Achieving complete TME in lap-SPS for mid- and low-RC is a significant oncological issue. Therefore, various strategies to achieve complete TME have been developed. Marks et al. [14] first reported favorable outcomes of cancer of the distal 3 cm of the true rectum by TATA with a hand-sewn coloanal anastomosis. Marks et al. [15, 16] then reported the usefulness of TATA in lap-SPS for rectal cancer. Kanso et al. [17] evaluated the short- and long-term outcomes of 138 patients treated with the primary perineal approach, compared with the primary abdominal approach, in ISR for low RC. The researchers concluded that a primary perineal approach could be considered the standard strategy for lap-SPS for low RC because of reduced operative time and similar short- and long-term outcomes. In addition, a randomized trial by Denost et al. [18] suggested that perineal rectal dissection was a new standard in lap-SPS for low RC since perineal rectal dissection reduced the risk of positive CRM in low RC.
In 2006, we started TARD combined with lap-SPS as a strategy to achieve complete TME in lap-SPS for RC near the anus—a procedure that mobilizes the most different portion of TME, “under direct vision,” in a down-to-up manner via the anus [7, 8]. We have been performing TaTME, using an endoscopic system, in lap-SPS for RC near the anus since January 2014. Recently, TaTME have been extensively studied worldwide. In this study, we aimed to evaluate the feasibility of transanal down-to-up dissection of the distal rectum, including TARD, to assist in achieving complete TME in lap-SPS for RC near the anus, assessing the surgical and oncological outcomes of these two procedures.
Regarding surgical outcomes, TaTME significantly reduced blood loss when compared with TARD. In contrast, using TARD to dissect the distal rectum under direct vision might be more straightforward, because the operative time of the perineal portion in TARD was shorter than that of TaTME; however, the shorter operative time of the perineal portion did not affect the total operative times of either procedure, in this study.
Second, in this study, no cases of mortality occurred; however, we experienced relatively high rates of postoperative complications, with 42.3% of patients displaying Clavien–Dindo classification grade ≥ 2 and 19.5% of patients displaying Clavien–Dindo classification grade ≥ 3. Urinary dysfunction and stoma-related complications were the most common postoperative complications, followed by anastomotic leakage. According to previous studies, the incidence of postoperative complications in the TARD group is nearly equivalent. Kanso et al. [17] reported overall morbidity and severe morbidities in ISR with a primary perineal approach in 47% and 16% of patients, respectively. Also, Denost et al. [18] reported that surgical morbidity occurred in 12% of lap-SPS cases.
In a study by Roodbeen et al. [19], postoperative complications (Clavien–Dindo classification grade ≥ 2 and ≥ 3) developed in 13 (31.7%) and 9 (22.0%) patients (out of 41 patients) with TaTME, respectively. In another study by Munini et al. [20], the frequency of Clavien–Dindo classification grade ≥ 2 was 28.9% in TaTME patients, while grade ≥ 3 classifications were absent. In contrast, Hallam et al. [21] reported more favorable outcomes: postoperative complications (Clavien–Dindo classification grades ≥ 2 and ≥ 3) occurred in 14% (10/70 patients) and 11% (8/70 patients) of patients, respectively. In a recent systematic review and meta-analysis by An et al. [22], the overall morbidity of TaTME was 30%, including leakage at 6.8%.
Colorectal surgeons are aware that urinary morbidity is an important clinical issue during down-to-up dissection of the rectum via the anus. In other studies, the rate of urinary injury has been reported to be 1–11%. Klein et al. [23] reported that, although the urinary function was preserved in 89% of 115 patients, a urethral injury occurred in one patient, while six (5%) patients required permanent urinary catheterization. In addition, Sylla et al. [24] analyzed urologic injuries in TaTME patients and reported 34 urethral, two ureteral, and three bladder injuries occurring during TaTME, performed over 7 years by 32 surgical teams.
Although none of our patients incurred urethral injury in this study, urinary dysfunction developed in 16 (13.0%) patients, including 10 (8.1%) patients who required medication for urinary dysfunction. In general, a transanal down-to-up approach to the rectum, including TARD and TaTME, is likely to injure the urethra and its associated neurovascular bundle. In particular, anterior dissection of the distal rectum is, technically, very difficult because of anatomical complexity. Attention must be paid to the neurovascular bundle located at the anterolateral side of the rectum to avoid urinary morbidity after surgery. In TARD, we performed the dissection transabdominally rather than transanally, for the anterolateral side of the rectum, where the neurovascular bundle was located. In contrast, taking advantage of good vision under endoscopy in TaTME, we could easily perform transanal dissection around the neurovascular bundle. For these reasons, urinary morbidity might have occurred more frequently in the TaTME group than in the TARD group. In addition, 10.0% (5 patients) of patients in the TARD group required medication for urinary dysfunction. This was thought to be due to blind dissection at the rectum’s anterior side under direct vision.
