
記住我







Eleven patients were included (eight male, three female). Baseline characteristics and responses are illustrated in Table 1. The median age at belantamab mafodotin initiation was 65 years (range 42–74) and 3 (27%) patients were aged over 70 years. Eight patients (73%) had λ AL-type and 3 (27%) κ AL-type. At diagnosis, the median involved free light-chain concentration was 534 (range 73–7181) mg/l. A median of two organs was involved at baseline (range 1–3): 9 (82%) had renal involvement and 4 (36%) had cardiac involvement. The median eGFR at the time of first belantamab mafodotin dose was 43 ml/min (range 7–120).
Table 1 Baseline characteristics and responses.The median time from AL amyloidosis diagnosis to first administration of belantamab mafodotin was 58 (range 12–154) months (~4.8 years) with a median of three prior lines of treatment (range 2–5). Prior therapies included immunomodulatory drugs (91%), proteasome inhibitors (100%) and anti-CD38 antibody (82%) treatment. Four patients (36%) had undergone prior melphalan-conditioned autologous stem cell transplantation.
At data cut-off, patients have received a median of 6 (range 1–11) doses of belantamab mafodotin. Response rates are shown in Fig. 1. Eight patients (73%) are still on therapy, ORR (partial response [PR] or better) was 64%. CR or very good partial response (VGPR) was achieved in 6 patients (55%). Reasons for treatment discontinuation (n = 1 each, 27% overall) were progressive disease and non-response or toxicity, respectively. At data cut-off, all patients were alive. At a median follow-up of 7.1 months (range 4.5–14.0), progression-free survival was 83% (95% confidence interval 27–97) and the median progression-free survival was not reached.
Fig. 1: Treatment response rates.
a Overall response rates; b Time to treatment response; Key: CR complete response, VGPR very good partial response, NR no response, ORR overall response rate.
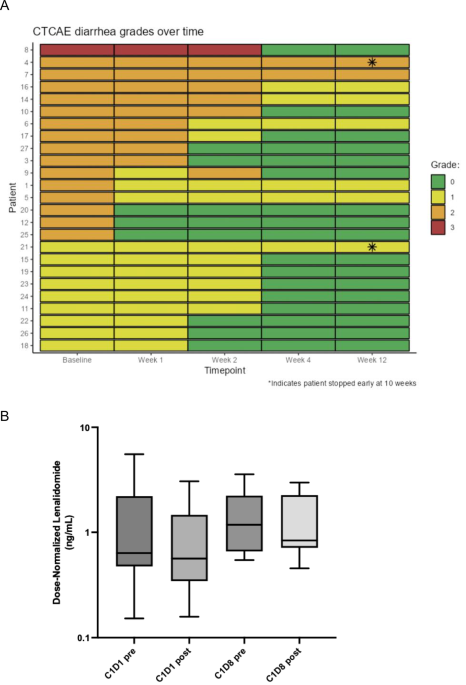
The most frequent adverse event was keratopathy, in all patients a bilateral microcystic corneal epitheliopathy. This occurred in 8 (73%) patients (grade 1–2: 55%; grade 3: 18%), necessitating dose and schedule modification of the three-weekly delivery in 4 (36%) patients. Ocular adverse events improved after treatment delay (increasing drug intervals to 4–6 weekly) and topical emollients with/without topical corticosteroids. One patient required treatment cessation due to ocular toxicity preventing further dose administration despite achieving PR after just one dose (patient 8).
One patient developed transient grade 1 dyspnoea and asymptomatic liver dysfunction which is similar to the rate reported in DREAMM-2. In our cohort, no patients developed cytopenia, which differed from DREAMM-2, which reported thrombocytopenia in 35% and anaemia in 24% as the most common adverse events after keratopathy. The only other series of reported belantamab mafodotin use in AL amyloidosis described thrombocytopenia in 17% (1/6) [2]. In our cohort, no infusion reactions were reported nor infections observed beyond COVID (two patients had mild infections not requiring hospital admission).
The majority of the cohort required dose reduction either at initiation (patient 4, due to end-stage renal failure and haemodialysis; patient 11, post-renal transplant) or during therapy (5/11; 45%: 3–1.9 mg/kg, 2–1.25 mg/kg). Only one patient remained on the standard dose of 2.5 mg/kg for ≥3 cycles. Four patients had an eGFR <30 ml/min with one patient experiencing grade 1 keratopathy. Two patients (patients 4 and 11) with end-stage renal failure commenced a dose of 1.25 mg/kg and achieved a VGPR and CR, respectively, with no additional toxicity. Patient 11 was treated with belantamab mafodotin after renal transplantation and was taking tacrolimus and mycophenolate mofetil as immunosuppression—we did not see any significant toxicity with a four-weekly dosing schedule and the patient achieved a CR at cycle 3. Patient 3 had a 42% reduction in the involved serum-free light chain after two doses but then had a prolonged gap due to keratopathy and lost the response. There were no treatment-related deaths, hospitalisations due to belantamab mafodotin and cardiac or renal toxicities observed in our cohort.
Belantamab mafodotin demonstrates significant activity in patients with heavily pre-treated AL amyloidosis with an ORR of 64%. Given the low grade underlying clonal dyscrasia in AL amyloidosis, these response rates appear to compare favourably with trial and real-world data of 30% achieving responses in relapsed myeloma. Effective novel therapies in multiply relapsed refractory AL amyloidosis are welcomed as data in this setting is scant. We recently reported real-world longitudinal data showing good outcomes and that responses do not significantly worsen with subsequent relapses in AL amyloidosis with 40–50% achieving at least a VGPR [6]. In the current cohort, apart from reversible keratopathy requiring dose modification and one treatment cessation, no other substantial toxicity was observed. Crucially, the common problems with AL amyloidosis treatment, often caused by steroids, like fluid retention and fatigue were not seen with belantamab mafodotin. Corneal toxicity was not unexpected; baseline and sequential ophthalmic examinations between belantamab mafodotin treatments allow monitoring for keratopathy. Of the current cohort, five patients would have been trial ineligible for the current prospective phase II trial (four due to renal impairment and one due to cardiac biomarkers). Two patients with severe renal impairment (stage V CKD) and one patient post-renal transplant tolerated treatment without additional toxicity and had good responses.
Our data has inherent limitations due to its retrospective nature and small sample size; however, we demonstrate good efficacy and tolerability of belantamab mafodotin in multiply relapsed AL amyloidosis including efficacy in patients with renal impairment. In summary, Belantamab mafodotin shows efficacy in our series of patients with multiply relapsed AL amyloidosis including those excluded from clinical trials. Further evaluation in prospective trials including those patients with advanced renal and cardiac disease is welcomed.
留言 (0)