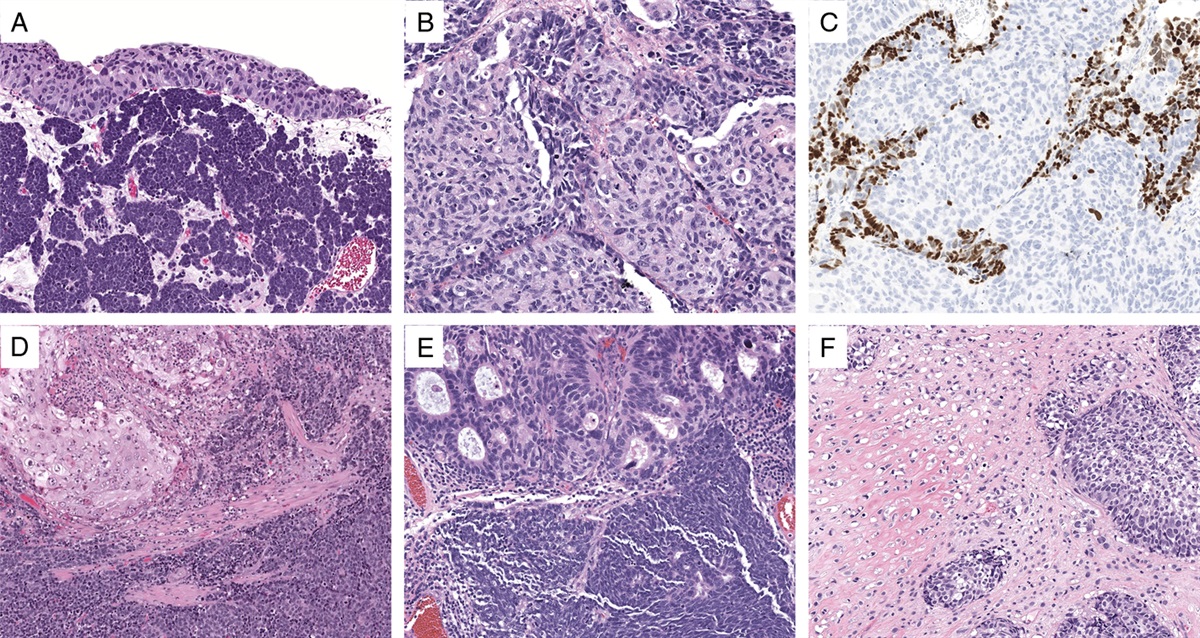
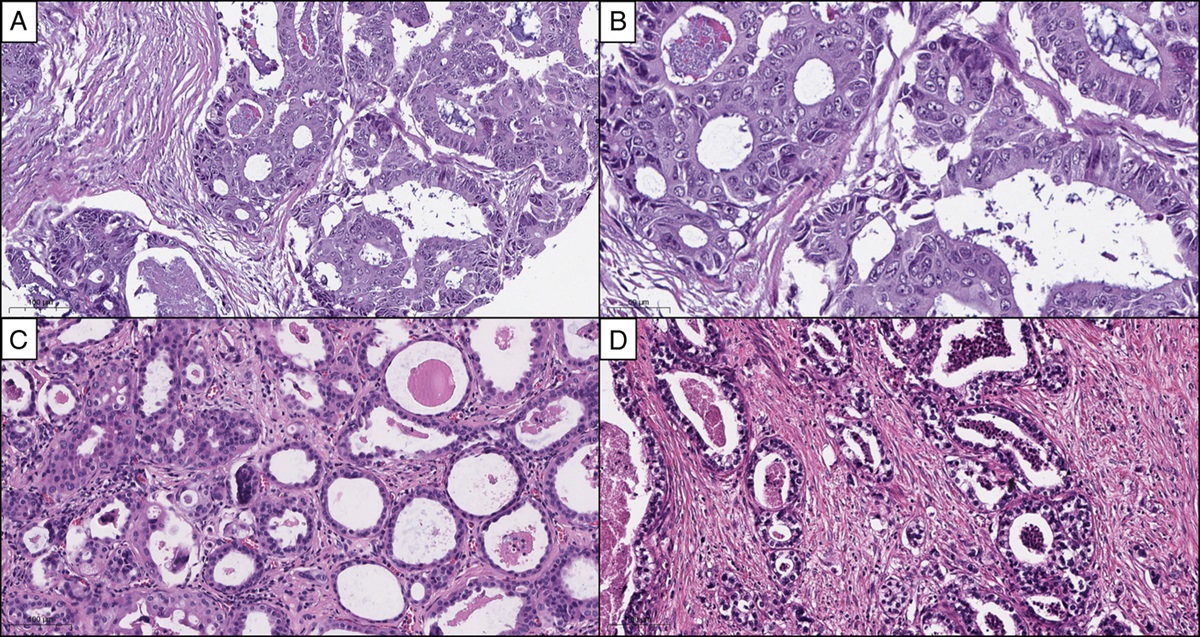
Combined NevusCombined melanocytic nevi are composed of more than one nevus type in a single lesion. They may occur in both cutaneous and mucosal sites,10,74,103 and may be composed of any combination of common acquired nevi, blue nevus variants, or Spitz nevi. Blue nevi, particularly deep penetrating nevi, are common components,104–106 but DBN10,103,105 or CBN74,105 may also be present (Figs. 7A, C). We consider that other histopathologically similar tumors that have been reported under a variety of other terms including clonal nevus, inverted type A nevus, nevus with focal atypical epithelioid components, and atypical dermal nodule in benign melanocytic nevus may also represent examples of combined nevi.105,107 Barnhill and colleagues have proposed the term “nevus with phenotypic heterogeneity” for this group of lesions. Although this name is probably a more accurate reflection of the pathogenesis of these melanocytic tumors, the terminology has not been widely adopted, possibly because the term “phenotypic heterogeneity” may engender clinical concern about the nature of the lesion.
 FIGURE 7.:
FIGURE 7.: Combined nevus. A to C, Combined nevus with banal compound nevus (C) admixed with epithelioid deep penetrating nevus (D).
“Compound Blue Nevus”Rare cases of compound blue nevus have been reported.108–110 The junctional component was reported to be composed of single dendritic melanocytes, a morphologic description that equally applies to normal junctional melanocytes. The dermal component comprised pigmented dendritic melanocytes arranged singly and in fascicles, similar to DBN. Melanophages were also present in the dermis. No significant cytologic atypia or mitotic activity should be observed.108–110 We have not seen a convincing example of this entity; upon review of cases that were diagnosed by others as compound blue nevus, we classified them as DPN and combined nevus.
Clinical Behavior of Blue NeviIn general, the blue nevi described above behave in a benign fashion. Involvement of regional lymph nodes is rare, as has been discussed above. Very rare cases of persistence or recurrence of blue nevi [DBN, CBN, and combined nevi with blue nevus component(s)] have been reported, often, but not always, after incomplete excision.6,111,112 The recurrent lesions usually resemble the original tumor, although occasionally, they may exhibit degenerative (“ancient”) changes or atypical features (pleomorphism and mitotic activity), the latter raising concern for subtle malignancy.111 Persistent or recurrent blue nevi seem to follow a benign course, and