
記住我









This prospective, single-arm, study investigated the feasibility of providing a prehabilitation program, with individualized exercise prescriptions, in patients scheduled for major abdominal cancer surgery who were identified as being at high risk for postoperative complications based on objective CPET-derived data informing of poor baseline functional capacity. The study was conducted at a tertiary/quaternary cancer center in Australia, with institutional ethics approval (LNR/18/PMCC/40).
ParticipantsConsecutive patients were screened for inclusion in this study at the pre-operative CPET Clinic. Patients being considered for major abdominal cancer surgery are routinely referred to the CPET clinic for risk stratification, to assess their suitability for surgery and for postoperative destination planning (e.g., surgical ward, extended recovery unit, HDU, or ICU). Patients were eligible for inclusion if they satisfied the inclusion and exclusion criteria presented in Table 1. Inclusion criteria were intentionally broad to include a real-world sample of high-risk patients preparing for major cancer surgery. Following agreement to participate, all patients were required to provide written informed consent. Participants then attended an appointment with a physiotherapist for baseline assessment of functional capacity (including a 6-min walk test (6MWT), handgrip strength testing, and 30-s sit to stand test), their individualized exercise prescription, respiratory exercises, and malnutrition screening. Participants identified as at risk of malnutrition on screening and/or in need of psychology input were referred to the dietetics and psychology services as part of standard care pathways.
Table 1 Inclusion and exclusion criteriaPrehabilitation programExercise interventionParticipants were prescribed an individualized exercise program based on the American College of Sports Medicine (ACSM) exercise guidelines for patients with cancer (Schmitz and Speck 2010) (Fig. 1). Given the complexity of this study population, exercise prescription was individualised to each person, with particular adaptions based on previous musculoskeletal injuries/issues (e.g., total joint replacements), symptoms such as pain and the patient’s exercise preferences. Exercise programs were prescribed and then progressed by a qualified physiotherapist or exercise physiologist based on participants’ response to exercise and adherence to the current exercise program. Goal setting and continued rating of self-efficacy allowed for individualized exercise interventions to be progressed and modified to achieve participant recognized important goals. Participants were given the choice of completing their exercise programs at the hospital or in settings closer to or within their home (e.g., home-based or community gyms). Further detail regarding the exercise intervention is provided as per the TIDieR checklist (Hoffmann et al. 2014) in Supplement 1.
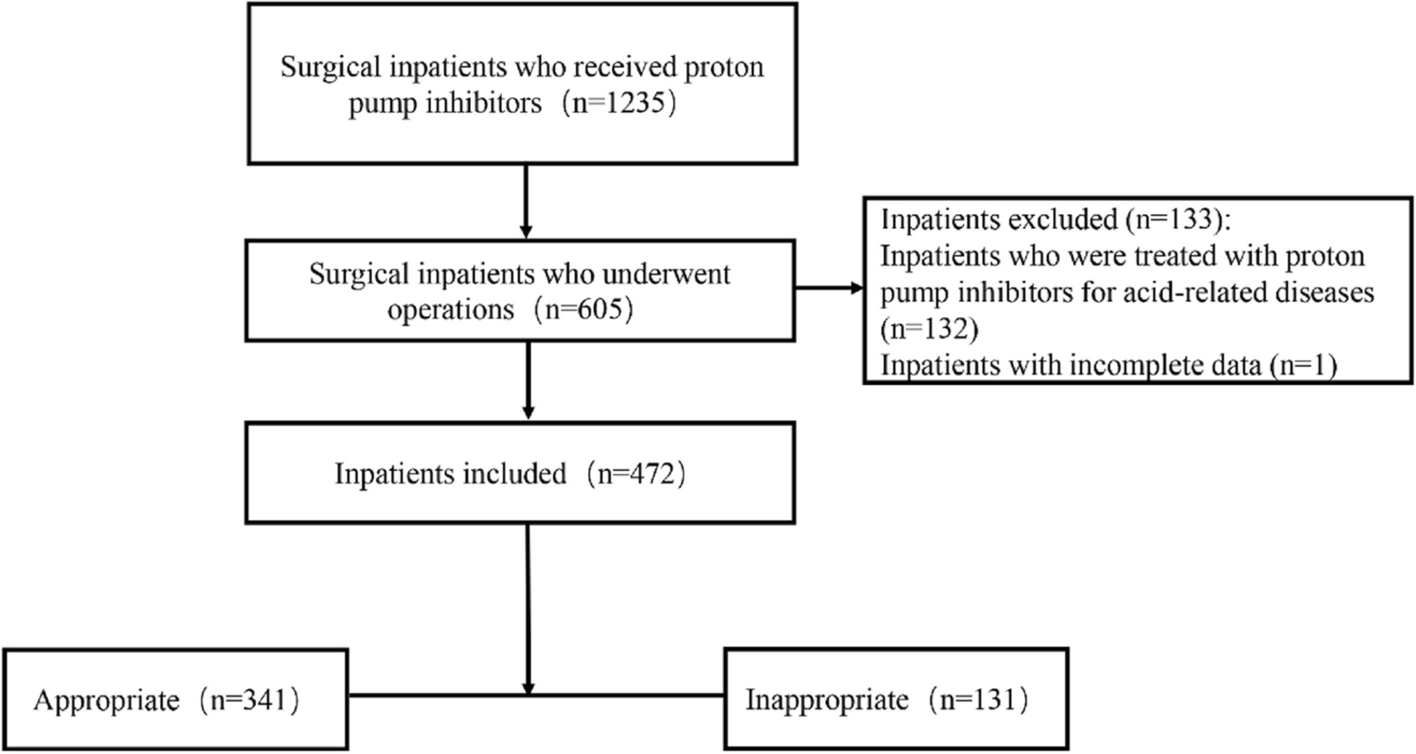
Fig. 1
Prehabilitation program flowchart
Breathing exercise interventionInformation on postoperative pulmonary complications and the importance of early postoperative ambulation, good pain relief, and breathing exercise prescriptions to prevent these complications were provided to all patients. Breathing exercises were based on the Active Cycle of Breathing (ACBT) technique (Lewis et al. 2012) and were provided in an educational session with practice supervised by a senior physiotherapist or senior nurse with experience in perioperative care.
