
記住我

Non-small cell lung cancer (NSCLC) comprises 80% of lung cancer diagnoses, and in the pre-screening era, patients still present most frequently in advanced stages of the disease. In around 30% of patients, the tumor is resectable but locally advanced, and the addition of systemic chemotherapy to resection has proven beneficial, with a 5% gain in overall survival (OS) in both the adjuvant and neoadjuvant chemotherapy setting.1–3 Systemic therapy has evolved, with currently chemo-immunotherapy as the new standard for patients without targetable mutations, due to clearly superior outcome results. Three randomized trials have recently confirmed the superiority of adding immunotherapy to the standard of care (neo)adjuvant chemotherapy. Addition of immunotherapy significantly improved the event free survival with significantly higher rates of pathological complete response (pCR) and major pathologic response (MPR) and a tolerable safety profile, as demonstrated in the NEOTORCH, Checkmate 816 and Keynote 671 studies.4–6
Neoadjuvant administration of chemotherapy +/- immunotherapy and radiotherapy has some advantages over adjuvant therapy, that is, systemic treatment following resection. Importantly, patient compliance and tolerance of systemic treatment are often better before resection, and potential downstaging of the tumor can lead to superior operability.7 In addition, neoadjuvant therapy has the potential for early elimination of micrometastases.8 In the era of immunotherapy, it may also be advantageous to try to sensitize the immune system against as much tumor antigen as possible, speaking in favor of neoadjuvant versus adjuvant approaches. Finally, the possibility of immediate evaluation of the treatment effect outweighs the disadvantage of not having treatment-naïve tissue available for investigation of tumor biology. In contrast, neoadjuvant therapy-induced fibrosis due to tumor regression may render surgery more difficult, although surgeons in specialized centers do not consider this a significant drawback. Likewise, there remains a small chance that delayed surgery, due to initial administration of systemic therapy, causes some patients to become inoperable, either due to tumor progression or patient deterioration, but this seems to be a rare event.9
Pathological response, measured as the percentage of residual viable tumor (RVT) in the resected lung, is currently used as a surrogate end point for many clinical studies. MPR, defined as ≤ 10% RVT, has been established as a surrogate end point for OS after neoadjuvant chemotherapy, potentially improving the efficiency of trials and expediting scientific advances.10 MPR was initially chosen as a threshold over pathologic complete response (pCR=0% RVT) since the latter was only infrequently achieved (~2% of patients) compared with MPR (~10% of patients). Interestingly, subsequent clinical trials investigating neoadjuvant (chemo)immunotherapies, such as CheckMate 816 and NADIM, reported pCR in up to 63% and MPR in up to 83% of the patients, respectively.6 Although it remains to be seen if MPR can also act as a surrogate marker for survival after neoadjuvant (chemo)immunotherapy like it does after neoadjuvant chemotherapy, initial reports have shown a strong prognostic potential of pathological evaluation in this setting.11
In patients with targetable mutations, the addition of targeted therapy in the adjuvant setting demonstrated a highly statistically significant and clinically meaningful improvement of disease-free survival and OS in resected disease, as has been shown in the practice changing ADAURA trial in EGFR mutated NSCLC.12 On the other hand, the efficacy of targeted therapy in the neoadjuvant setting is still under evaluation13 but it seems to be well tolerated and associated with pathological response in patients with stage IB-III disease, and without treatment-related surgery delay, as has been shown in the phase II umbrella trial NAUTIKA1 in ALK positive NSCLC.13
PATHOLOGICAL REGRESSION/RESPONSE GRADING – CURRENT GUIDELINESAlthough there have been proposals for evaluating histomorphological response in lung cancer specimens resected after (radio)chemotherapy dating back to 1997,14,15 it was the multidisciplinary paper by the International Association for the Study of Lung Cancer (IASLC) published in 2020 that formalized and expanded those recommendations into guidelines applicable in the clinical trial setting as well as in daily practice.16 It has to be noted though that these recommendations should be regarded as preliminary as they partly rely on expert consensus rather than evidence derived from actual case series. Therefore, they may be subject to change once evidence from more studies on the subject becomes available.
Since the basis of all pathological assessment is gross assessment, focused tissue sampling becomes the most important step in the evaluation of pathologic treatment response in the neoadjuvant setting. Precise microscopic evaluation can only be performed if sufficient tissue has been submitted to guarantee reliable results. The IASLC guidelines provide detailed practical assistance in recognizing the tumor bed and sampling the pretreated tumor.16 Key points are the recommendation to section the tumor in the plane of the maximum tumor dimension, to photograph the cut surface and to map the submitted blocks on the photograph. Tumor beds up to 3 cm diameter should be entirely submitted for histological evaluation. If the tumor bed is larger than 3 cm, at least the largest and most representative whole section of the tumor should be entirely submitted, including grossly necrotic or fibrotic areas. This deviates from traditional grossing techniques in tumor pathology where previously emphasis was placed on primarily submitting viable tumor for diagnosis and staging. In case no RVT is detected on initial assessment or the detected RVT content lies around the MPR cut-off, submission of additional tumor blocks or of the entire tumor may become necessary. The submitted blocks should cover the border of the tumor including around 1 cm of the surrounding lung parenchyma to define the tumor edges.