the atypical and degenerative morphologic changes seen in some recurrent tumors were not associated with aggressive behavior in most cases. It has been suggested that these changes are likely related to the inflammatory response to the previous surgical procedure.111 However, as clinical recurrence of blue nevi may herald malignant transformation, careful clinical follow-up and histologic examination of the recurrent lesion is warranted.74,113,114
BLUE NEVUS-LIKE MELANOMA (SO-CALLED MALIGNANT BLUE NEVUS)Malignant blue nevus is a term first coined by Allen and Spitz to describe blue nevus-like lesions which had resulted in metastasis and patient death in some cases.115 It has since been used by several authors to denote various entities: malignant change arising in a preexisting CBN,74,113,116,117 melanoma arising at the site of a (previously excised) blue nevus,113,118–120 melanoma with cytoarchitectural features resembling CBN but apparently arising de novo,121–123 or melanoma with an admixed residual benign CBN component.113,118,124–126
So-called malignant blue nevi comprise a rare group of melanocytic tumors, which in some cases are not easy to classify precisely as benign or malignant purely on the basis of the morphologic features of the primary tumor. Mones and Ackerman127 have published a comprehensive review of cases reported in the literature bearing these diagnoses, and are strongly critical of the use of such terms. These authors are firmly of the opinion that all such lesions should be categorized into “blue nevus,” “melanoma,” and “melanoma in association with a blue nevus.” Although their interpretation is largely based on a logical analysis of the literature, precise categorization of such lesions is not always possible, nor is it possible to reliably predict from histologic features of the primary tumor the biologic behavior of atypical melanocytic lesions showing some morphologic similarities to blue nevus or CBN. Nevertheless, we agree that the term malignant blue nevus is inadvisable, given the juxtaposition of the adjective “malignant” with the noun “nevus,” which connotes a benign lesion. It is far better, we believe, to term such lesions as “blue nevus-like melanoma (BNLM) or atypical blue nevus-like lesion of uncertain malignant potential,” depending on the degree of atypia and the degree of histologic certainty of the malignant potential of the lesion. If the latter term is used, the evidence in favor of a diagnosis of nevus and melanoma respectively should be discussed in the report and, whenever possible, a favored diagnosis proffered. Furthermore, in this situation, or whenever genuine doubt exists