Study selection
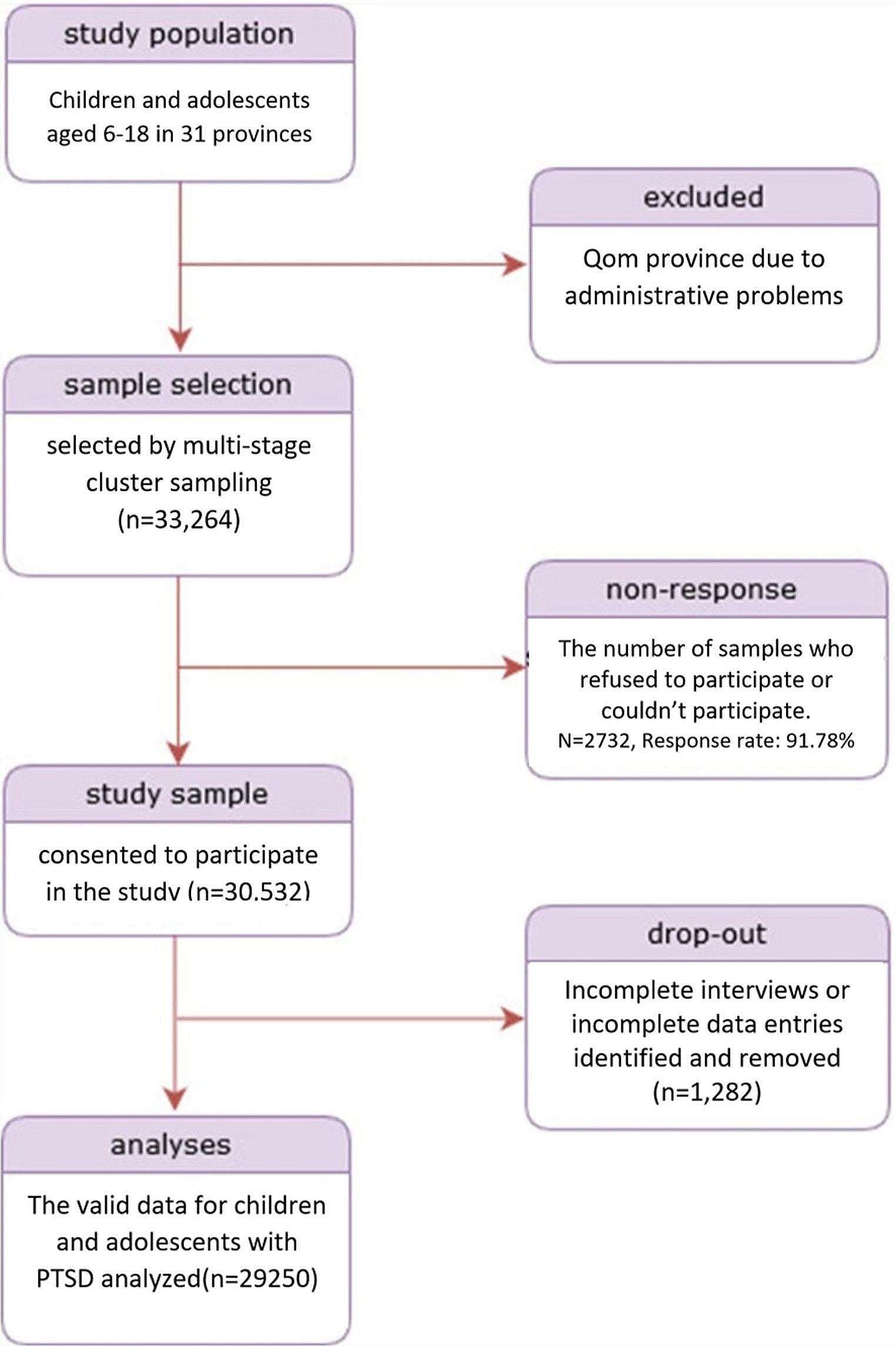
The inclusion process is illustrated in Fig. 1 and an overview of the included studies, including results, is presented in Table 1. The two searches combined resulted in 13,661 hits. Thereafter, 8045 duplicates were removed, and 5616 reports proceeded to screening. After screening abstracts, 365 studies were read in full text, after which 25 studies were considered for inclusion. A further 4 studies were identified in the reference lists or the Web of Science Citation Index of the 25 considered studies and review literature. Fourteen [53,54,55,56,57,58,59,60,61,62,63,64,65,66] of these 29 studies were later excluded (see SI 6). Thus, 15 studies [67,68,69,70,71,72,73,74,75,76,77,78,79,80,81] were included. See SI 6 for a list of all studies excluded from full text review.