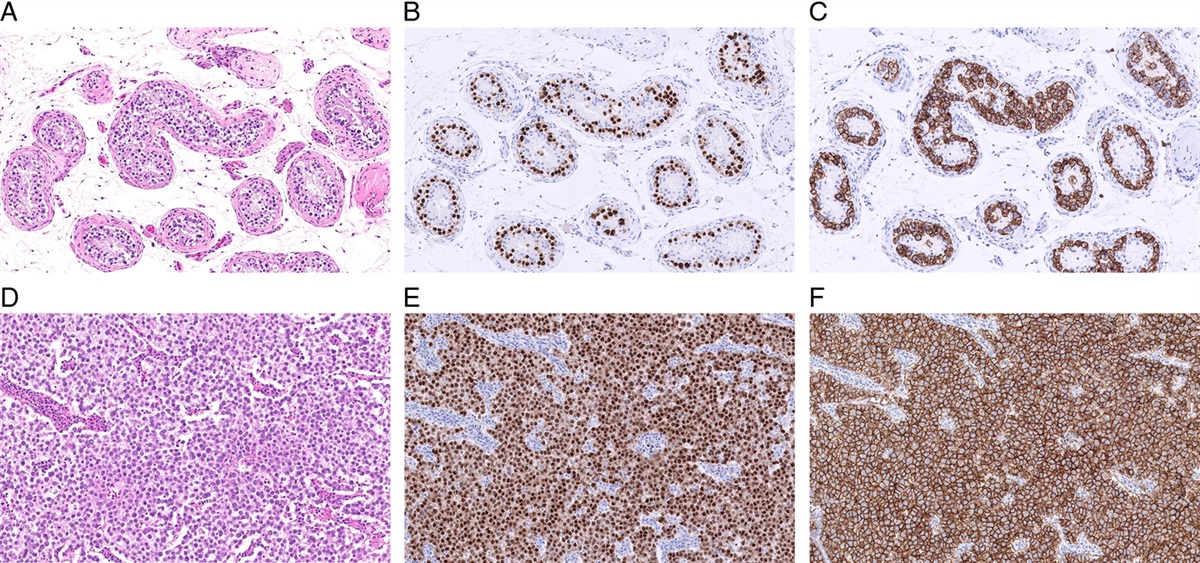
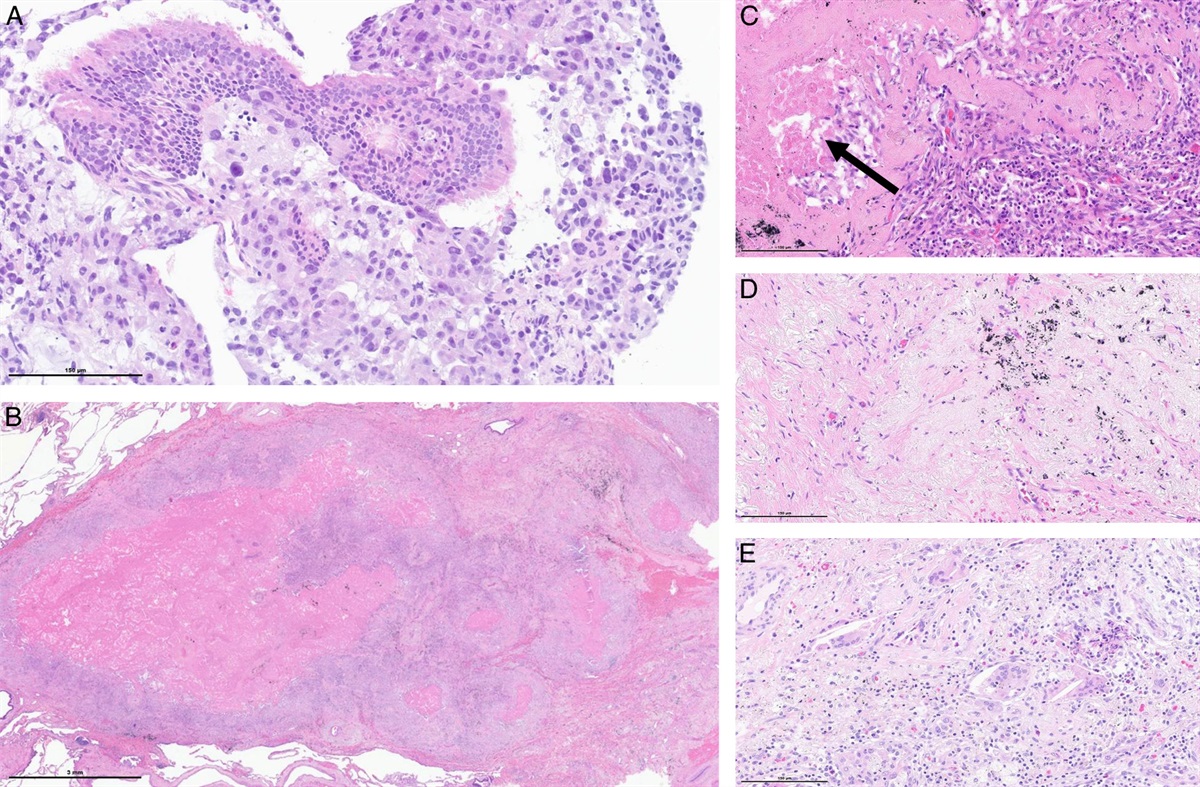
Histological assessment is based on the identification of the “tumor bed,” the area where the tumor was located prior to neoadjuvant therapy, consisting of a combination of RVT, stromal tissue (including fibrosis and inflammation), and necrosis (Figs.1 and 2). Together these 3 components account for 100% of the tumor bed and the percentage of individual components in the tumor bed shall be estimated in 10% increments (or single percentages when <5%) on each slide and then averaged over all slides containing the tumor bed. RVT may be detected throughout the tumor bed, frequently in the periphery, but in general without predictable localization. It is noteworthy that the stromal tissue includes any type of fibrosis and inflammation. As the different characteristics of fibrosis have not been found to be clinically relevant, they need not be further specified. Inflammation is regarded as a part of the stromal component if it is confined to the tumor bed but shall be disregarded if representing reactive changes in the surrounding non-neoplastic lung. Moreover, extracellular mucin counts as part of the RVT if viable tumor cells are identified but as stroma in case they are not. This mirrors the guidelines issued for esophageal adenocarcinoma resected after neoadjuvant therapy.17,18 Until now, the only prognostically significant parameter for prognosis after chemotherapy appears to be the