about the biologic potential of the lesion, it is probably appropriate to seek an opinion from one or more experienced colleagues. Rather than adding new diagnostic entities to the dermatopathologic lexicon, these terms indicate the difficulty in histologically classifying such lesions as benign or malignant, and reflect the uncertainty in prediction of their behavior. This allows communication of the level of concern about a given lesion to the clinician, facilitating the formulation of an appropriate management plan.128,129 In this difficult area, we believe that such an approach is of more value than to attempt to precisely categorize all such lesions as either benign (nevi) or melanoma when there is a significant possibility that such categorization may be inaccurate. Further study of these cases, correlated with prolonged clinical follow-up and preferably also with molecular data, may be helpful in refining diagnostic criteria for this uncommon but difficult and problematic group of tumors.
Most of the cases of BNLM are associated with CBN (either pure CBN or CBN in combination with other nevus types). Melanoma apparently arising in association with a pure DBN is very rare.122,130,131 Connelly and Smith113 proposed 2 criteria to enable distinction of BNLM from metastatic or nodular melanoma, namely the lack of a junctional component and the presence of a background benign blue nevus. Clearly, correlation with clinical details is also important if a diagnosis of metastatic melanoma is being considered, particularly to establish whether the patient has a known history of melanoma and whether there is evidence of metastatic disease elsewhere.
Genetic studies of small numbers of cases have suggested that aberrations commonly seen in melanomas (such as mutations in CDKN2A and alterations in chromosomes 10q, 1p, and 17) are not identified in BNLM, suggesting that the molecular pathogenesis of BNLMs is distinct from that of conventional melanoma.125 Further genetic studies are required to confirm these findings. A recent study reported the presence of frequent somatic mutations in the heterotrimeric G protein alpha-subunit, Guanine nucleotide binding protein (G protein), q polypeptide, in blue nevi (83%) and ocular melanoma of the uvea (46%).132 The mutations occurred exclusively in codon 209 in the Ras-like domain and resulted in constitutive activation, turning Guanine nucleotide binding protein (G protein), q polypeptide into a dominant acting oncogene. These findings provide molecular evidence of a histogenetic link between these tumors which, as we recognized many years ago, show morphologic similarities in a subset of cases.
