
記住我
A 56-year-old man, a never smoker, presented to the emergency department with a 3-day history of right-sided chest pain—treated outside with analgesics—and he developed gradual-onset swelling of face, neck, chest and abdomen for 1 day. He also had a history of productive cough and fever in the past month; there was no history of bouts of vomiting, recent trauma, surgery or any lung diseases. Examination revealed crepitus suggestive of subcutaneous emphysema. Chest X-ray shows (figure 1A–E) right pneumothorax with bilateral extensive subcutaneous emphysema extending from neck to abdomen.
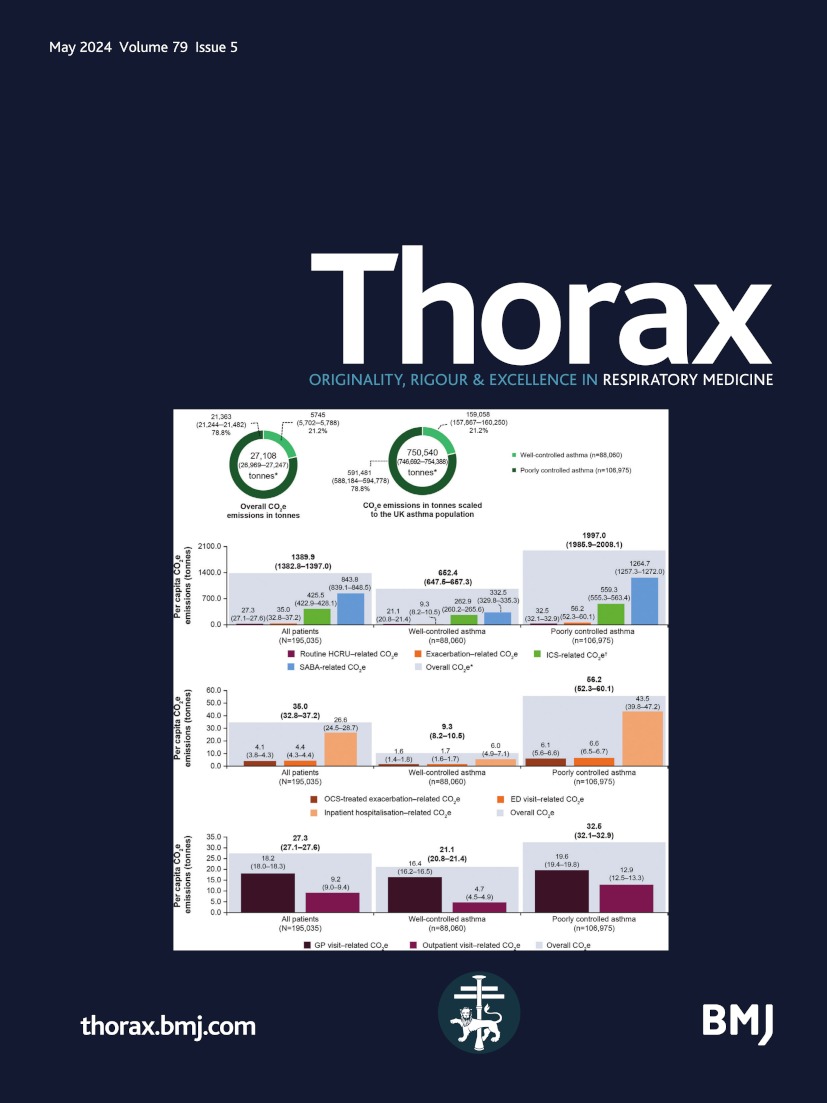
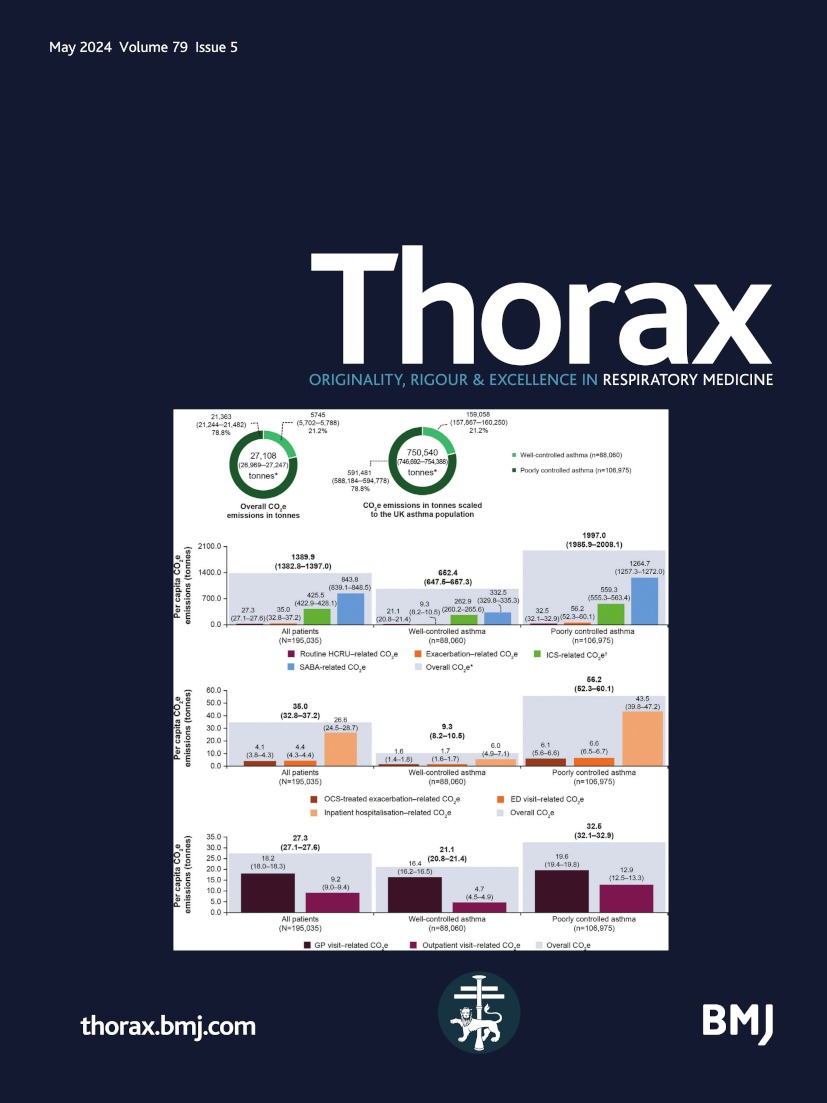
 Figure 1
Figure 1 (A) Frontal chest radiograph demonstrates right-sided pneumothorax (thin white arrow), streaks of air in the mediastinum suggestive of pneumomediastinum (thin black arrow) and extensive subcutaneous emphysema in the chest wall and neck (thick white arrow). (B) Lateral radiograph of the neck also demonstrates subcutaneous emphysema (thick white arrow). Axial (C) and coronal (D) sections of contrast-enhanced CT thorax in lung window confirms pneumomediastinum (thin black arrow), pneumothorax (asterisk) and subcutaneous emphysema. Coronal sections of contrast-enhanced CT thorax in lung window (E) and mediastinal window (F) demonstrate thick-walled cavity with surrounding consolidation in right upper lobe (double arrows).Tip of the intercostal drainage tube also noted within the superior aspect of right-sided pneumothorax.
