Objective
This study focused on the intensities of cochlear implant (CI) stimulation in pediatric CI users with inner ear malformation or cochlear nerve deficiency (CND). In this population, CI programming is difficult because a large intensity of CI stimulation is required to achieve sufficient hearing, but the excess CI stimuli often induce facial nerve stimulation. We aimed to assess whether the results of intraoperative electrically evoked auditory brainstem responses (EABRs) testing predict maximum current levels of CI stimuli (cC levels) optimized by a behavioral-based method after long-term CI use.
Study Design
A retrospective case review.
Setting
A tertiary referral CI center.
Patients
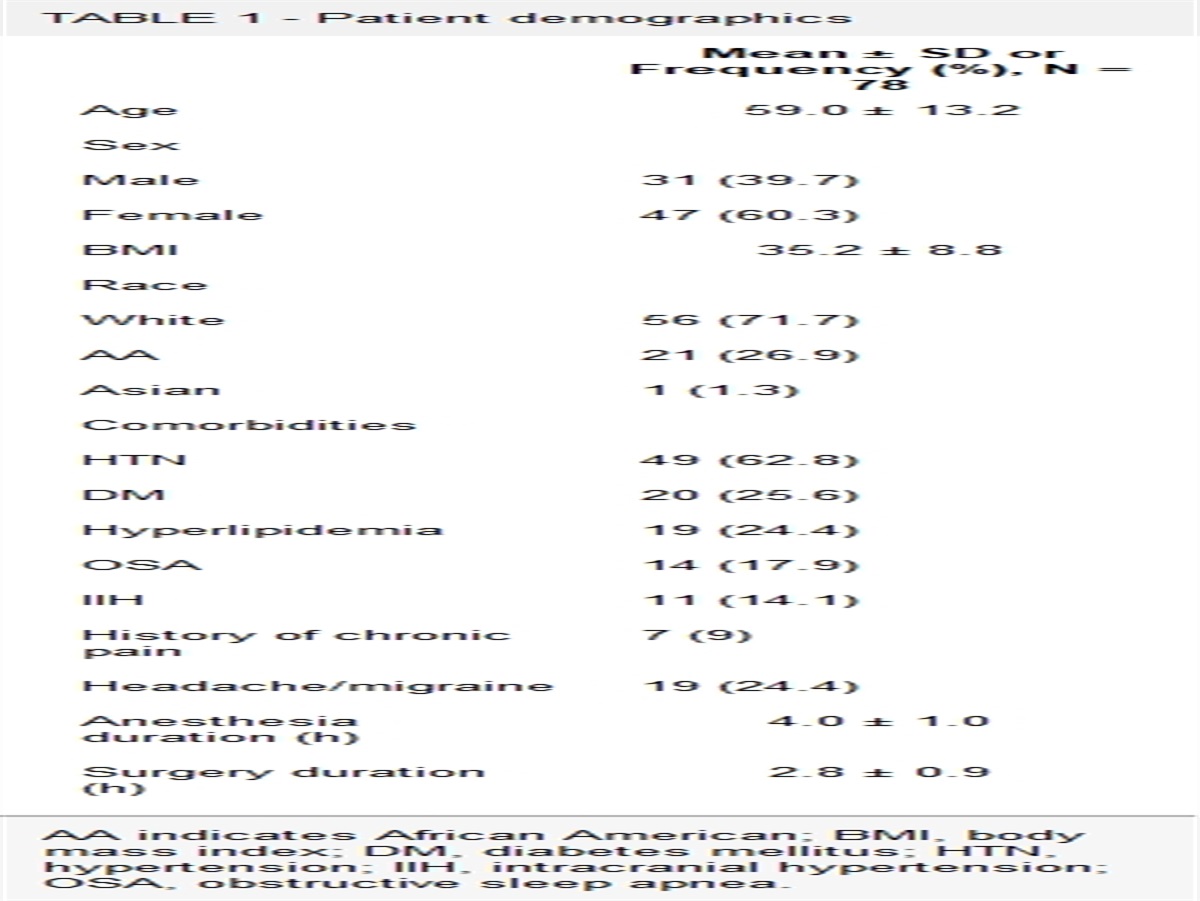
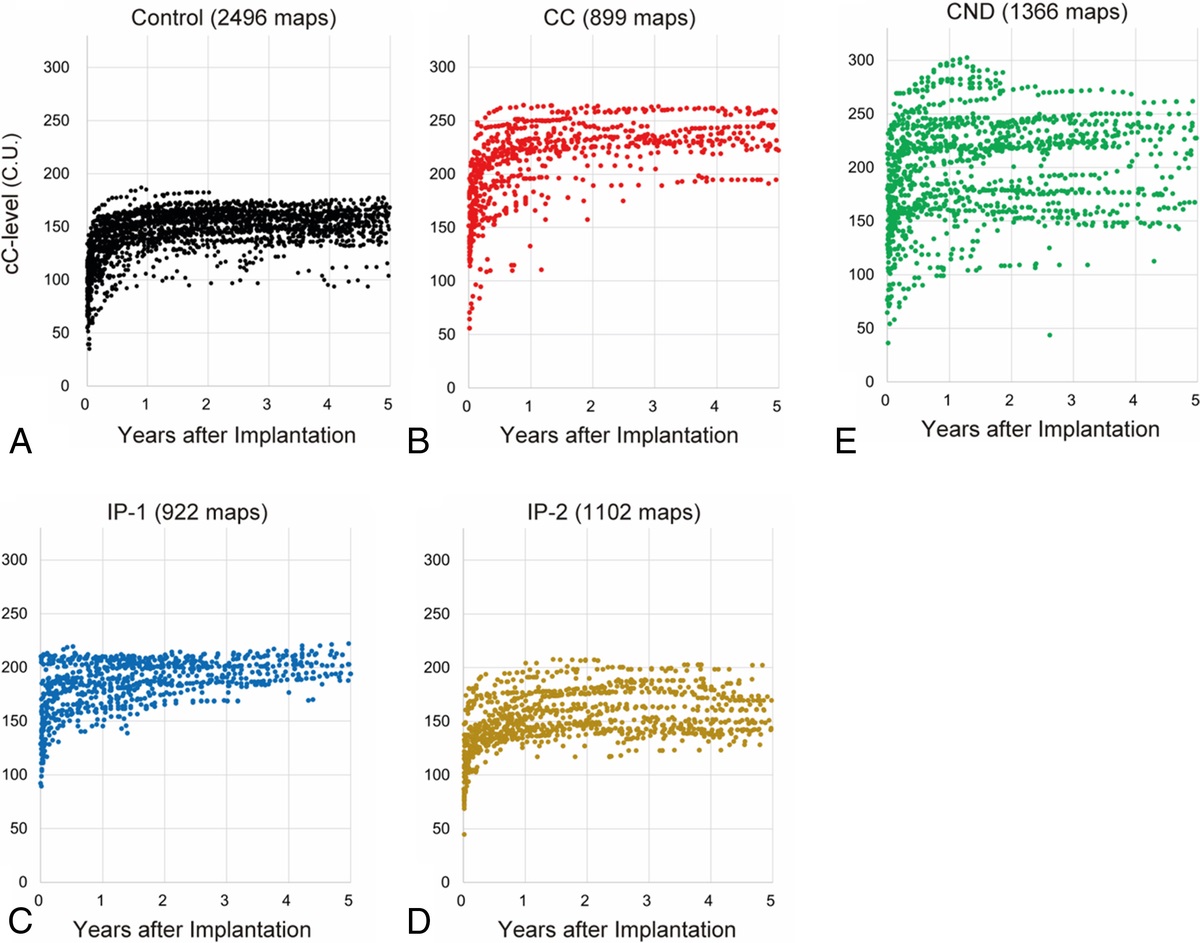
A total of 116 ears with malformations (malformation group) and 63 control ears (control group) from patients younger than 18 years who received CI. The malformation group comprised 23 ears with a common cavity (CC), 26 with incomplete partition type 1 (IP-1), 26 with incomplete partition type 2 (IP-2), and 41 with CND.
Intervention(s)
Diagnostic.
Main Outcome Measure(s)
Correlation between intraoperative EABR results and cC levels determined by the behavioral-based CI programming after long-term CI use.
Results
