
記住我



Data for the current study are secondary outcomes from a RCT where adolescents were randomized to 10-week GCBT interventions (brief- or standard- length CBT) or 10-week delayed-access WL. Following WL, participants were randomized to brief- or standard-length CBT. For further details, see study protocol [21]. Results from the primary outcome measures from this trial have been published elsewhere [19].
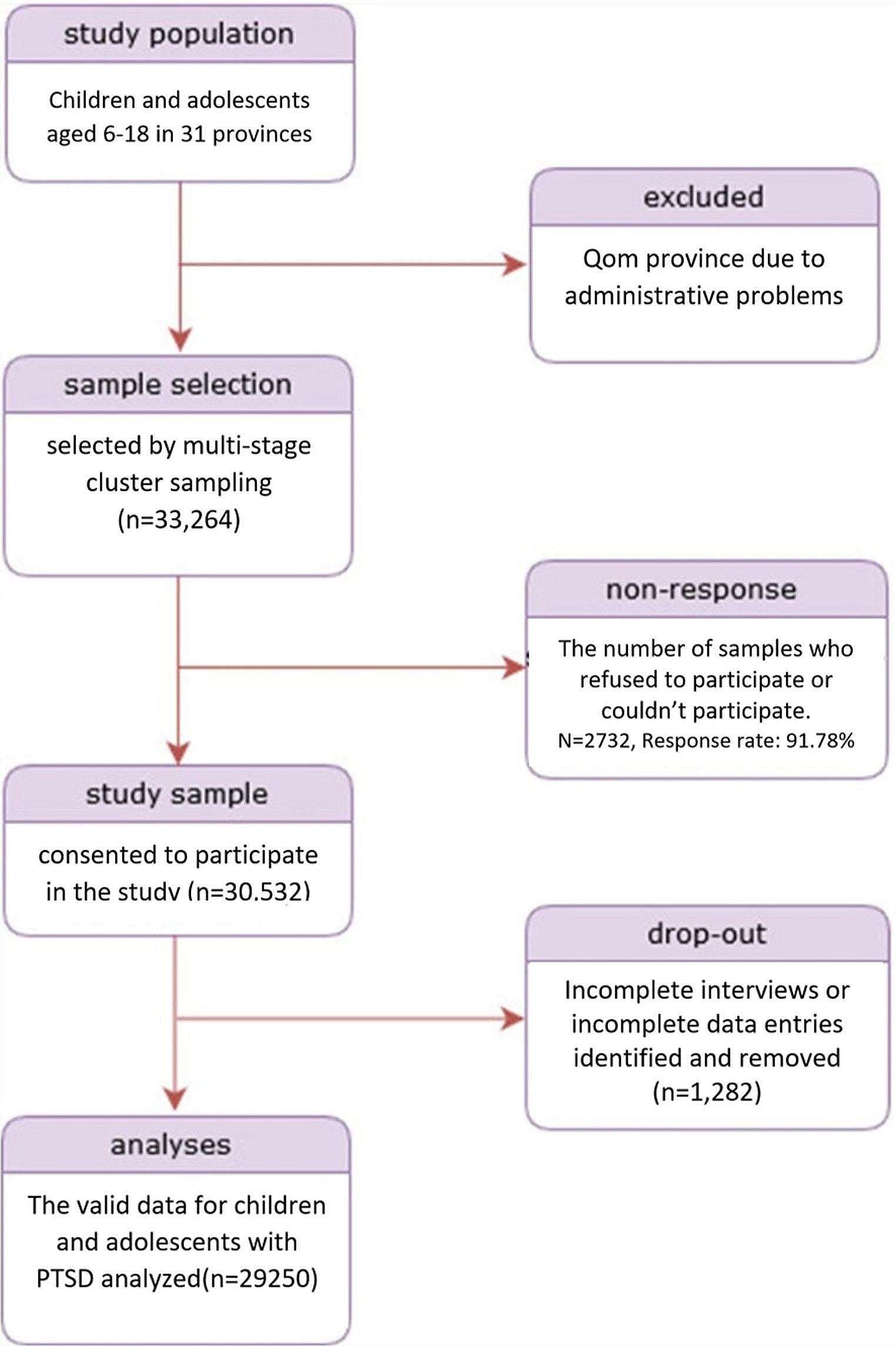
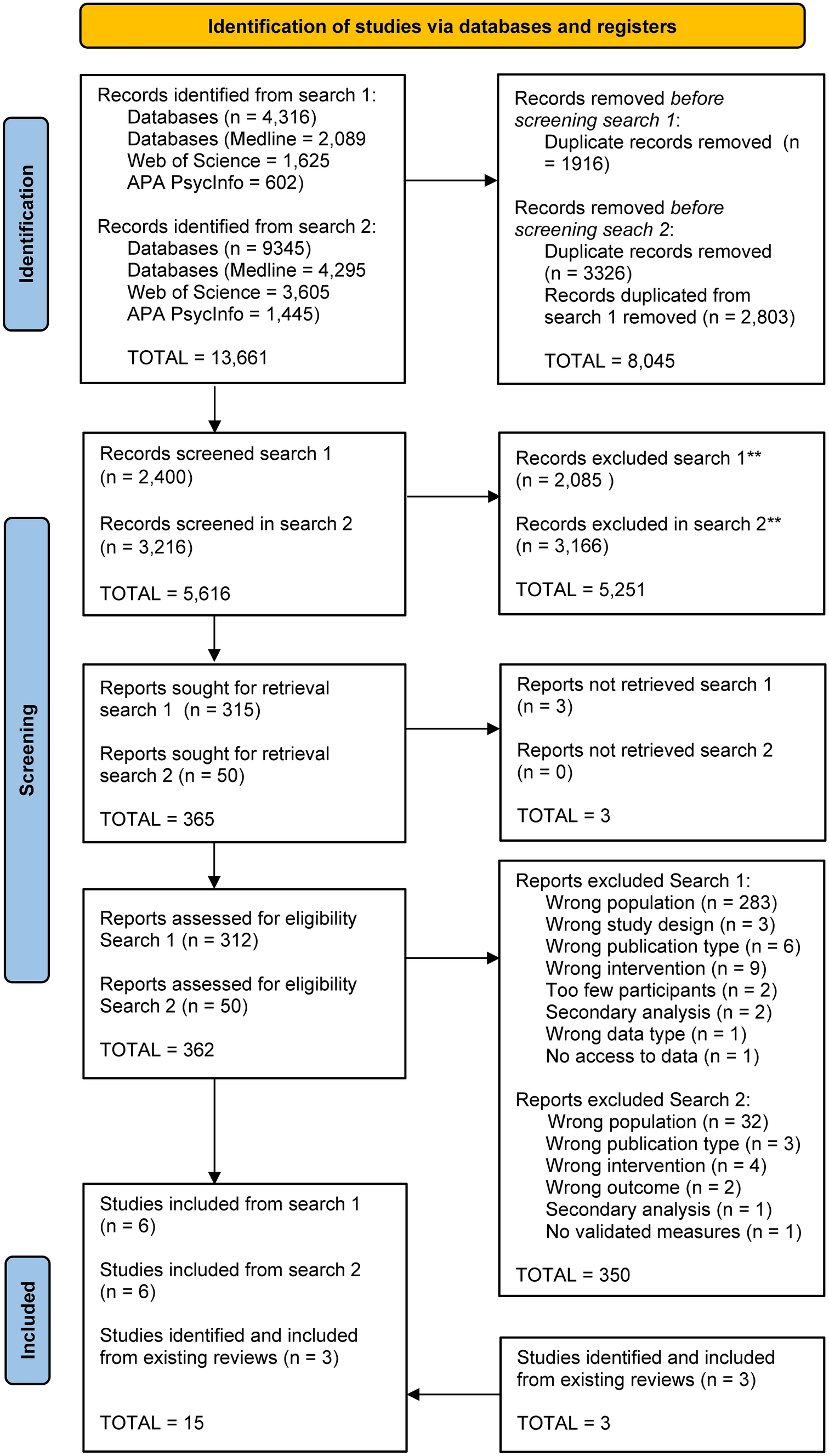
ParticipantsA total of 363 adolescents aged 12–16 years from 18 junior high schools (17 public and 1 private school) were referred for assessment. The schools represented both rural and urban areas. Participants were recruited between October 2014 and November 2016. Inclusion criteria were self-reported or parent-reported youth anxiety symptoms (i.e., ≥ 25 on the Spence Children’s Anxiety Scale; SCAS) [42], and a minimum level of interference from anxiety in daily life (i.e., a score of ≥ 1 on the first question on the Child Anxiety Life Interference Scale; CALIS) [30]. Exclusion criteria were (a) problems following group-rules, (b) disruptive behavior, and/or (c) learning problems causing difficulties following a manualized group-program. Whereas fulfillment of inclusion criteria was determined from adolescents’ and caregivers’ scores on SCAS and CALIS, a semi-structured interview developed for the RCT was administered by the providers of the GCBT and gave ground for exclusion. This was a conjoint interview with the adolescent and his/her caregiver(s), assessing the adolescent’s anxiety symptoms, anxious thoughts, avoidance, and his/her goals for the treatment. In addition, adolescents and caregivers were asked whether any of the exclusion criteria might apply. The adolescent’s teacher was consulted to give his/her appraisal of the adolescent, based on observations from the classroom (i.e., the