Usual carePatients who were not eligible for recruitment into this study received standard/usual preoperative care. Standard care prior to March 2019 included a recommendation for pre-operative exercise advice as part of the pre-admission clinic, but this did not include supervised exercise training or physiotherapy sessions in the weeks leading up to surgery. Patients non-agreeable to the study after March 2019 were offered the same program of preoperative physiotherapy including preoperative exercise training, information/education, and screening for preoperative nutritional needs as the study participants through standard care as part of a newly established multidisciplinary prehabilitation service.
Postoperative carePostoperatively, study participants received standard postoperative care that included routine postoperative physiotherapy on postoperative day one and then ongoing physiotherapy as needed for respiratory management and early mobilization and individualized to patient needs. Following discharge from the hospital, standard care did not include referral to a standardized postoperative exercise program and is representative of current standard practice in Australia.
Study outcome measurementsPrimary study outcomes assessed for study feasibility, and secondary outcomes assessed for improved functional outcomes, patient well-being, and for incidence of postoperative complications. Functional outcomes were measured at baseline and the following prehabilitation. Postoperative complications were assessed at 30 days after surgery. Outcome assessors were not blinded to participation in the research study.
Feasibility (primary outcome)Feasibility was assessed by recruitment (number of patients screened and/or consented) and retention (number of participants who attended repeat CPET assessments), adherence with the intervention (based on compliance with the exercise prescription and attendance at breathing education sessions). To be considered feasible to design a larger more definitive efficacy study, we set the target for recruitment >70% of eligible participants consenting to enrol in the prehabilitation program (Thabane et al. 2010). Additionally, retention was assessed with a target of >85% of participants attending a second CPET test; and adherence with the prehabilitation program was assessed against the target of individuals achieving >70% of the prescribed exercise program (self-reported) during the study follow-up with phone calls.
Cardiopulmonary fitnessCPET was performed at baseline and at the end of the prehabilitation program as per the Perioperative Exercise Testing and Training Society (POETTS) practice guidelines (Levett et al. 2018). Tests were analyzed by anaesthetists accredited in CPET assessment. Gas exchange-derived variables were obtained during a ramp protocol with a cycle ergometer to ascertain participants’ cardiorespiratory fitness. Traditional CPET-derived parameters that were analyzed included oxygen consumption (VO2) at anaerobic threshold (AT; ml/kg/min) and at peak exercise (pVO2) corrected to both patient body weight (ml/kg/min) and to patient body surface area (ml/min/m2). VO2 at AT was determined according to the POETTS guidelines, using the three-point estimate of modified V-slope, ventilatory equivalents, and increasing end-tidal partial pressure of oxygen (PETO2) (Levett et al. 2018). The risk of postoperative pulmonary complications was assessed using the Assess Respiratory Risk in Surgical Patients in Catalonia (ARISCAT) Score (Canet et al. 2010).