percentage of RVT,14,19–23 often expressed as pCR, defined as the absence of RVT in the primary tumor and lymph nodes, and MPR, defined as ≤10% of RVT in the primary tumor bed. Initial reports support these thresholds also for tumor evaluation after neoadjuvant (chemo-)immunotherapy6,11,24,25
 FIGURE 1:
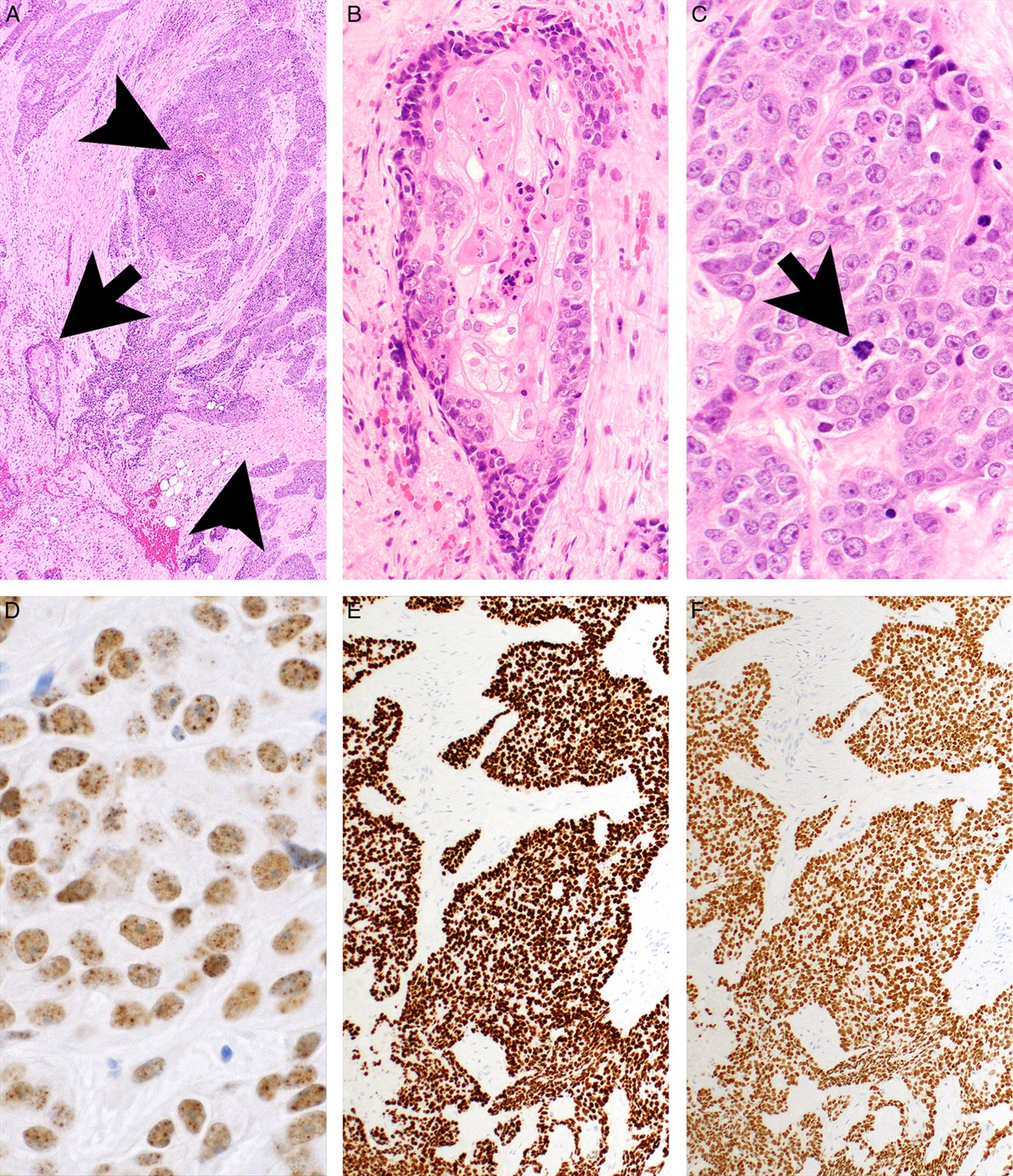
FIGURE 1: (A) Adenocarcinoma in the diagnostic transbronchial biopsy. (B) Overview of the tumor resected after neoadjuvant immuno-chemotherapy, showing complete pathological response. (C-E) Histological detail of the tumor bed, consisting of (C) necrosis (arrow), proliferative fibrosis and inflammation, (D) scarring fibrosis with (E) giant cells and cholesterol clefts. (A-E: H&E; A: ×40 magnification; B: overview, C-E: ×20 magnification).
 FIGURE 2:
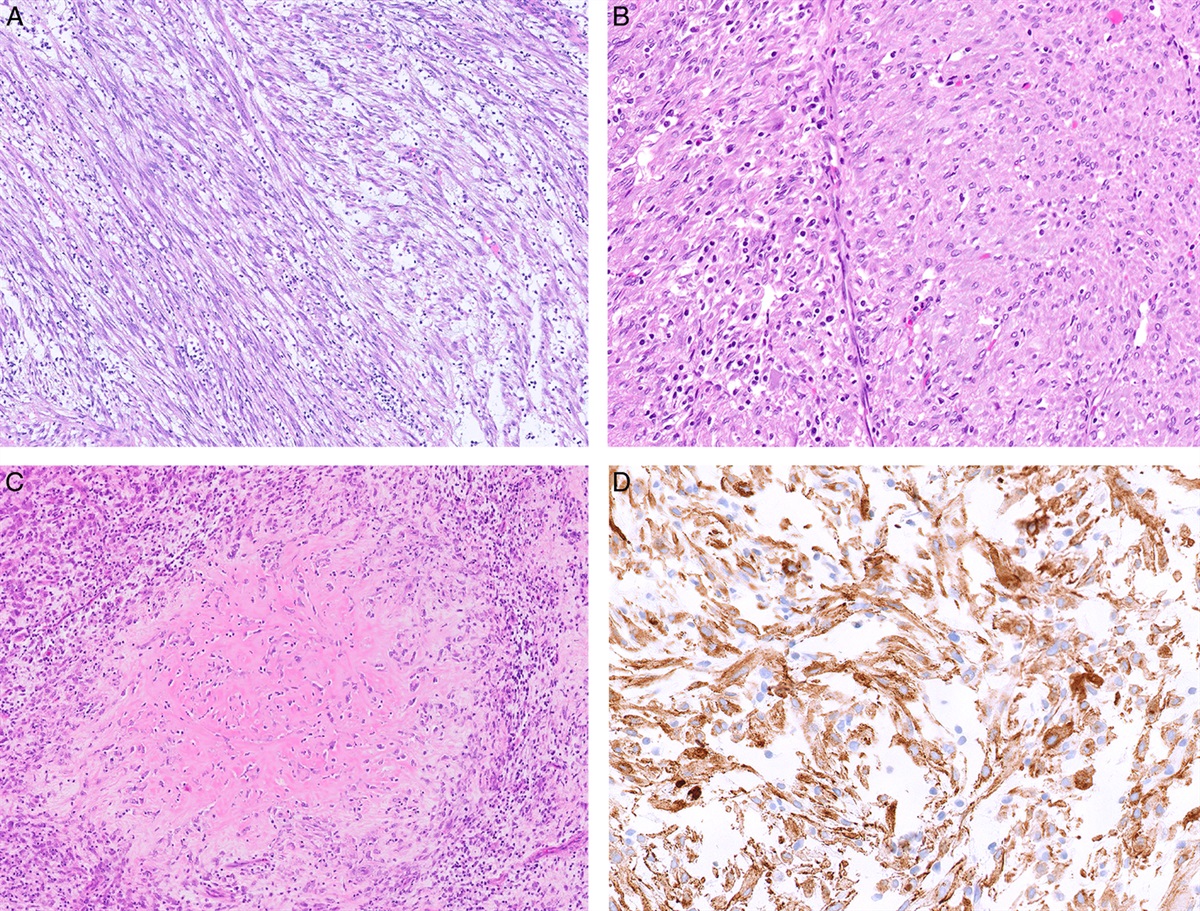
FIGURE 2: Solid adenocarcinoma without histologically evident response to neoadjuvant chemotherapy. (A) Overview of the tumor bed, comprising >90% or residual vital tumor and a lympho-follicular reaction in the periphery of the lesion. (B) A higher magnification of the area marked in A depicts the only minimal content of necrosis and lack of fibrosis. (C) Overview of the tumor invading the pleura. (D) Higher magnification of the area marked in A, highlighting the invasion of the tumor cells (arrows) beyond the outer elastic layer of the pleura (arrowheads). (A, B: H&E; C, D: EvG; A: overview, B, D: x40 magnification, C: x10 magnification).