He underwent an emergency chest tube insertion and was given high-flow oxygen; CT thorax (figure 1F) showed areas of consolidation and cavities in the right lung (double arrows) and concurrently his sputum examination revealed Mycobacterium tuberculosis.
Pulmonary tuberculosis is a rare cause of spontaneous pneumomediastinum.1 The cause is usually a cavity rupturing into the pleural space and the formation of a bronchopleurocutaneous fistula. Primary spontaneous pneumomediastinum is usually seen in smokers or following bouts of retching or vomiting.
Chest X-ray is done in most cases but diagnosis is made only in 30%; a contrast-enhanced CT thorax helps to delineate other causes.2 These are post-trauma or postoesophagoscopy which are dealt with more commonly.2 In suspected cases of oesophageal rupture an oral contrast or oesophagoscopy may be needed.3 Recently many cases have been described in patients with COVID-19 and post COVID-19; our case was prior to the pandemic and hence did not undergo testing.4
In mild cases, spontaneous resolution is the rule; no specific treatment is required and hence antibiotics, tube thoracostomy and surgery are usually deferred.2 But in our case there was pneumothorax and active infection as well.
Hence he was given antituberculous therapy, and chest tube drainage and high flow oxygen were continued, with which he gradually improved and was discharged. On telephonic follow-up he had completely recovered but could not travel due to the COVID-19 pandemic restrictions.
Ethics statementsPatient consent for publication
留言 (0)