Leakage is a critical issue in transanal down-to-up rectal dissection procedures. Previous studies have reported an anastomotic leakage rate of between 5.5 and 17.9% [19,20,21,22,23, 25].
The international TaTME registry reports a morbidity rate of 35.4%, including an anastomotic failure rate of 15.7%, a pelvic abscess rate of 4.7%, an anastomotic fistula rate of 0.8%, a chronic sinus rate of 0.9%, and an anastomotic stricture rate of 3.6%. The registry also reported that male sex, obesity, smoking, diabetes mellitus, tumors >25 mm, excessive intraoperative blood loss, manual anastomosis, and prolonged perineal operative time were independent risk factors for anastomotic failure [26].
In this study, anastomotic leakage occurred in 8.9% of patients, including one who required reoperation because of ischemia at the anastomotic site [27]. However, for other patients with leakage, we could only treat the patients conservatively, with interventional radiological drainage. This might be because diverting ileostomas were created in all patients. In addition, in this study, stoma-related complications occurred more frequently than expected, where most patients had outlet obstruction and/or a high-output stoma. Stoma-related complications could be associated with the fact that we created a stoma at the ileum and not at the transverse colon for all patients.
Third, focusing on oncological outcomes is also important to clarify the feasibility of down-to-up dissection for RC. In particular, local recurrence is of great concern. We achieved complete or nearly complete TME in all patients. In addition, we obtained safe surgical margins, including the CRM and DMs in both groups. Jiang et al. conducted a systematic review and meta-analysis [28], showing that TaTME had more positive CRM and DM advantages than laparoscopic TME. We believe that transanal down-to-up dissections have some benefits. First, we could convert the procedure to rectal amputation whenever any direct invasion of the adjacent organs (such as the vagina, prostate, and seminal vesicles) was suspected during mobilization of the distal rectum [29]. Second, with down-to-up dissections under direct vision, we could obtain an adequate distant margin from the end of the tumor. For patients who needed ISR to preserve the anus for RC near the anus, we obtained an adequate distance from the end of the RC. For five patients in whom the tumor was suspected of invading the external sphincter muscle or the adjacent organs (such as the prostate and vagina), we could choose an adequate surgery for rectal amputation from an oncological perspective.
In this study, recurrence developed in 14.6% (18/123) of patients. Although no significant difference in recurrent organs was found between the two groups, we observed a high recurrence rate of 32.3% even in pStage III, compared with 7.7% in pStage I and 9.1% in pStage II. Metastasis to the lungs and local recurrence, including the pelvis lymph nodes, was frequent. Wasmuth et al. [30] reported a high local recurrence rate of 7.6% (12/157 patients) at a median follow-up of 20 months, including eight unexpected patterns of multifocal or extensive local recurrences, resulting in the abandonment of TaTME in Norway. van Oostendorp et al. [31] reported the short-term outcomes of 120 patients with TaTME performed at 12 centers. The overall local recurrence rate was 10%, with a mean interval to recurrence of 15.2 months. Multifocal local recurrence was present in eight of 12 patients. In a prolonged cohort (266 patients), overall multifocal local recurrence rate was 5–6%. The researchers stated that multifocal local recurrence may be closely associated with suboptimal TaTME execution. In both studies, most local recurrences were multifocal or extensive. Our study did not encounter the same degree of multifocal or extensive local recurrence reported in the literature.
In a prospective multicenter study in Denmark [2], the dissection plane was mesorectal in 60% of the cases, intra-mesorectal in 28%, and muscular in 12%. Non-micro-radicality was observed in 8% of cases, although microscopic and macroscopic residual tumors were observed in 6% and 2%, respectively. Although the local recurrence rate was 3.5% (4/115 patients), one patient had multifocal recurrence at a median follow-up of 23 months. A systematic meta-analysis review by Jiang et al. [28], examining pathological outcomes of transanal versus laparoscopic TME for RC, reported that TaTME had better outcomes for positive CRM than laparoscopic TME. However, Caycedo-Marulanda et al. [32] reported that a positive CRM increased the risk of local recurrence 4.2 times more than a negative CRM. Local recurrence is likely closely associated with positive CRM. Therefore, we emphasize cognizance regarding the development of multifocal or extensive local recurrence in a transanal down-to-up dissection of the rectum, which could be closely associated with a positive CRM. Preoperative treatment is important for patients with locally advanced RC.