This IASLC approach was recently tested in an international concordance study, including 11 expert thoracic pathologists from 4 continents.26 Scoring of pathologic response according to the IASLC criteria on hematoxylin and eosin (H&E)–stained slides from 84 resected NSCLC specimens was excellent for pCR (inter-rater agreement [IRA]=0.94) and good for MPR (IRA=0.84), in line with previous single institution studies.21,23,27 Most of the interpretation discordances were observed in the RVT range between 30% and 65%. The areas of discrepancies included (i) variability of tumor bed measurement due to the difficulty to distinguish the tumor bed from preexisting scars or inflammation, (ii) difficulty to distinguish tumor cells from an intimately admixed prominent lymphoplasmacytic stromal component on H&E-stained slides, (iii) problems of separating reactive pneumocytes from lepidic adenocarcinoma and (iv) interpretation of mucin in mucinous adenocarcinoma, which should have counted as viable tumor but was not evaluated as such by some pathologists.26 In this study, fibrovascular cores of papillary carcinoma were regarded as RVT rather than stroma. This approach simplified scoring and most likely reduced interobserver variability.26
As pathology is moving into the digital era, it is hoped that image analysis will become a valuable tool, not only to standardize the evaluation of treatment response but also to alleviate the increasing workload as a result of tumor scoring. Promising initial reports of image analysis algorithms tested versus human assessment of MPR on the LCMC3 study cases have recently been presented, demonstrating a strong correlation between the 2 with comparable disease-free survival rates.28,29 The algorithm was trained to distinguish and quantify the tumor bed, viable tumor tissue, necrosis, tumor-associated stroma, and adjacent non-tumoral lung parenchyma. In the 136 LCMC3 cases evaluated, AI-based predictions of RVT tended to be consistently lower than the RVT visually assessed by the pathologists in the cases with low tumor content, most probably due to the fact that the algorithm meticulously partitioned the tumor cells from the other compartments, but the pathologists tended to visually include also the tumor-associated stroma as RVT areas.29 The prognostic prediction of the AI-based RVT was superior for DFS and OS.29
Applicability of the recommendations by automated algorithms needs to be kept in mind when evaluating future amendments of scoring criteria if these more objective technical advancements are to be employed.
When the evaluation of treatment response after chemotherapy was initially described in 1997 in a small cohort of 40 lung cancer resection specimens, it seemed that its morphological aspect, characterized by the presence of marked scarry fibrosis in the region of the former primary tumor, concentric foci of fresh tumor necrosis and surrounding foam cell clusters with transition into vascular granulation tissue, was specific to therapy and not recognized in spontaneously regressed tumors.14 Only necrosis with directly adjoining viable tumor was detected in the control cohort of untreated tumors.14 However, spontaneous regression, morphologically undistinguishable from post-therapy changes, can occur in untreated tumors, making it paramount for the pathologist to receive pertinent clinical information.16,30
EVOLVING QUESTIONS AND CONTROVERSIES WARRANTING FURTHER STUDY Gross Examination of the Tumor/Tumor BedAs mentioned above, guidelines on the gross assessment of lung cancer resection specimens for the evaluation of treatment response are largely based on expert opinion, as studies specifically addressing the extent of tissue submission remain very few to date.
In 1997, Junker and colleagues did not provide specific information on how to submit the treated tumors and likewise many other studies on the topic failed to report how exactly the tumors were sampled.14,15,20–22,31–33 Some groups reported taking at least 1 section per cm of greatest tumor diameter without further specification.19,24
Aside from the recommendations by the IASLC as described above, some authors recommend an initially more extended macroscopic evaluation of the tumor bed, embedding every second section in tumors larger than 3 cm, resulting in a final microscopic evaluation of at least 50% of the tumor slides.34 In their study assessing response after neoadjuvant immunotherapy, Cottrell et al proposed to not only submit a complete cross-section from the largest diameter of the “tumor mass” as recommended by the IASLC but also a section from each additional 1 cm of greatest tumor dimension, in parallel to the grossing approaches suggested for breast tumors resected after neoadjuvant chemotherapy.35,36 Another group recommended to completely embed the tumor regardless of tumor size but recognized that this would surpass feasibility in daily routine practice.37,38 The most recent study on this particular topic is the only one to date that is evidence-based. Here, the authors performed a simulation study analyzing the accuracy rates of %RVT, MPR, and pCR of 31 pretreated primary lung tumors using traditional grossing (1 section per cm tumor) compared with the gold standard of submitting the entire tumor bed and identified the minimum number of tumor sections to be submitted to ensure the most accurate scoring of %RVT, MPR, and pCR. They found that achieving accuracy rates of at least 90% for assessing RVT and MPR/pCR scores requires submission of the entire primary tumor for smaller tumors and up to a maximum of 21 sections for larger tumors.39
Weighted Versus Unweighted EvaluationOriginally, the assessment of the percentage of RVT, necrosis, and fibrosis was recorded per each individual slide/tumor block and then averaged for all slides containing tumor bed. Such an unweighted approach, as endorsed by the IASLC, does not account for size differences of the tumor bed on the individual slides. To correct for this, the method of assessing a “weighted average” has been proposed, which includes measuring the 2-dimensional extent of the tumor bed (i.e., length and width) on each slide and taking this into account when averaging the overall percentage of RVT, fibrosis and necrosis.34
A comparison of the weighted and unweighted approaches of RVT scoring using a specifically designed MPR calculator was recently performed and demonstrated that similar RVT (and MPR) scores were achieved with both methods. For reasons of time-effectiveness and ease of application, the unweighted approach was recommended for general use, with the weighted approach reserved for those cases that were deemed difficult to score or in which the RVT content was close to the 10% MPR cut-off.26
Cut-offs for MPR May Differ According to Histological Tumor TypeThe prognostically most appropriate cut-offs for MPR may differ according to histological tumor type and possibly other, yet unknown parameters. Results from 3 independent single-center retrospective studies have challenged the application of a universal 10% cut-off for MPR in pretreated NSCLC. A US cohort comprised 272,21 a Swiss cohort 11722 and a Chinese cohort 316 NSCLC.23 All 3 groups could verify a 10% cut-off for squamous cell carcinoma but found a cut-off of 65%21,22 or 59%23 to be more appropriate for adenocarcinoma. However, this alternative cut-off for adenocarcinoma could not be verified in another large US cohort of 339 NSCLC patients, where 10% emerged as the universal cut-off regardless of histological tumor type.40 Further studies are warranted to elucidate the potential impact of the histological tumor type on the optimal MPR cut-off.
Assessment of Synchronous Multiple Tumor NodulesThere are no specific guidelines to date on how to assess treatment response in synchronous multiple tumor nodules.16,26 Nonetheless, some guidance shall be provided in the following, which should be adapted once more data become available.
