
記住我
Bone-anchored hearing implants (BAHIs) are widely used for hearing rehabilitation of patients with conductive or mixed hearing loss as well as for those with single-sided deafness. There are two percutaneous solutions currently on the market: the BAHA Connect (Cochlear Bone Anchored Solutions AG, Mölnlycke, Sweden) and the Ponto (Oticon Medical AB, Askim, Sweden). BAHIs bypass the middle ear by conveying vibration, generated by an external sound processor, to the inner ear via a skin-penetrating abutment and a screw implanted in the mastoid bone (1). Survival rates of BAHI systems are high, varying from 74% to 98% (2–4). However, complications, such as inflammation of the skin around the percutaneous abutment, pain, and even implant loss, have been reported (2,5).
In the center where we work, transcutaneous solutions are our first choice because they avoid such complications (6–8), although, sometimes, two-stage surgery is needed in patients who have previously undergone radical modified surgery (9,10). However, there is another group of patients with severe-to-profound and mixed hearing loss whose requirements extend beyond transcutaneous solutions. Perhaps, because of resistant chronic otitis, a complex surgical history, or congenital malformation of the ear, use of conventional hearing aids is not possible. Bone conduction hearing aids also have limited applicability when the audiologic indications are poor (11). At this point, there is a need for an alternative percutaneous solution that has a wider indication range and which can compensate for hearing loss involving bone conduction thresholds of up to 65 dB.
The Ponto BAHI is a relatively new solution (compared with BAHAs) and was introduced on the market in 2009 (12). Since then, effectiveness of the Ponto has been reported in terms of audiologic and self-report outcomes, intraoperative and postoperative adverse events, comparison of various models of implant and sound processor, and different surgical techniques (2,13–18). However, in the latest systematic literature review, Lagerkvist et al. (19) say that the effectiveness of Ponto in patients with severe-to-profound and mixed hearing loss (with bone conduction thresholds greater than 45 dB HL) has not been fully assessed.
This study, therefore, aims to investigate the audiologic effectiveness of the Ponto system in such patients. Because hearing loss has psychosocial consequences and can cause constant emotional tension that cannot be predicted from audiometric data alone, a second aim of this study was to assess the change in hearing and quality of life from the patient's perspective.
MATERIALS AND METHODS Patients and Study DesignA database consisting of medical records of patients who had undergone a Ponto implantation between July 2015 and September 2020 in our tertiary referral ENT center was carefully examined. The eligibility criteria were as follows:
age, ≥18 years; preoperative severe-to-profound hearing impairment according to the Bureau International d'Audiophonologie recommendations (20); preoperative bone thresholds average (at frequencies: 0.5, 1, 2, and 4 kHz) ≥ 45 dB HL; a minimum of 12 months follow-up.The analysis of each patient's treatment and audiologic outcomes was based on full medical documentation. This study was conducted in accordance with the ethical standards of the institutional review board and conformed with the Helsinki Declaration. Because of the retrospective nature of the study, no specific informed consent was obtained from the participants.
Audiometric TestingHearing thresholds for air conduction (AC) and bone conduction (BC) were assessed on all patients three times: before surgery and at 1 and 12 months after sound processor activation. The pure tone average (PTA4) for AC and BC was determined at 0.5, 1, 2, and 4 kHz.
The free-field hearing thresholds, word recognition score (WRS), and speech reception threshold (SRT) in noise were assessed before surgery and 6 and 12 months afterwards. All tests were performed in free-field under unaided and aided condition (i.e., without and with the processor). A loudspeaker was positioned 1 m in front of the subject (S0 azimuth). During the free-field hearing thresholds and WRS tests, the contralateral side was plugged and additionally covered with an over-the-ear phone or masked with 70 dB narrowband noise (if the interaural difference for PTA4 for AC was over 30 dB). For the matrix test, only double blocks of the nonoperated ear were used.
The free-field hearing thresholds were assessed at 0.5, 1, 2, and 4 kHz. The effective gain was evaluated 12 months after surgery and calculated as the difference between the PTA4 for BC and the average free-field hearing threshold in the aided condition.
WRS was assessed with the Demenko & Pruszewicz Polish Monosyllabic Word Test performed under unaided and aided configurations in quiet at 50, 65, and 80 dB SPL.
SRT in noise were assessed using the Polish Matrix Sentence Test (21) with signal and noise presented from the front (S0N0). The noise level was fixed at 65 dB SPL and the signal level was changed adaptively. The maximum value of SRT was 15.5 dB (i.e., the point at which there was lack of understanding of speech in noise).