BNLM is rare. They often occur in older individuals (often >45 y), are usually large (3-13 cm), and may show clinical evidence of a residual CBN. Many of the reported cases exhibit local invasion or widespread metastasis.116–118,121,123,124,133–136 The scalp is the commonest site of involvement, followed by the face, buttocks, and chest. Rarely BNLMs in other locations, such as the vulva,118 have also been reported.
Cases of BNLM reported in the literature have behaved very aggressively, with a majority exhibiting metastases leading to patient death.113,121,123,125,131,135,137–142 There are probably a number of factors contributing to this poor outcome, including delayed diagnosis and treatment of the malignant component, an overestimate due to difficulties in separating nonmetastasizing BNLM from atypical CBN, and reporting bias. However, metastasis or death may be delayed up to 19 years after the diagnosis.118,133 Reliable prediction of the behavior of BNLM based on histopathologic features has not always been successful, although some studies have suggested that Breslow thickness may be predictive of outcome.122 A recent comprehensive analysis of 23 patients with BNLM treated at the Melanoma Institute Australia (incorporating the Sydney Melanoma Unit), the largest series reported to date, found that clinical outcome was similar to that of conventional melanoma patients when matched for tumor thickness and other important prognostic factors.143
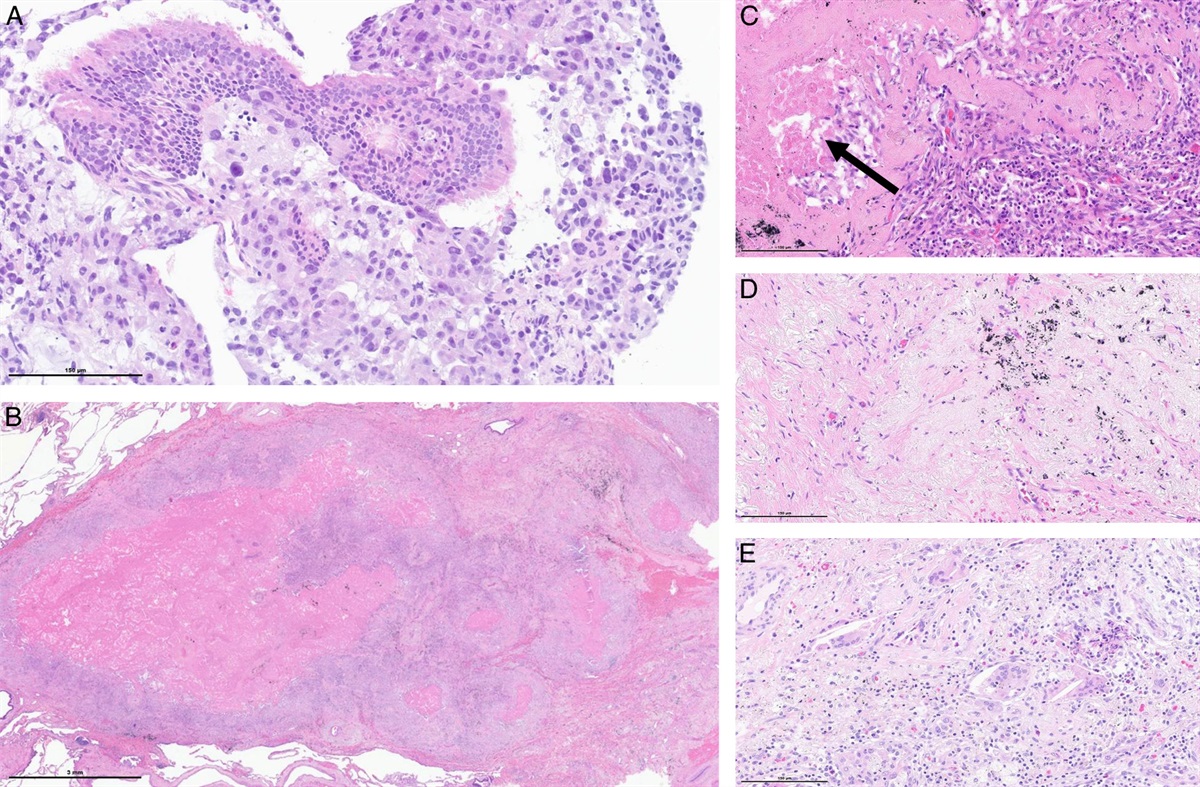
Pathologic Features and Differential DiagnosisBNLM can generally be distinguished from CBN by the presence of a frankly malignant component (Figs. 8A, B).118 Histologically, BNLM is characterized by widespread necrosis in many cases (Figs. 8C, D),6,116,133,134,144 and palisading of cells around the areas of necrosis may be seen.133,134 However, necrosis is not a common finding in all series.122 Focal necrosis has been reported to occur rarely in otherwise typical CBN,74 although it is our opinion that, in the absence of prior biopsy or trauma, the presence of necrosis is very concerning for malignancy. Other criteria supportive of a diagnosis of BNLM include high mitotic rate (>2/mm2), abnormal mitotic figures, vascular invasion, excessive cell crowding, expansile growth and marked cytologic pleomorphism and atypia (Figs. 8D, E). Occasional cases of BNLM may, however, be associated with a low mitotic rate.113,118,121,122,135,136,138–142,145–147
 FIGURE 8.:
FIGURE 8.: Examples of blue nevus-like melanoma (so-called malignant blue nevus). A, Cellular lesion resembling amelanotic CBN at low power. B, Prominent cytologic atypia (nuclear pleomorphism and very prominent nucleoli) and isolated mitotic figures (arrow). C, Another example showing a highly cellular and nodular tumor confined to the subcutaneous adipose tissue, and showing densely cellular nodules exhibiting areas of heavy pigmentation composed primarily of melanophages and necrosis (N). D and E, The tumor cells are oval to spindle in shape, show moderate cytologic atypia, including scattered mitotic figures (arrows), and are variably pigmented. Note the presence of admixed melanophages and necrosis (N). CBN indicates cellular blue nevi.