When dealing with synchronous multiple tumor nodules, especially when those are located close to each other, radiological imaging from before administration of neoadjuvant treatment should be consulted to know if the tumor was initially multifocal or if multifocality has resulted from a heterogeneous mode of tumor regression/response. If multiple tumor nodules are deemed to derive from a solitary tumor or are interpreted to represent intrapulmonary metastases, one combined RVT score can be provided. If the tumor nodules are thought to be independent primary tumors according to clearly divergent histology (e.g., adenocarcinoma and squamous cell carcinoma), assessment of tumor regression/response should be performed for each tumor separately. In cases where the origin of synchronous tumors remains uncertain, detailed molecular typing is advisable to distinguish separate primaries from intrapulmonary metastases.26,41
Assessment of Lymph NodesAll lymph nodes must be submitted for histological evaluation of residual disease. The IASLC recommendations allow for an exception in cases where the lymph node diameter surpasses 2 cm in macroscopically clearly positive nodes. Embedding the most representative section is recommended in this rare and specific situation.16 In case no vital tumor is detected, the rest of the lymph node must be submitted. The definition of pCR includes no residual tumor in the lymph nodes in addition to no RVT in the primary tumor. Discordant response to treatment between the primary lung tumor and lymph node metastases may occur (Fig. 3). There are no recommendations to date to the question if any residual tumor in the lymph nodes should affect the MPR score of the primary tumor or whether it should be recorded separately.
 FIGURE 3:
FIGURE 3: Squamous cell carcinoma with discordant response to chemo-immunotherapy between primary tumor and the lymph node metastasis. (A) The overview of the centrally located tumor bed shows no residual vital tumor, which has been completely replaced by scarring fibrosis without necrosis. (B) Residual vital tumor in the hilar lymph node parenchyma (arrows), without evident signs of treatment response. P40 staining highlights the tumor cell nuclei stained in brown and confirms the diagnosis of a non-keratinizing squamous cell carcinoma (inset). (C) Histological detail of the tumor area in the lymph node. (A-C: H&E; A: overview, B: ×5 magnification, C: ×40 magnification).
Recently, lymph node-specific MPR after neoadjuvant chemotherapy has been reported to predict OS in patients regardless of MPR in the primary tumor, but the proposed cut-offs of RVT to determine MPR varied significantly.23,42 In a US cohort of 75 patients, the optimal cut-off was 70%.42 A Chinese study on 316 patients reported 8% as the optimal cut-off for lymph node-specific MPR.23
In the neoadjuvant immunotherapy setting, “nodal immune flare” (NIF) has been described as a phenomenon present in 16% (7/44) of patients in the NEOSTAR trial (NCT03158129), where nodal progression was suspected by CT and PET, showing increased 18F-fluorodeoxyglucose (18F-FDG) uptake, and eventually recognized to represent a type of pseudoprogression due to lack of histologically detectable tumor in tissue specimens.43 De novo non-necrotizing granulomas were found on histological examination of resected lymph nodes as compared with pretreatment fine needle aspiration cytology in all 7 patients with NIF and 3 patients without radiological abnormalities. Although sarcoid-like granulomas tend to be occasionally associated with neoplasms also outside of neoadjuvant therapy, and were described in single cases following chemotherapy,44 they were lacking in all 28 patients from the postchemotherapy control group.43 NIF was associated with an inflamed microenvironment in the lymph nodes as assessed by gene expression analyses, but not with pathological or radiological tumor responses, primary tumor microenvironment or toxicity to immunotherapy. The pathologist plays a crucial role in the assessment of residual disease in lymph nodes, underlining the necessity to submit all lymph node tissue for histological evaluation.
There is no consensus if the concept of micrometastases (metastases measuring up to 2mm) and isolated tumor cells (metastases measuring less than 0.2mm or 200 tumor cells), as outlined in the tumor-node-metastasis (TNM) classification,45 should be applied to lung cancer resections, including resections after neoadjuvant therapy. Further research is needed to evaluate the clinical value of the different approaches in those rare cases.
Regression Grading/Tumor Response Scoring after Immunotherapy and Targeted TherapyThe multidisciplinary recommendations for pathologic assessment of lung cancer resection specimens after neoadjuvant therapy as recommended by the IASLC are to be applied after all systemic therapies, including chemotherapy, chemoradiation, molecular-targeted therapy, immunotherapy, or any future novel therapies yet to be discovered, whether administered alone or in combination.16 Of course, this does not preclude further study in the field and does not rule out the possibility that adaptations of the grading scheme (according to specific therapies) may prove superior in the future. To date, no alternative scoring scheme or adaptation to the current recommendations has been adopted by the IASLC for evaluating treatment response in lung cancer specimens.
Quantitative immune-related pathologic response criteria (irPRC) for assessment of tumor regression after neoadjuvant anti-PD-1 treatment in NSCLC were initially proposed in 2018 by Cottrell and colleagues analyzing 20 patients from the first neoadjuvant nivolumab trial NCT02259621, for which 5-year clinical outcomes have recently been reported.35,46 Applying irPRC in all tumor types resected after neoadjuvant immunotherapy treatment was subsequently proposed by the same group under the name of “pan-tumor pathologic scoring to immunotherapy,” basing their recommendation on the assessment of over 250 tumors and 11 different tumor types.47 The differences with regard to the IASLC recommendations are that the RVT of the irPRC/pan-tumor pathologic scoring comprises not only the viable tumor cells but also the intratumoral stroma if signs of regression are not identified (Fig. 4). This viable tumor area is divided by the area of the tumor bed, containing the regression bed, necrosis and the tumor cell area and multiplied by 100 to arrive at the % of immune-related residual viable tumor (%irRVT). The stroma of the regression bed of the irPRC scoring therefore needs to be distinguished from the intratumoral stroma and any unspecific fibrosis and inflammation surrounding the tumor. As a result, the irPRC scoring scheme will always render an equal or higher percentage of RVT compared to the current IASLC scoring system (Fig. 4). The features proposed to identify the regression bed are claimed to be characteristic enough that regressed tumor may be recognized, even if not pathologically confirmed or even clinically suspected.47 Those features comprise proliferative fibrosis with neovascularization and evidence of immune activation (plasma cells, granulomas, tertiary lymphoid structures, and tumor-infiltrating lymphocytes) and cell death (interstitial foamy macrophages and cholesterol clefts).47 In lung cancer, this assumption cannot be readily accepted, as all described features can be found as confounders in the tumor bed, the immediate surrounding non-neoplastic lung parenchyma, and the resected lymph nodes in the absence of any previous systemic therapy.16,30,48,49
 FIGURE 4:
FIGURE 4: Comparison of assessing residual vital tumor as recommended by the IASLC versus the immune-related pathologic response criteria (irPRC). (A, B) Overview of an adenocarcinoma resected after neoadjuvant immuno-chemotherapy. (A) Applying the IASLC-criteria, residual viable tumor (marked in red) comprises tumor cells only, and accounts for <10% of the tumor bed, qualifying for major pathological response. (B) Applying the irPRC criteria, residual viable tumor (marked in red) comprises tumor cells and also the intratumoral stroma, and accounts for 30% of the tumor bed. (C) Histological detail of the heavily inflamed tumor area. (D) Fibrosis and necrosis (inset), located in the rest of the tumor bed. (A-D: H&E; A, B: overview, C, D: x40 magnification).