Self-Report QuestionnaireSelf-reported patient outcomes were collected using the Clinical Global Impression Scale (CGI-S) (22), the Glasgow Benefit Inventory (GBI) (23), and the Abbreviated Profile of Hearing Aid Benefit (APHAB) (24).
The CGI-S is a short tool used to assess change in a patient's condition. In our study, patients were asked to assess the change in their hearing and the change in their general quality of life 12 months after Ponto sound processor activation in comparison with the state before surgery. The answers consisted of a seven-point scale with the degrees: 1, very much improved; 2, much improved; 3, minimally improved; 4, no change; 5, minimally worse; 6, much worse; 7, very much worse.
The GBI is an instrument to measure patient benefit developed especially for otorhinolaryngologic interventions. The questionnaire consists of 18 items on a five-point Likert scale, which address change in health status after an intervention. The responses range from −100 (maximum negative benefit) to 0 (no benefit) to +100 (maximum benefit). The GBI was filled in once, 12 months after activation of the sound processor.
The APHAB is the most widely used hearing-specific questionnaire among Polish audiology patients. APHAB comprises 24 items divided into four subscales: ease of communication (EC), background noise (BN), reverberation (RV), and aversiveness (AV). The first three subscales (EC, RV, and BN) address speech understanding in various everyday environments, while AV quantifies negative reactions to environmental sounds. APHAB was filled in before implantation and 12 months after sound processor activation. The change in hearing was calculated by subtracting the postoperative result from the preoperative result.
SurgeryAll surgical procedures were performed by two senior surgeons. In all cases, a wide Ponto implant, diameter of 4.5 mm and length of 4 mm, was placed in a one-stage surgical procedure under general anesthesia.
Over the last 5 years, different surgical techniques for inserting implants in the temporal bone have been used in our center. For the first five patients operated in 2015, a linear incision technique with peri-implant soft-tissue reduction (skin thinning) was performed as originally described by de Wolf et al. (25). In these patients, a 6-mm abutment length was used. For the next nine patients, a Minimally Invasive Ponto Surgery (MIPS) technique (Oticon Medical, Somerset, NJ) involving a surgical punch technique (4-mm punch) described in previous articles (16,18,26) was used. For these cases, the abutment length was 9 mm. In two patients, a linear incision without soft tissue thinning (first described by Hultcrantz et al. (27)) was done and a 9-mm abutment was used. The reason for perforation was bleeding after the first step of the MIPS technique—punch puncture of the skin and subcutaneous tissue. In such cases, coagulation might impair wound healing, and there was a need to stop bleeding from the emissary vein. Punch puncture was performed with a superior and inferior cut. Bleeding was secured and a drill was used to prepare a place for screws. It was important to assess the subcutaneous tissue and adjust abutment length accordingly (6, 9, or 12 mm).
Dressing removal was 10 days after surgery. Skin reaction around the implant was assessed for all patients postsurgery according to the Holgers scale (28).
All patients were fitted with an external processor (Ponto Pro Power, Ponto 3 Power, or Ponto 3 SuperPower). The sound processor was activated 6 to 8 weeks after implantation in the case of 11 patients and after 10 weeks in three patients. The other two patients had activation at 10 weeks reoperation.
Statistical AnalysisA Shapiro-Wilk test was used to test the assumption of normality. If the assumption of normality was met, paired-sample t tests were conducted to compare preoperative and postoperative results. To assess postoperative GBI results, a one-sample t-test was used. The level of statistical significance was set at p < 0.05. For statistical analysis, IBM SPSS Statistics v.24 software (IBM Corp, 2016, Armonk, NY) was used.