ability to follow group-rules, disruptive behavior, and/or presence of major learning problems). Thus, exclusion was based on information from the adolescents, caregivers, and teachers. A final decision was made in discussion with the principal investigator of the study. Three adolescents were excluded, 34 did not meet inclusion criteria, seven declined to participate, and six were not included as some schools did not manage to recruit enough adolescents to form a group before the semester ended. The final sample comprised 313 adolescents (mean age 14.0 years, SD = 0.84, 84.0% girls). See Fig. 1 for the study flow-chart and Table 1 for sample characteristics.
Fig. 1
CONSORT Flow diagram reproduced from Haugland et al., 2020
Table 1 Baseline demographic and clinical characteristics of participants in group cognitive-behavioral interventions (GCBT) compared to waitlist, and brief GCBT compared to standard-length GCBTThe study was approved by the Regional Committees for Medical and Health Research Ethics in Norway (Approval No 2013/2331).
Recruitment and randomizationParticipants were recruited through multiple formats (e.g., routine student and parent meetings with school nurses, nomination by teachers, and information through media, school, and classroom meetings). Information about the study was also given to those adolescents scoring above mean on a school survey concerning anxiety symptoms. Both self-referral and referral from others were endorsed.
Adolescents and at least one caregiver met with the providers of the GCBT interventions to assess eligibility. Informed written consent/assent was obtained from caregivers and adolescents, followed by baseline assessments and evaluation of inclusion and exclusion criteria.