Additional Tissue Biomarkers, Including Tumor Microenvironment and Spatial MetabolomicsThe histomorphological evaluation of response to neoadjuvant therapy centers on the tumor cells, as their residual quantity is easily amenable to microscopic evaluation and has been consistently shown to have a prognostic impact.11,14,19–21,23 The tumor microenvironment (TME), including the tumor-associated stroma and immune cells, is much less well evaluated, as recently summarized.50 Regarding morphological characteristics evaluable using H&E-staining, stroma related to treatment can be fibroelastotic, fibromyxoid, or hyalinized, but the different quality seems to have no prognostic significance.21 Still, the type of fibrotic response and the associated tumor microenvironment including the immune infiltrate may be important features not yet sufficiently explored. The effect of neoadjuvant therapy on expression of PD-L1 and tumor-infiltrating lymphocytes is discussed controversially, as summarized elsewhere.49,50 Techniques such as spatial matrix-assisted laser desorption/ionization mass spectrometry imaging (MALDI-MSI) that localize hundreds to thousands of different metabolites directly from formalin-fixed paraffin-embedded tissue sections with cellular spatial resolution can further evaluate the complex therapy-induced changes. Applying machine learning on the data rendered tumor cell- and stroma-specific metabolic classifiers that were specific to NSCLC after neoadjuvant therapy and would further prognostically stratify groups of patients with and without MPR.51 Those techniques will not be readily applicable in current practice but draw attention to the possible exploitability of a qualitative assessment of the tumor stroma component as an additional future readout for therapy response.
Biomarkers Beyond Tissue – Circulating Tumor DNA (ctDNA)The use of non-tissue-based biomarkers in the form of “liquid biopsies” is a remarkable new tool in precision oncology. Fragments of double-stranded cell free DNA (cfDNA), measuring ~ 140 to 170nt in length, are continuously released into the circulation from normal cellular constituents, such a hematopoietic cells.52 In cancer patients, a variable fraction of cfDNA is derived from tumor cells. This is referred to as circulating tumor DNA (ctDNA), which is shorter, more fragmented, and measures <145nt in length. This size difference is exploited using fragment size analysis and selective sequencing to increase the sensitivity of ctDNA assays.53
Assessment of ctDNA in the early NSCLC setting may be more difficult than in metastatic tumors due to a lower tumor volume. Although this would imply a linear relationship between tumor volume and ctDNA levels, this is not necessarily the case. Studies have shown a better correlation between ctDNA levels and tumor necrosis, as opposed to tumor size per se.54 For example, NSCLC with higher amounts of necrosis and more invasive patterns of growth have higher levels of ctDNA compared to those without.55 How tumor cells release ctDNA may also influence ctDNA levels. Passive mechanisms such as apoptosis and necrosis, as well as active methods, like tumor-derived extracellular vesicle (EV) secretion, have been described.54 EVs have a lipid bilayer, preventing rapid DNA degradation, making them an attractive target for ctDNA analysis.56 Intrinsic molecular characteristics may also play a role, as lung cancer subclones carrying driver mutations were shown to release more ctDNA compared with those without driver mutations.57 Once present within the circulation, ctDNA has a half-life of ~1 to 2 hours, which is influenced by the rate of degradation and clearance from the circulation. Many variables affect ctDNA levels and subsequent detection, hence stringent methodology and appropriate assay selection is mandatory.
In clinical use, ctDNA clearance has been shown to correlate with treatment efficacy in advanced cancers.58 Based on this, its use in the neoadjuvant setting has recently been explored. Preliminary results from 2 ongoing clinical trials have shown promising data. In the CHECKMATE 816 trial, ctDNA levels were correlated with pCR and OS. Analysis was performed on the first day of the 3 neoadjuvant treatment cycles. Patients who cleared ctDNA, defined as undetectable ctDNA levels, had higher rates of pCR and a longer event-free survival.6 In the nivolumab plus chemotherapy group, ctDNA clearance was associated with pCR (11/24 patients; 46%). There was no pCR observed in patients without ctDNA clearance (0/19; 0%).6 This is comparable to findings in the NADIM phase II trial.38 Peripheral blood samples were prospectively collected before and after neoadjuvant treatment (before surgery). Patients with low ctDNA levels at baseline had significantly improved progression-free survival (PFS) and OS compared with those with high ctDNA levels (adjusted HR, 0.20; 95% CI, 0.06 to 0.63; P=0.006; and adjusted HR, 0.07; 95% CI, 0.01 to 0.39; P=0.002 for PFS and OS, respectively). In another small study, including 22 patients with tumors resected after chemotherapy, immunotherapy or a combination thereof, changes in ctDNA (measured as a R∆mean VAF) were also concordant with pathologic response.59 In addition, in the single-arm phase II LCMC3 trial, ctDNA reductions post-atezolizumab correlated with pathologic response (P=0.0001, r=0.38).60 These data highlight the possibility to use ctDNA in evaluating neoadjuvant therapy efficacy and its potential as a surrogate marker for pCR.
The utility of ctDNA in the neoadjuvant targeted therapy setting still needs to be evaluated. The ongoing LCMC4 Evaluation of Actionable Drivers in EaRly Stage Lung Cancer (LEADER) Neoadjuvant Screening Trial (NCT04712877) may provide more insight, as an important component of the trial involves the use of ctDNA to assess response to neoadjuvant targeted therapy and detection of minimal residual disease.61
CONCLUSIONDue to the evolving treatment landscape of lung cancer and since the standard of care for patients with advanced resectable NSCLC is increasingly moving into the neoadjuvant setting, assessment of treatment response by the pathologist has emerged as an increasingly important additional parameter of pathologic assessment. Although guidelines exist that should be followed in order to achieve worldwide standardization of evaluating pretreated NSCLC specimens, controversies and challenges still remain in the application of the recommendations regarding grossing and histomorphological evaluation, as summarized above and elsewhere.16,34,62 The digital era holds great promise in alleviating the increasing workload for pathologists, which is further compounded by the growing demand for more and more refined evaluation of an increasing number of sections per case. However, the promised gain in standardization will first require further refinement of existing guidelines and resolving persistent controversies, which can ideally be achieved by evidence-based means, if the data allows for it. In addition, as technology is advancing in the evaluation of the TME and the usage of blood-based assays for the evaluation of residual disease, alternative read-outs for therapy response may become the standard in future routine clinical practice.