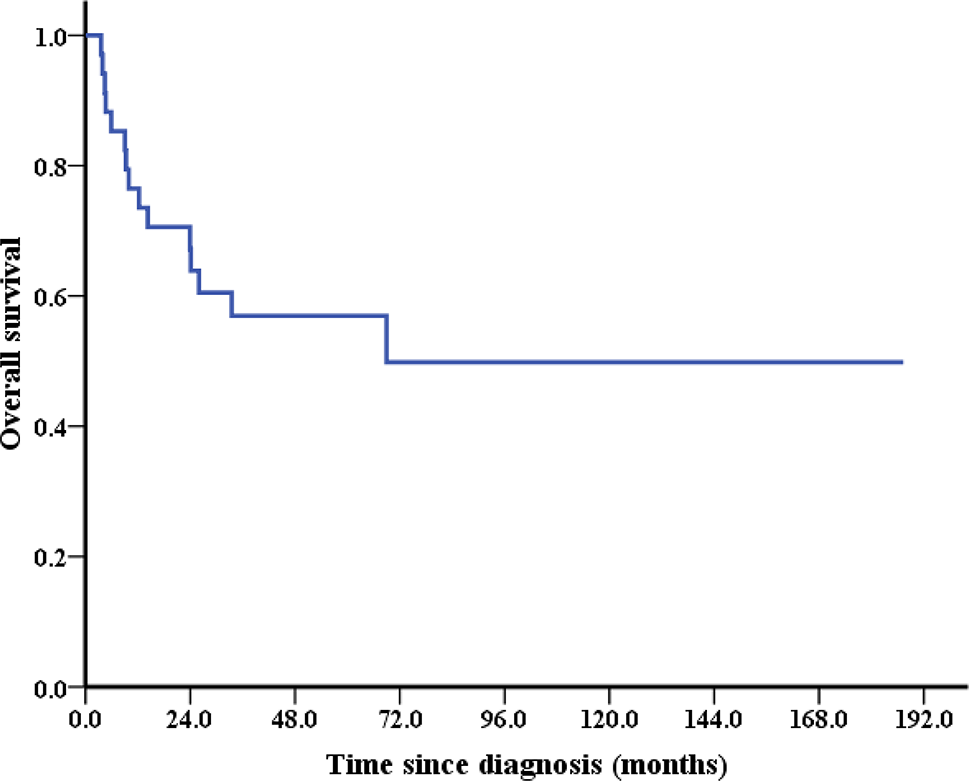
Finally, this study found a favorable survival rate, with a 5-year OS rate of 95.8% and a 5-year RFS rate of 88.8%. In comparing the two groups, the 5-year OS and RFS were comparable.
Marks et al. [16] reported a 5-year OS rate of 90% (regarding long-term outcomes) after a transanal approach to TME for RC. In addition, Denost et al. [33] reported that the 5-year OS and DFS rates of transanal low rectal dissection were 87.0% and 72%, respectively. Recently, we found studies evaluating the long-term outcomes of TaTME. Hol et al. [34] reported that the 5-year DFS and OS rates in 159 consecutive patients with TaTME were 81% and 77.3%, respectively. In addition, Ourô et al. [35] reported that the 5-year DFS and OS rates in 44 patients with TaTME were 87.0% and 81%, respectively.
Recent meta-analyses [36,37,38,39,40,41] suggest that transanal down-to-up dissection procedures, including TARD and TaTME, might be acceptable in lap-SPS for mid-and low-RC. However, we currently reason that oncological safety in a transanal down-to-up dissection for RC is still controversial. We must wait for the results of the COLOR III [42] and ETAP-GRECCAR 11 TRIAL [43] studies to further evaluate the efficacy and safety of TaTME.
This study had some limitations. First, this study was conducted at a single institution in Japan, and the data were retrospectively analyzed using a small sample size. As a transanal down-to-up dissection of the distal rectum to achieve complete TME is considered a difficult technique even for colorectal surgeons, the quality of the techniques could improve with increasing surgical experience. These experiences might affect surgical and oncological outcomes. However, we could not evaluate the outcomes of 123 patients, especially for the TARD group, in which only 50 patients could be evaluated in this study. The small sample size of the TARD group may cause some bias in surgical and oncological outcomes. Second, this study used a one-team approach for all patients. If two teams had performed the surgery, we might have reduced both operative time and blood loss because of improved visualization of the anterior side of the distal rectum. Third, we were not able to evaluate the accurate distance between the anal verge and the tumor by reviewing the medical and operative records. Finally, we should have evaluated functional outcomes following surgery to assess further the efficacy and safety of the procedures we performed.






留言 (0)