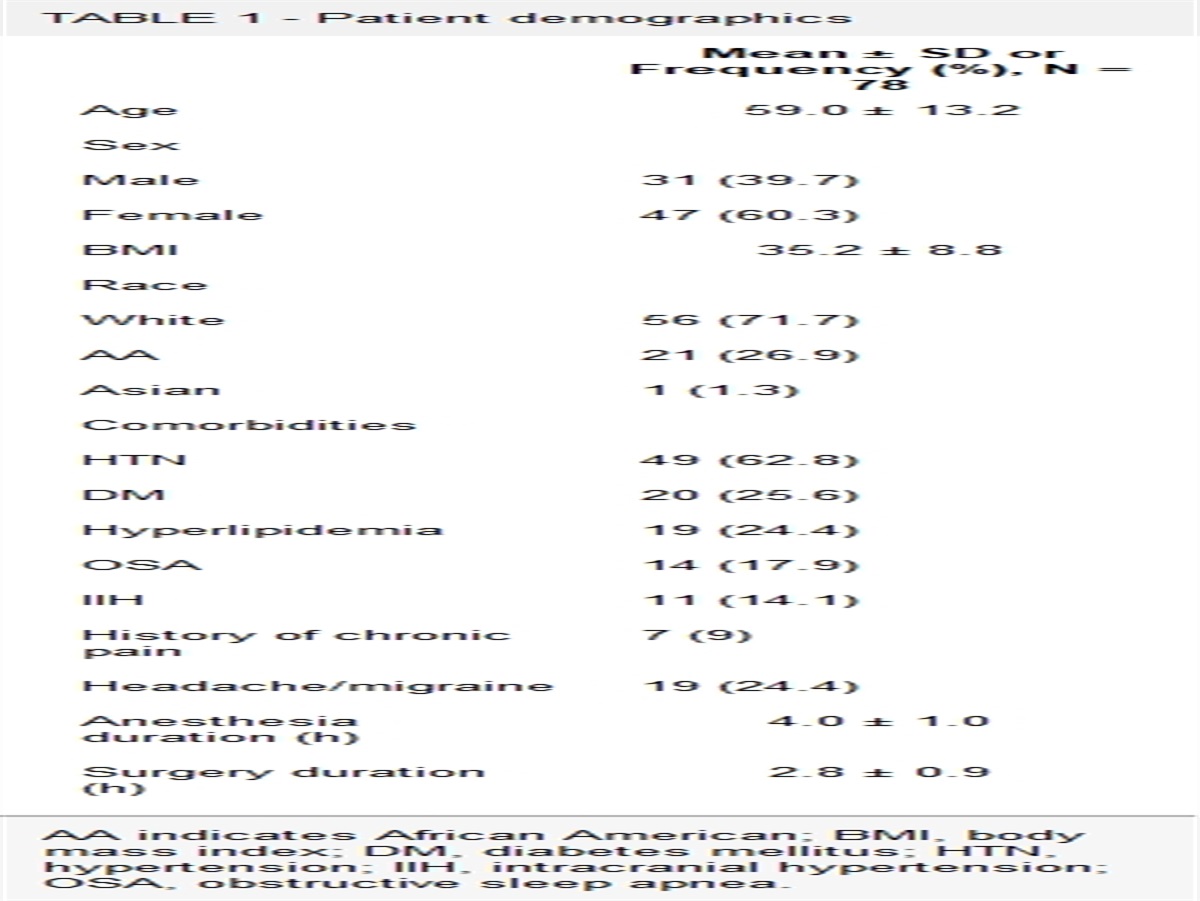
RESULTS Study Setting and Patient SelectionThere were 38 patients who underwent Ponto implantation during the study period. Of these, 18 met the inclusion criteria. Two patients who were lost from follow-up were excluded. The final study group included 16 patients. Patient information is summarized in Table 1.
TABLE 1 - Patient characteristics Patient Age at Implantation Sex Implant Side HL Side Cause of HL Previous Surgery (Implanted Side) HA Before Surgery Surgery Technique Abutment (mm) Processor Type 1 41 F Left Bilateral congenital malformations of the middle or outer ear; COM; cholesteatoma Radical mastoidectomy; revision after radical mastoidectomy Nonoperated ear linear incision with skin thinning 6 Ponto Pro Power 2 64 F Left Bilateral COM; cholesteatoma Myringoossiculoplasty; radical mastoidectomy; 3× revision after radical mastoidectomy No linear incision with skin thinning 6 Ponto Pro Power 3 65 M Right Bilateral COM; cholesteatoma Radical mastoidectomy; revision after radical mastoidectomy Nonoperated ear linear incision with skin thinning 6 Ponto Pro Power 4 63 F Right Bilateral COM 2× Myringoossiculoplasty Nonoperated ear linear incision with skin thinning 6 Ponto Pro Power 5 64 M Left Bilateral COM 2× Myringoossiculoplasty; antromastoidectomy No linear incision with skin thinning 6 Ponto Pro Power 6 68 M Left Bilateral COM; cholesteatoma 2× Myringoossiculoplasty; radical mastoidectomy; revision after radical mastoidectomy No MIPS 9 Ponto 3 Power 7 39 F Left Bilateral congenital defect outer ear (craniofacial malformation) No No MIPS 9 Ponto 3 Power 8 59 F Left Bilateral COM Antromastoidectomy; 2× tympanoplasty No MIPS 9 Ponto 3 Power 9 30 M Right Unilateral COM; cholesteatoma Radical mastoidectomy; revision after radical mastoidectomy No linear incision without skin thinning 9 Ponto 3 Power 10 60 M Left Bilateral COM 2× Myringoossiculoplasty; No MIPS 9 Ponto 3 Power 11 74 F Left Bilateral COM; cholesteatoma 3× Myringoossiculoplasty; radical mastoidectomy; revision after radical mastoidectomy Nonoperated ear linear incision without skin thinning 9 Ponto 3 SuperPower 12 54 M Right Bilateral COM; cholesteatoma Myringoossiculoplasty; radical mastoidectomy; 3× revision after radical mastoidectomy No MIPS 9 Ponto 3 SuperPower 13 21 M Right Bilateral COM 2× Myringoossiculoplasty No MIPS 9 Ponto 3 Power 14 47 F Right Bilateral COM; congenital defect middle ear; Turner syndrome 2× Myringoossiculoplasty Bilateral MIPS 9 Ponto 3 SuperPower 15 22 M Left Bilateral COM 4× Myringoossiculoplasty No MIPS 9 Ponto 3 SuperPower 16 44 F Right Bilateral COM 2× Myringoossiculoplasty No MIPS 9 Ponto 3 SuperPowerCOM indicates chronic otitis media; F, female; HA, hearing aid; HL, hearing loss; M, male; MIPS, Minimally Invasive Ponto Surgery.