Table 1 Study characteristics, intervention, implementation location, sample, N, outcomes and results, overall risk of biasStudy characteristics
Study characteristics are presented in full in SI 7. Of the 15 included studies, two were individually randomized RCTs [67, 75] ([67] = wait list control, [75] = passive control), two were cluster randomized RCTs [76, 80] ([76] = wait list control, [80] = treatment
as usual), four were non-randomized controlled trials [70, 71, 78, 79] ([70, 71, 79]= wait list control, 78 = passive control), and the remainder were uncontrolled pre-post intervention studies. None included follow-up measures. The studies were published between 2005 and 2022. Three studies investigated the effects of two interventions [67, 79, 80]. Thus, the included studies assessed a total of 18 unique interventions.
Risk of bias in individual studies
Overall risk of bias for each study is presented in Table 1. None of the included studies were assessed to have low risk of bias. Eight studies were assessed to have moderate risk of bias [67, 70, 71, 74,75,76, 79, 80] and seven were assessed to have high risk of bias [68, 69, 72, 73, 77, 78, 81]. All four RCTs were assessed to have moderate risk of bias. Some bias was expected as it is difficult to blind participants in studies of psychosocial interventions. Additionally, none of the studies had published a pre-specified data-analysis plan. Four of the non-randomized studies were assessed to have moderate risk of bias due to bias in measurement of results (i.e., inability to blind). The remainder were assessed to have high risk of bias as they had conducted no controls of baseline sample characteristics.
Participant characteristics
A comprehensive overview of participants’ (N = 5741) characteristics is presented in SI 8. Of the included studies, 12 had < 100 participants, two has 100–350, and one had > 4500 participants. Participants were aged between 6 and 18 years, and 49.59% were girls. All studies reported gender as a binary variable and one study [77] included only boys. The participants were primarily classified as refugees (included in 13 studies). However, two studies each included internally displaced youth [67, 79], asylum seekers [70, 73], and forcibly displaced youth [71, 76]. Two studies included only unaccompanied youth [73, 77] and one study explicitly included both accompanied and unaccompanied youth [75]. Other studies made references to parents and/or caretakers. Most studies reported the participants’ ethnicity/country of origin, but two [76, 78] reported only geographical area (Africa, Middle East, and Asia). In total there were 24 distinct ethnicities/countries of origin reported, the studies were carried out in 11 different territories, including 8 in high income countries. The participants had been living in their current location from 2 months up to 7 years (4 studies did not report this variable [71, 72, 75, 79]).
Primary outcomes: qualitative synthesis
Primary outcomes are presented in Table 2 and described qualitatively as only one study included validated measures of wellbeing [71], and quality of life [69], respectively. Although one study reported resilience [73] it did not use a validated measure.