It is hoped that the recent spotlight on pathology as a discipline guiding the advances of oncological treatment by providing a more immediate assessment of clinical efficacy will lead to a firm inclusion of the pathologist in trial design, thereby generating the data needed to answer the questions that remain in assessing treatment response in pretreated specimens.
REFERENCES 1. Pignon JP, Tribodet H, Scagliotti GV, et al. Lung adjuvant cisplatin evaluation: A pooled analysis by the LACE Collaborative Group. J Clin Oncol. 2008;26:3552–3559. 2. Burdett S, Pignon JP, Tierney J, et al. Adjuvant chemotherapy for resected early-stage non-small cell lung cancer. Cochrane Database Syst Rev. 2015;2015:CD011430. 3. Group NM-aC. Preoperative chemotherapy for non-small-cell lung cancer: a systematic review and meta-analysis of individual participant data. Lancet. 2014;383:1561–1571. 4. Wakelee H, Liberman M, Kato T, et al. Perioperative pembrolizumab for early-stage non-small-cell lung cancer. N Engl J Med. 2023;389:491–503. 5. Lu S, Wu L, Zhang W, et al. Perioperative toripalimab + platinum-doublet chemotherapy vs chemotherapy in resectable stage II/III non-small cell lung cancer (NSCLC): Interim event-free survival (EFS) analysis of the phase III Neotorch study. J Clin Oncol. 2023;41(36_suppl):425126. 6. Forde PM, Spicer J, Lu S, et al. Neoadjuvant nivolumab plus chemotherapy in resectable lung cancer. N Engl J Med. 2022;386:1973–1985. 7. Betticher DC, Hsu Schmitz SF, Totsch M, et al. Mediastinal lymph node clearance after docetaxel-cisplatin neoadjuvant chemotherapy is prognostic of survival in patients with stage IIIA pN2 non-small-cell lung cancer: A multicenter phase II trial. J Clin Oncol. 2003;21:1752–1759. 8. Blumenthal GM, Bunn PA Jr, Chaft JE, et al. Current status and future perspectives on neoadjuvant therapy in lung cancer. J Thorac Oncol. 2018;13:1818–1831. 9. Conroy MR, Dennehy C, Forde PM. Neoadjuvant immune checkpoint inhibitor therapy in resectable non-small cell lung cancer. Lung Cancer. 2023;183:107314. 10. Hellmann MD, Chaft JE, William WN Jr, et al. Pathological response after neoadjuvant chemotherapy in resectable non-small-cell lung cancers: proposal for the use of major pathological response as a surrogate endpoint. Lancet Oncol. 2014;15:e42–e50. 11. Deutsch JS, Cimino-Mathews A, Thompson E, et al. Association between pathologic response and survival after neoadjuvant therapy in lung cancer. Nat Med. 2024;30:218–228. 12. Wu YL, Tsuboi M, He J, et al. Osimertinib in resected EGFR-mutated non-small-cell lung cancer. N Engl J Med. 2020;383:1711–1723. 13. Lee JM, McNamee CJ, Toloza E, et al. Neoadjuvant Targeted therapy in resectable NSCLC: Current and future perspectives. J Thorac Oncol. 2023;18:1458–1477. 14. Junker K, Thomas M, Schulmann K, et al. Tumour regression in non-small-cell lung cancer following neoadjuvant therapy. Histological assessment. J Cancer Res Clin Oncol. 1997;123:469–477. 15. Junker K, Langner K, Klinke F, et al. Grading of tumor regression in non-small cell lung cancer : Morphology and prognosis. Chest. 2001;120:1584–1591. 16. Travis WD, Dacic S, Wistuba I, et al. IASLC Multidisciplinary recommendations for pathologic assessment of lung cancer resection specimens after neoadjuvant therapy. J Thorac Oncol. 2020;15:709–740. 17. Shia J, McManus M, Guillem JG, et al. Significance of acellular mucin pools in rectal carcinoma after neoadjuvant chemoradiotherapy. Am J Surg Pathol. 2011;35:127–134. 18. Bhatti AB, Akbar A, Khattak S, et al. Impact of acellular mucin pools on survival in patients with complete pathological response to neoadjuvant treatment in rectal cancer. Int J Surg. 2014;12:1123–1126. 19. Pataer A, Kalhor N, Correa AM, et al. Histopathologic response criteria predict survival of patients with resected lung cancer after neoadjuvant chemotherapy. J Thorac Oncol. 2012;7:825–832. 20. Blaauwgeers JL, Kappers I, Klomp HM, et al. Complete pathological response is predictive for clinical outcome after tri-modality therapy for carcinomas of the superior pulmonary sulcus. Virchows Arch. 2013;462:547–556. 21. Qu Y, Emoto K, Eguchi T, et al. Pathologic assessment after neoadjuvant chemotherapy for NSCLC: Importance and implications of distinguishing adenocarcinoma from squamous cell carcinoma. J Thorac Oncol. 2019;14:482–493. 22. Zens P, Bello C, Scherz A, et al. A prognostic score for non-small cell lung cancer resected after neoadjuvant therapy in comparison with the tumor-node-metastases classification and major pathological response. Mod Pathol. 2021;34:1333–1344. 23. Liu X, Sun W, Wu J, et al. Major pathologic response assessment and clinical significance of metastatic lymph nodes after neoadjuvant therapy for non-small cell lung cancer. Mod Pathol. 2021;34:1990–1998. 24. Cascone T, William WN Jr, Weissferdt A, et al. Neoadjuvant nivolumab or nivolumab plus ipilimumab in operable non-small cell lung cancer: The phase 2 randomized NEOSTAR trial. Nat Med. 2021;27:504–514. 25. Chaft JE, Oezkan F, Kris MG, et al. Neoadjuvant atezolizumab for resectable non-small cell lung cancer: An open-label, single-arm phase II trial. Nat Med. 2022;28:2155–2161. 26. Dacic S, Travis W, Redman M, et al. International association for the study of lung cancer study of reproducibility in assessment of pathologic response in resected lung cancers after neoadjuvant therapy. J Thorac Oncol. 2023;18:1290–1302. 27. Weissferdt A, Pataer A, Vaporciyan AA, et al. Agreement on major pathological response in NSCLC patients receiving neoadjuvant chemotherapy. Clin Lung Cancer. 2020;21:341–348. 28. Dacic S, Travis WD, Giltnane JM, et al. Artificial intelligence (AI)–powered pathologic response (PathR) assessment of resection specimens after neoadjuvant atezolizumab in patients with non-small cell lung cancer: Results from the LCMC3 study. J Clin Oncol. 2021;39(15_suppl):106. 