Age at implantation ranged from 21 to 74 years with a mean of 50.9 years (standard deviation [SD] = 16.6 yr). In 15 patients, the hearing loss was bilateral, although all patients were implanted unilaterally. In two patients (Patients 5 and 6), the implantation procedure was performed in the better hearing ear because their BC thresholds in the poorer ear were beyond the audiologic indications for BAHIs. The etiology of hearing loss in our group of patients included chronic otitis media (COM), cholesteatoma, and congenital malformations of the middle or outer ear.
Surgical Outcomes and Adverse EventsIntraoperatively, one patient (Patient 4) had emissary vein bleeding after the periosteum was exposed, which was corrected with wax. A somewhat spongy bone was confirmed in two patients (Patients 3 and 6). There were no symptoms in preoperative diagnosis that could pose any problem, but especially in the case of those patients who had middle ear surgery (e.g., canal wall up or canal wall down), the consistency of the bone might be soft. In these patients, the sound processor was activated 10 weeks after implantation.
At dressing removal, good wound healing (Holgers Grade 0 or 1) around the abutment was found in 10 of 16 patients. In four patients (Patients 4, 6, 8, and 15), minor complications such as slight redness and moist tissue without granulation formation (Holgers Grade 2) was observed. After local treatment (and checks at extra visits), these symptoms disappeared within 6 weeks. However, one patient (Patient 8) reported slight numbness of the skin around the abutment and periodic pain that persisted throughout the postoperative follow-up period. Major complications assessed as Holgers Grade 4 were noted in two patients (Patients 7 and 11); because of persistent skin infection around the abutment and a lack of response to treatment, reoperation was required.
In Patient 7, 5 weeks after the initial surgery, inflammatory and granulation tissues were removed. At postoperative extra visits, healing was normal (Holgers Grade 0) and activation was done after 10 weeks. In Patient 11, 6 weeks after the initial surgery, the abutment (without implant) was removed and so was necrotic tissue. After 3 months, the abutment was placed and connected to the implant under local anesthesia. Four weeks later a second revision was performed involving the removal of skin overgrowth. Ten weeks later, activation was done. The patient reported periodic itching and aching skin at the abutment site lasting up to 1 year.
At the 12-month postoperative follow-up, slight redness requiring local treatment (Holgers Grade 2) was noted in three patients (Patients 5, 9, and 16) in whom no complications had previously been reported. All patients were still using the Ponto after an average observation time of 2.7 years (minimum, 1.1 yr; maximum, 4.9 yr).
Audiometry and Speech TestsPreoperative hearing thresholds for air and bone condition in the implanted and nonimplanted ear for each patient are shown in Table 2.