Cutaneous metastases from melanoma may rarely mimic BNLM, and when they lack atypical cytologic features, they may mimic blue nevus. These lesions are composed of pigmented fusiform, dendritic and epithelioid melanocytes surrounding dermal collagen bundles. Occasional atypical epithelioid melanocytes, scattered mitotic figures and an associated perivascular lymphocytic infiltrate may be present, all representing subtle clues to the correct diagnosis. Nevertheless, correlation with the clinical features is critical to definitive diagnosis.148
“ATYPICAL” CELLULAR BLUE NEVUSA rare variant of blue nevus with many morphologic features of CBN but with some additional atypical features (that in isolation would be evidence raising the possibility of melanoma) without clear cut evidence of malignancy, (ie, a lesion intermediate or indeterminate between typical CBN and melanoma) has been referred to as “atypical CBN” (ACBN),74,98,149 “locally aggressive,”144,150 “extensive,”151,152 or CBN-like melanocytic tumor of uncertain malignant potential.153 ACBNs tend to occur in the buttock or sacral region of young or middle-aged adults. All lesions of ACBN reported so far have been solitary, predominantly dermal nodules, some extending into the superficial subcutis.74,98 Clinically, such lesions resemble CBN, but histologically, they contain worrisome features, such as asymmetry, hypercellular foci, focal cytologic atypia, and occasional mitoses (<2/mm2).74,149,153 Atypical mitotic figures are not seen.118 Elder and Murphy153 proposed diagnostic criteria for ACBN as CBN that display some, but not all, of the following features: (1) size >3 cm, (2) increased cellularity, (3) cellular pleomorphism, (4) increased mitotic activity, and (5) areas of necrosis. However, a recent study involving the assessment of a series of cellular blue melanocytic neoplasms by 14 experienced dermatopathologists showed that there is substantial disagreement among pathologists about the definitions and biologic nature of such tumors, in particular those thought to have atypical features (ACBN).99 The results highlight the lack of clear, consistent diagnostic criteria, resulting in poor interobserver reproducibility in the diagnosis of such lesions. Clearly, further study of this group of lesions correlated with clinical follow-up data (and molecular findings) is required to clarify the clinical significance of atypical morphologic features in CBN. In our view, it is likely that ACBN does not represent a distinct entity and may be composed of a mixture of CBN with atypical histologic features and a subtle CBN-like low grade form of melanoma. The recent suggestion that the latter should be referred to as melanocytoma (as a distinct intermediate entity in contrast to the traditional dichotomous diagnostic categorization of melanocytic tumors as either nevus or melanoma) is a proposal with some merit and worthy of further consideration and study. However, to prevent it becoming a “waste basket” category liable to expansion and inappropriate (over) usage, precise diagnostic criteria would need to be defined.