At each school, sequences of five to eight adolescents were randomly assigned to brief GCBT (n = 91), standard-length GCBT (n = 118), or WL (n = 104). The randomization procedure was determined prior to inclusion and according to a computer-generated random-digit procedure, with groups randomized to all three conditions at each school. A total of 52 intervention-groups were completed (including adolescents re-randomized to brief or standard-length GCBT after WL), comprising 142 adolescents allocated to brief GCBT and 160 adolescents allocated to standard-length GCBT.
A subgroup of adolescents received other treatments for anxiety (i.e., medication, or specialized mental health community services at least once a month) during the interventions (9.9%), WL (6.7%), or the 1-year follow-up (18.5%). A small number received anxiety-medication (SSRIs) pre-treatment (n = 4), during the intervention (n = 2), or during the 1-year follow-up (n = 3).
Providers and interventionsThe GCBT sessions were held at schools, during school hours. Each group was conducted by two providers, comprising mainly school-nurses (n = 21), mental health workers from community services (community psychologists n = 5, family therapist n = 1), or employees from local CAMHS (n = 5, e.g., social workers). All providers participated as part of their regular job. The providers were 93.8% women (mean age = 43.2, SD = 8.09, range 32–62), most (83.9%) having no prior CBT training. Each provider administered 1–8 groups (mean = 3.3 groups; SD = 1.8), with 75.0% administering both interventions.
The standard-length 10 session program (plus two parents-only sessions) was Cool Kids (CK), a CBT program for youth anxiety. The adolescent group-based, school-version was applied [38]. Adolescents attended weekly 90-min sessions. The program comprises workbooks for adolescents and parents.
The brief 5 session program was Vaag [37], a group-based CBT program comprising weekly sessions of 45–90 min over four weeks, followed by a final session five weeks later. Session two was a joint youth-parent session.