TABLE 2 - Preoperative hearing thresholds for air and bone condition in the implanted and nonimplanted ear Patient 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 Implanted ear AC 500 Hz 100 95 70 65 55 60 85 75 75 80 85 70 60 85 80 90 1,000 Hz 105 90 75 75 75 75 90 80 110 85 70 85 65 75 85 85 2000 Hz 90 100 75 80 110 75 95 80 80 75 70 75 70 70 85 85 4,000 Hz 100 110 80 80 100 95 110 100 85 90 80 90 110 80 95 95 BC 500 Hz 55 35 35 25 30 20 30 30 30 30 40 35 25 30 40 45 1,000 Hz 60 45 35 40 50 35 35 50 55 40 40 45 35 45 55 40 2000 Hz 50 55 50 55 55 60 45 50 45 50 50 45 45 50 60 50 4,000 Hz 55 65 60 70 45 65 70 55 50 60 55 65 75 60 70 75 Nonimplanted ear AC 500 Hz 95 20 10 70 105 70 35 25 10 10 75 10 25 85 15 30 1,000 Hz 90 15 45 70 100 90 55 30 5 25 55 25 25 80 30 25 2000 Hz 95 30 80 75 100 105 35 30 5 30 45 30 10 60 25 35 4,000 Hz 100 45 90 70 100 110 75 45 5 80 70 80 45 65 45 35 BC 500 Hz 50 15 5 45 60 55 20 20 5 5 40 5 0 40 5 20 1,000 Hz 50 10 40 40 70 65 40 25 0 20 25 20 5 45 25 20 2000 Hz 70 25 60 40 70 75 30 25 0 25 15 25 5 40 20 30 4,000 Hz 65 40 75 35 65 75 65 40 0 75 35 75 30 50 40 30AC indicates air conduction; BC, bone conduction.
Preoperatively, PTA4 for AC thresholds was between 75 and 98.75 dB HL (median [Me] = 83.1 dB HL) and remained stable in all subjects (i.e., there was a threshold shift of less than ±10 dB HL) both at the 1 month follow-up (preoperative versus 1 mo, t = 2.18; p = 0.045) and at the 12-month follow-up (pre versus 12 mo, t = 2.45; p = 0.027).
Likewise, PTA4 for BC thresholds was between 45 and 56.25 dB HL (Me = 46.25 dB) and remained stable in all subjects both at the short-term follow-up (pre versus 1 month, t = 0.70; p = 0.493) and at the long-term follow-up (pre versus 12 mo, t = 1.15; p = 0.270).
Average free-field hearing thresholds decreased from 79.2 dB HL (SD = 8.09 dB HL; Me = 78.75 dB HL) to 53.1 dB HL (SD = 5.02 dB HL; Me = 52.5 dB HL) after 6 months and to 54.5 dB HL (SD = 4.72 dB HL; Me = 53.75 dB HL) after 12 months. At both timeframes, the mean thresholds were significantly lower than before surgery (pre versus 6 mo, t = 15.11; p < 0.001 and pre versus 12 mo, t = 15.57; p < 0.001). At the 12-month follow-up, the PTA4 for BC was 48.1 dB, and average free-field hearing with Ponto was 54.5 dB, which indicated an average effective gain of −6.2 dB.
The average WRS results are presented in Figure 1. For all three level settings (50, 65, and 80 dB), WRS increased significantly from (respectively) 0%, 1%, and 16% before surgery to 34%, 70%, and 84% after 6 months and to 32%, 75%, and 88% after 12 months. For both timeframes, average WRS was significantly higher than before intervention (pre versus 6 mo, t = 11.44; p < 0.001 and pre versus 12 mo, t = 13.80; p < 0.001).
 FIG 1:
FIG 1: WRS results at 50, 65, and 80 dB preoperatively, and at 6 and 12 months postoperatively. The error bars represent SDs. SD indicates standard deviation; WRS, word recognition score.
Average SRT results are presented in Figure 2. Patient 11 was excluded from the analysis because of significant problems remembering words during the test. SRT in noise decreased from 14.07 dB signal-to-noise ratio (SNR) (SD = 3.17 dB; Me = 15.5 dB) before surgery to 6.32 dB SNR (SD = 4.99 dB; Me = 7.6 dB) after 6 months and 6.17 dB SNR (SD = 4.38 dB; Me = 6.8 dB) after 12 months, respectively. At both timeframes the average WRS was significantly lower than before intervention (pre versus 6 mo, t = 7.60; p < 0.001 and pre versus 12 mo, t = 9.27; p < 0.001).
 FIG 2:
FIG 2: SRTs in noise preoperatively, and at 6 and 12 months postoperatively. SRT indicates speech reception threshold.
Patient-Reported OutcomesThe results of 15 of 16 patients were included in the analysis (Patient 1 refused to fill in the questionnaires).
According to the CGI-S questionnaire, 14 of 15 patients reported that their hearing after implantation was much improved or very much improved. Just one patient (Patient 8) reported only minimal improvement in hearing. For the quality of life (QoL) question, 13 of 15 patients reported it was much improved or very much improved; for the other two (Patients 8 and 9), the QoL improved minimally.
The average GBI total score was 38.7 points (SD = 18.8; Me = 36.1) and was statistically significantly higher than 0 (t = 7.98; p < 0.001).
留言 (0)