Some authors found that ACBNs tend to recur, and may acquire a more aggressive phenotype if incompletely excised,153 whereas other studies found no evidence of recurrence or metastasis in their cases.149 Until further data emerges, it therefore seems an appropriate course of action to regard such lesions as being of uncertain/indeterminate malignant potential and to treat them with complete resection, followed by close clinical follow-up for local recurrence or regional/distant spread.
Differential DiagnosisThe distinction of ACBN from melanoma can be difficult. High mitotic activity (>2/mm2), atypical mitotic figures, marked cytologic atypia, cell crowding, expansile growth, and necrosis favor melanoma,113,137 but it has been suggested that the finding of atypical mitotic figures seems to be the most helpful distinguishing feature.6 As described above, ACBN is distinguished from CBN by the presence of one, or occasionally more, of the following features: asymmetry, hypercellular foci, focal cytologic atypia, and occasional mitoses (<2/mm2).
Maize et al154 demonstrated that ACBN showed more chromosomal aberrations than unequivocally benign CBN (which showed none), but which are less frequent and fewer in number than unequivocally malignant lesions resembling blue nevi (BNLM) using comparative genomic hybridization. The small number of cases and the limited follow-up period in this study, however, did not permit prognostic stratification of the ambiguous cases (ACBN) based on their degree of chromosomal aberration.154 Nevertheless, these data may provide some molecular basis for the presence of the atypical morphologic features and, furthermore, evidence that the traditional dichotomous categorization of melanocytic tumors into benign and malignant may not always be appropriate (that is, that an intermediate/borderline category of melanocytic tumors (“melanocytomas”) or perhaps low grade forms of melanoma may exist.
Deep Penetrating Nevus, Epithelioid Blue Nevus, and Pigmented Epithelioid Melanocytoma Deep Penetrating NevusThe term “deep penetrating nevus” was coined by Seab et al155 in 1989 to describe a lesion with worrying histologic features but benign clinical behavior, which was often misdiagnosed as melanoma. In Seab et al's series, none of the lesions recurred or metastasized after a mean follow-up of 7 years. In our experience, DPN most commonly occurs as part of a combined nevus (ie, as part of a nevus composed of more than one nevus cell type).105,156
DPN usually presents as a solitary lesion, and rarely as multiple lesions.155,157 Patients with DPN are usually between 10 and 30 years of age when diagnosed (although they may occur at any age), with no significant sex predilection. The most common sites of involvement are the head, neck and shoulder, and less often trunk, upper arm, hip, and thigh. Most lesions are well-demarcated, darkly pigmented papules or nodules, usually <10 mm in size.155 Variable pigmentation is common, particularly in those lesions forming part of a combined nevus.
Histologically, DPNs are relatively symmetric and well-demarcated lesions extending to the deep reticular dermis and sometimes into subcutis, and often exhibit an inverted wedge-shaped silhouette (Fig. 9A). They are usually composed of nests and fascicles of predominantly ovoid epithelioid cells, which often contain cytoplasmic melanin pigment, the latter
留言 (0)