29. Dacic S, Travis WD, Giltnane JM, et al. Artificial intelligence-powered assessment of pathologic response to neoadjuvant atezolizumab in patients with non-small cell lung cancer: Results from the LCMC3 study. J Thorac Oncol. 2023:S1556–0864 (23)02415-2. doi:10.1016/j.jtho.2023.12.010 30. Kerr KM, Johnson SK, King G, et al. Partial regression in primary carcinoma of the lung: Does it occur? Histopathology. 1998;33:55–63. 31. Forde PM, Chaft JE, Smith KN, et al. Neoadjuvant PD-1 blockade in resectable lung cancer. N Engl J Med. 2018;378:1976–1986. 32. Rusch VW, Giroux DJ, Kraut MJ, et al. Induction chemoradiation and surgical resection for non-small cell lung carcinomas of the superior sulcus: Initial results of Southwest Oncology Group Trial 9416 (Intergroup Trial 0160). J Thorac Cardiovasc Surg. 2001;121:472–483. 33. Rothschild SI, Zippelius A, Eboulet EI, et al. SAKK 16/14: Durvalumab in addition to neoadjuvant chemotherapy in patients with Stage IIIA(N2) Non-small-cell lung cancer-A multicenter single-arm phase II Trial. J Clin Oncol. 2021;39:2872–2880. 34. Saqi A, Leslie KO, Moreira AL, et al. Assessing pathologic response in resected lung cancers: Current standards, proposal for a novel pathologic response calculator tool, and challenges in practice. JTO Clin Res Rep. 2022;3:100310. 35. Cottrell TR, Thompson ED, Forde PM, et al. Pathologic features of response to neoadjuvant anti-PD-1 in resected non-small-cell lung carcinoma: A proposal for quantitative immune-related pathologic response criteria (irPRC). Ann Oncol. 2018;29:1853–1860. 36. Provenzano E, Bossuyt V, Viale G, et al. Standardization of pathologic evaluation and reporting of postneoadjuvant specimens in clinical trials of breast cancer: Recommendations from an international working group. Mod Pathol. 2015;28:1185–1201. 37. Provencio M, Nadal E, Insa A, et al. Neoadjuvant chemotherapy and nivolumab in resectable non-small-cell lung cancer (NADIM): An open-label, multicentre, single-arm, phase 2 trial. Lancet Oncol. 2020;21:1413–1422. 38. Provencio M, Nadal E, Gonzalez-Larriba JL, et al. Perioperative nivolumab and chemotherapy in stage III non-small-cell lung cancer. N Engl J Med. 2023;389:504–513. 39. Weissferdt A, Cheuk H, Lin H, et al. Pathologic processing of lung cancer resection specimens after neoadjuvant therapy. Modern Pathol. 2024;37:100353. 40. Pataer A, Weissferdt A, Correa AM, et al. Major pathologic response and prognostic score predict survival in patients with lung cancer receiving neoadjuvant chemotherapy. JTO Clin Res Rep. 2022;3:100420. 41. Murphy SJ, Harris FR, Kosari F, et al. Using genomics to differentiate multiple primaries from metastatic lung cancer. J Thorac Oncol. 2019;14:1567–1582. 42. Pataer A, Weissferdt A, Vaporciyan AA, et al. Evaluation of pathologic response in lymph nodes of patients with lung cancer receiving neoadjuvant chemotherapy. J Thorac Oncol. 2021;16:1289–1297. 43. Cascone T, Weissferdt A, Godoy MCB, et al. Nodal immune flare mimics nodal disease progression following neoadjuvant immune checkpoint inhibitors in non-small cell lung cancer. Nat Commun. 2021;12:5045. 44. Chida M, Inoue T, Honma K, et al. Sarcoid-like reaction mimics progression of disease after induction chemotherapy for lung cancer. Ann Thorac Surg. 2010;90:2031–2033. 45. Brierley JD, Gospodarowicz MK, Wittekind C. TNM classification of malignant tumours. John Wiley & Sons; 2017. 46. Rosner S, Reuss JE, Zahurak M, et al. Five-year clinical outcomes after neoadjuvant nivolumab in resectable non-small cell lung cancer. Clin Cancer Res. 2023;29:705–710. 47. Stein JE, Lipson EJ, Cottrell TR, et al. Pan-Tumor pathologic scoring of response to PD-(L)1 blockade. Clin Cancer Res. 2020;26:545–551. 48. Weissferdt A, Sepesi B, Pataer A, et al. Pathologic assessment following neoadjuvant immunotherapy or chemotherapy demonstrates similar patterns in non-small cell lung cancer (NSCLC). Ann Oncol. 2018;29:viii680. 49. Zens P, Bello C, Scherz A, et al. The effect of neoadjuvant therapy on PD-L1 expression and CD8+lymphocyte density in non-small cell lung cancer. Mod Pathol. 2022;35:1848–1859. 50. Rojas F, Parra ER, Wistuba II, et al. Pathological response and immune biomarker assessment in non-small-cell lung carcinoma receiving neoadjuvant immune checkpoint inhibitors. Cancers (Basel). 2022;14:2775. 51. Shen J, Sun N, Zens P, et al. Spatial metabolomics for evaluating response to neoadjuvant therapy in non-small cell lung cancer patients. Cancer Commun (Lond). 2022;42:517–535. 52. Schwarzenbach H, Hoon DS, Pantel K. Cell-free nucleic acids as biomarkers in cancer patients. Nat Rev Cancer. 2011;11:426–437. 53. Mouliere F, Chandrananda D, Piskorz AM, et al. Enhanced detection of circulating tumor DNA by fragment size analysis. Sci Transl Med. 2018;10. 54. Papadopoulos N. Pathophysiology of ctDNA release into the circulation and its characteristics: What Is important for clinical applications. Recent Results Cancer Res. 2020;215:163–180. 55. Abbosh C, Birkbak NJ, Wilson GA, et al. Phylogenetic ctDNA analysis depicts early-stage lung cancer evolution. Nature. 2017;545:446–451. 56. Melo SA, Sugimoto H, O’Connell JT, et al. Cancer exosomes perform cell-independent microRNA biogenesis and promote tumorigenesis. Cancer Cell. 2014;26:707–721. 57. Mao X, Zhang Z, Zheng X, et al. Capture-based targeted ultradeep sequencing in paired tissue and plasma samples demonstrates differential subclonal ctDNA-releasing capability in advanced lung cancer. J Thorac Oncol. 2017;12:663–672. 58. Pascual J, Attard G, Bidard FC, et al. ESMO recommendations on the use of circulating tumour DNA assays for patients with cancer: A report from the ESMO Precision Medicine Working Group. Ann Oncol. 2022;33:750–768. 59. Yue D, Liu W, Chen C, et al. Circulating tumor DNA predicts neoadjuvant immunotherapy efficacy and recurrence-free survival in surgical non-small cell lung cancer patients. Transl Lung Cancer Res. 2022;11:263–276. 60. Kris MG. Dynamic circulating tumour D
留言 (0)