The CC, IP-1, and CND ears required significantly larger cC levels than the IP-2 ears and control groups. However, the cC levels increased to reach the plateau 1 year after surgery in all groups. Among the malformation group, 79 ears underwent intraoperative EABR testing. Greater than 80% of the CC, IP-1, and IP-2 ears and 54.8% of the CND ears exhibited evoked wave V (eV) and were included in the eV-positive category. Myogenic responses but no eV were observed in 18.2, 15.0, and 35.5% of the CC, IP-1, and CND ears, defined as the myogenic category. No eV or myogenic response was elicited in 9.7% of the CND ears. We focused on minimum current levels that elicited eV (eV levels) in the eV-positive category and maximum current levels that did not elicit any myogenic responses (myogenic levels) in the myogenic category. A significant relationship was detected between the eV levels and the cC levels. When analyzed in each malformation type, the eV levels significantly correlate with the cC levels in the CC and CND ears but not in the IP-1 and IP-2 ears, probably because of slight variation within the IP-1 group and the small number of the IP-2 group. The myogenic category did not show a significant relationship between the myogenic levels and cC levels, but the cC levels were similar to or smaller than the myogenic levels in most ears.
Conclusions
This study confirmed that intraoperative EABR testing helps predict the optimal cC levels in malformation ears. EABR-based CI programming immediately after cochlear implantation, followed by behavioral-based CI programming, may allow us to achieve early postoperative optimization of CI maps even in young children with severe malformations.

留言 (0)