Both programs include basic CBT-interventions for anxiety, e.g., cognitive restructuring, exposure tasks, and homework. None of the programs cover sleep hygiene or sleep interventions. See study protocol [21] for further details on structure and content of the interventions.
Training, supervision, and treatment integrityThe GCBT providers received one four-day skills-training workshop focusing on basic CBT-principles for anxiety, programs, and assessment procedures. During the period when the providers administered the interventions, they attended two additional two-day workshops.
Supervision was given by experienced CBT-therapists (N = 10) and primarily administered face-to-face. For practical reasons (e.g., geographical distance, weather conditions, a tight time schedule), exceptions could be made, with some supervision sessions delivered digitally or by phone instead of face-to-face. All sessions were videotaped, and these video-recordings were available for the supervisors prior to and during supervision.
Independent raters scored treatment integrity, rating two of the video-taped sessions from each of the 52 groups. Ratings were done by clinical experts, applying the Competence and Adherence Scale for Cognitive Behavioral Therapy (CAS–CBT) [7], covering scorings of adherence to the program (0 = none, 6 = thorough) and competence (0 = poor skills, 6 = excellent skills). Adherence and competence scores for each group (mean of the two rated sessions) ranged from 3.17 to 5.75 (mean = 4.41, SD = 0.56) for adherence and 2.75 to 5.88 (mean = 4.18, SD = 0.66). Thus, high adherence and good competence were achieved [19].
InstrumentsAll measures were administered electronically. Sleep characteristics, and anxiety- and depressive symptoms, were assessed pre- and post-interventions, post-WL, and 1-year after the interventions. Sleep outcomes comprised insomnia, sleep onset latency (SOL), and sleep duration, all previously applied in population-based studies [22, 40]. As sleep outcomes were reported by adolescents only, we applied only adolescents’ self-reported anxiety and depressive symptoms in the current study.
Demographic informationAdolescents reported their sex, age, and their own and their caregivers’ country of birth. Social class was determined by occupation of the highest-ranking parent (reported by caregivers and adolescents) according to the Registrar General Social Class coding scheme and categorized as high, medium, and low [27]. Family structure was rated from the question “with whom do you live”, with six possible response alternatives, later categorized as two-parent or single-parent families.
Sleep outcomesInsomnia was operationalized according to DSM-5 criteria [22]. The following three criteria were used as an operationalization for insomnia disorder, in line with the DSM-5 criteria: (a) the presence of either difficulty in initiating or maintaining sleep for at least three nights per week; (b) the presence of daytime sleepiness and tiredness for at least three days per week; and (c) duration of the sleep problems for at least three months. A similar definition has been used in other studies, (e.g., [22, 41]). More specifically, insomnia comprised a positive response (“somewhat true” or “certainly true”) to Difficulties initiating and maintaining sleep (DIMS) and a positive response (“somewhat true” or “certainly true”) to a joint sleepiness and/or tiredness. Further, insomnia required a DIMS frequency of at least three days per week and a duration of at least three months. The DIMS was rated on a three-point Likert-scale with response options “not true”, “somewhat true” and “certainly true”. Given a positive response (“somewhat true” or “certainly true”), the participants were asked how many days per week they experienced difficulties initiating and maintaining sleep and how long this had been a problem. Tiredness/sleepiness was rated by a joint question on a three-point Likert-scale with response options “not true”, “somewhat true” and “certainly true”. If confirmed (“somewhat true” or “certainly true”), adolescents reported the number of days per week they experienced sleepiness and tiredness, respectively.
The adolescents indicated when they usually went to bed at night and their usual rise time in the morning on weekdays and weekends. Time in bed (TIB) was calculated by subtracting bedtime from rise-time.
Sleep onset latency (SOL) i.e., how long it usually took to fall asleep, was reported in hours and minutes, and further categorized into five levels (from a score of 1 = less than 15 min to 5 = 120 min or more).
Sleep duration was calculated separately for weekday and weekend nights and defined as TIB minus SOL. Weekday nights were selected for further analyses. Sleep duration was categorized into ten levels (from a score of 1 = less than 4 h to 10 = 12 h or more).