Table 2 Summary of within and between group results for quality of life and wellbeing reported in individual studiesWellbeing was measured using the World Health Organisation Well-Being Index (WHO-5; [82]) by Foka et al. ([71], non-randomized controlled trial, moderate risk of bias). The intervention was a positive psychology intervention called Strengths for the Journey and consisted of six, daily 2-h group sessions for youth aged 6 to 17 (M age = 10; age matched groups were possible, 78.8% girls in intervention group, 52.6% girls in control group). The intervention was at the selected level and was developed and implemented in Greece, in transit camps for forcibly displaced people. The intervention manual is freely available at: https://www.qmul.ac.uk/sbbs/about-us/our-departments/psychology/strengths-for-the-journey-project/. The intervention was implemented in Arabic and Farsi languages by trained leaders and volunteer translators. No differences were found between the intervention and (non-randomized) control group in wellbeing scores at baseline (intervention M = 41.67, SD = 20.90; control M = 40.77, SD = 18.20; t(53) = − 0.17, p = 0.87) and scores were similar to previous established norms [82]. At post measurement, the intervention group reported significant and large increases in wellbeing compared to the control group (intervention M = 88.27, SD = 13.24; control M = 47.89, SD = 22.03; F(1,46) = 42.99, ηp2 = 0.48, p < 0.001) [71]. Sensitivity analyses were conducted to control for gender and baseline levels of self-esteem [71].
Quality of life was measured using the PedsQL Inventory-Version 4 for adolescents [83] by Doumit et al. ([69], pre-post study, assessed high risk of bias). The intervention was an existing Cognitive-Behavioural skill-building intervention called Creating Opportunities for Patient Empowerment program (COPE, [84]), and was intended to increase quality of life and promote positive mental health. The participants were 40 Syrian refugee youth (M age = 14.22, 48.4% girls) living with their families in Lebanon. The intervention was at the selected level of prevention and consisted of seven weekly hour-long sessions, implemented in a local community centre. No cultural tailoring was described, but the intervention was implemented by the study PI and Arabic speaking therapists who translated directly from the English language manual. The mean total score at pre-intervention was comparable with previously established general population means [83]. Significant improvements in total quality of life were observed from pre- to postintervention (pre M = 85.20, SD = 8.98; post M = 88.77, SD = 7.67; t(28) = 2.09, p = 0.05). However, the only subscale of the PedsQL [83] to exhibit significant improvements was the physical functioning scale.
Secondary outcomes: description of studies
The most common secondary outcomes were child-rated symptoms of depression and PTSD. Child-rated depression was reported in 11 studies, which amounted to 14 unique interventions. Of these, 3 were RCTs [67, 76, 80] (5 interventions, all with moderate risk of bias) and 8 pre-post studies (3 with moderate risk of bias [70, 71, 79] and 5 with high risk of bias [68, 69, 72, 78, 81]). Child-rated PTSD was reported in 8 studies which amounted to 9 interventions (2 RCTs with moderate risk of bias [75, 76], 6 pre-post, 3 with moderate risk of bias [70, 74, 79] and 3 with high risk of bias [68, 73, 77]). However, the interventions and outcome measures reported in the two RCTs were not considered clinically similar. For example, one [75] was a written intervention implemented for traumatic grief symptoms over 3 days, while the other [76] was a group intervention for survivors of war or conflicts implemented over 8 weeks (see Table 1 for measures and SI 9 for a description of the interventions). PTSD was also parent-rated in one pre-post study [81] (serious risk of bias). Anxiety was reported in five non-randomized studies (5 interventions, 2 with moderate risk of bias [70, 74], 3 with high risk of bias [69, 78, 81]). A composite score of behavioural and emotional difficulties (measured using the child, teacher, or parent-rated Strengths and Difficulties Questionnaire; SDQ; [85], was reported in 5 studies (1 RCT with moderate bias [76], 4 pre-post, 2 with moderate risk of bias [70, 74], 2 with high risk of bias [73, 78]) which amounted to 5 interventions. Externalizing and Internalizing symptoms were reported in one study ([76], RCT, 1 intervention, moderate risk of bias). Statistics for secondary outcomes reported in individual studies are presented in SI 10.
Results of synthesesBetween-group analysis (study aim 1)
The only outcome possible to conduct a between-group meta-analysis of was depression (secondary outcome). Depression was measured in 3 RCT studies (5 interventions), all with moderate risk of bias. Two studies were at the indicated level of prevention [






留言 (0)