Anxiety and depressive symptomsAnxiety symptoms were assessed by the Spence Children’s Anxiety Scale (SCAS) [33, 42] comprising 44 items, including six positive filler items. SCAS is scored on a 4-point scale, rated from 0 (never) to 3 (always). SCAS has demonstrated sound psychometric properties [3, 33]. Good to excellent internal consistency was found in the current study, applying Cronbach’s alpha (α = 0.91).
Responders to GCBTClinical Global Impression–Improvement (CGI–I) [18], was used to assess change in clinical symptoms. In this study CGI–I focused specifically on the adolescents’ anxiety symptoms and impairment from anxiety. CGI–I ranges from 1 (very much improved) to 7 (very much worse). The CGI–I was scored by providers of the GCBT, based on a joint parent-youth interview (15–30 min) administered pre- and post-intervention/post-WL. Consistent with previous research [35], adolescents who received a CGI–I score of 1 (very much improved) or 2 (much improved) were considered as responders to GCBT, whereas youth with a CGI–I score ≥ 3 (from minimally improved to very much worse) were defined as non-responders. Three expert scorers, blinded to the original CGI–I scores, rated 20% of the scores based on videotapes of the assessment interviews, with an average agreement between expert scorers and providers of [ICC] (2.1) = 0.81.
Data analysisPower calculation for the RCT was performed for the primary outcome measures (i.e., anxiety symptoms), where we aimed to obtain a small to moderate effect size (d = 0.40) between the GCBT and WL condition. With an assumed attrition of 10%, a recruitment goal of 323 participants was established [21].
Demographic characteristics, anxiety- and depressive symptoms, and sleep characteristics are presented with mean, standard deviation (SD), numbers and percentages (Table 1). Differences between conditions (GCBT versus WL, and brief versus standard GCBT) pre-intervention were analyzed by t tests (continuous variables) and chi-square tests (categorical variables). The same was applied in analyses of potential pre-intervention differences between responders and non-responders.
Logistic mixed-effects models (insomnia) and linear mixed effect models (SOL and sleep duration) (LMMs) were used to analyze possible differences in the change in sleep outcomes between timepoints. To account for dependency within schools and intervention-groups, these were used as random intercepts in addition to individuals in all analyses.
To investigate changes in sleep outcomes across time for all participants (pre- to post-intervention/post WL, and one-year follow-up) a model including time as the fixed effect was provided.
To test differences regarding change in sleep outcomes between GCBT and WL, a model including condition (GCBT/WL), time (pre- to post-interaction / post-WL) and an interaction term between condition and time as fixed effects were provided.
For analyses of differences between brief and standard-length GCBT on sleep outcomes, LMMs were conducted including intervention (brief and standard-length), time and an interaction term between intervention and time as a fixed effect. For the groups re-randomized to GCBT after WL, post-WL scores were used as pre-intervention scores. For insomnia odds ratios (OR) with 95% confidence intervals (CI) are provided, while estimated means, standard error (SE), and p-values for differences between changes in GCBT by time are given for SOL and sleep duration.
Finally, LMMs were used to analyze possible differences between adolescents defined as responders and non-responders to GCBT. Similar models were applied as above, accounting for dependencies within schools and groups as random factors in addition to individuals. Further, responders, time (pre-intervention /or post-WL and post-intervention) and an interaction term between responders and time were included as a fixed effect.
Within- and between-group effect sizes (Cohen’s d) were calculated based on estimated means from LMM analyses (unadjusted) and pooled pre-standard deviations. Analyses used the intention-to-treat sample. A significance level of p < 0.05 was applied. Missing data were examined by the missing value analysis in SPSS 25 (SPSS/IBM Statistics, Chicago, IL), and handled by a full information maximum likelihood missing data methodology (FIML) in STATA (15.1) (StataCorp, College Station, TX). Missing data originated mainly from participants lost to assessment after WL (n = 9; 8.7%), post-intervention (n = 21; 10.0%), and at 1-year follow-up (n = 100; 33.0%). Nonsignificant Little’s MCAR tests, at pre-intervention (p = 0.170), post-intervention (p = 0.761), and follow-up (p = 0.268) indicated that data on anxiety symptoms, depressive symptoms, insomnia, SOL, and sleep duration were missing completely at random.
留言 (0)