Functional exercise capacity and strengthFunctional exercise capacity was assessed objectively using the 6-min walk test (6MWT) according to the American Thoracic Society guidelines (American Thoracic Society 2002). Physical Activity Levels were assessed subjectively by the International Physical Activity Questionnaire (IPAQ) (Craig et al. 2003). Handgrip strength was assessed on both dominant and non-dominant hands using a hydraulic handheld dynamometer (Baseline® Lite™ Hydraulic Hand Dynanometer, Baseline® Evaluation Instruments, Fabrication Enterprises, White Plains, NY10602, USA). Participants were given three attempts with both hands and the maximum reading recorded. Lower body strength was assessed using a sit-to-stand test over 30 seconds (Rikli and Jones 1999). Participants were instructed to sit in a standardized chair and stand up and sit down as many times as possible within 30 seconds.
Health-related quality of life (HRQoL) assessmentHRQoL was measured by the Functional Assessment of Cancer Therapy – General (FACT-G) (Cella et al. 2002). The total scores vary from 0 to 136, with higher scores indicating a better the quality of life. The Edmonton Symptom Assessment Scale (ESAS) was used to describe symptoms commonly seen in cancer patients. It involves eight visual analog scales (VAS) to indicate levels of pain, activity, nausea, depression, anxiety, drowsiness, appetite, and sensation of wellbeing (Bruera et al. 1991). A self-efficacy questionnaire was also administered (Rogers et al. 2006). This survey includes a nine-item scale that measures the most common barriers to exercise reported among cancer patients (including lack of discipline, nausea, exercise not a priority, bad weather, fatigue, lack of interest, time, lack of enjoyment, and lack of encouragement) and a four-item task self-efficacy which asked participants to rate their confidence in the ability to walk 20 min without stopping, run for 10 min without stopping, climb three flights of stairs without stopping, and exercise for 20 min at a level hard enough to cause a large increase in heart rate and breathing (Rogers et al. 2006). Self-efficacy was rated on a scale from 0 to 100% at 10% intervals. General headings were also provided as guides (not at all confident, 0–20%: slightly confident, 20–40%; moderately confident, 40–60%; very confident, 60–80%; extremely confident, 80–100%). The Malnutrition Screening Tool (MST), a simple, quick, valid, and reliable tool, was used to identify patients at risk of malnutrition (score of ≥2) (Ferguson et al. 1999).
Postoperative outcomesPostoperative outcomes that were measured included ICU admission and length of stay, days until the participant sat out of bed, medical emergency team (MET) calls during hospital admission, hospital length of stay, hospital re-admissions, and a patient centric measure—days at home within 30 days after surgery (DAH-30) (Myles et al. 2017). Postoperative pulmonary complications were assessed using the Melbourne Group Score (MGS version 2) (Parry et al. 2014) and postoperative complications were graded by the Clavien-Dindo scoring system (Dindo et al. 2004).
Statistical analysis of secondary outcomesGiven that this was a feasibility study, we did not undertake formal a priori power calculation. Rather, we recruited a study size of convenience that reflected our target population of high-risk patients deemed candidates for prehabilitation (Thabane et al. 2010). This feasibility study was not powered to test efficacy, did not include a control group, and we did not adjust for multiple factors because the aims of the study were exploratory. Continuous variables are reported as mean (range), mean (standard deviation, SD) or median (interquartile range, IQR), depending on distribution, and categorical variables as frequency (number, %). Change over time in physical activity, functional exercise capacity, strength, mood, and HRQoL of participants exposed to the intervention were examined from the baseline to completion of the intervention assessment time point (prior to surgery) and analyzed using paired samples t test. Linear mixed models were used to investigate change over time across the three timepoints; baseline, end of intervention (preoperative, prior to surgery), and 30 days postoperatively for 6MWT and handgrip strength testing. Regression analyses initially planned were not conducted as there was not enough data to make these analyses meaningful. All analyses were performed with the statistical software IBM SPSS Statistics Version 25 (SPSS© IBM Corp). Participants still awaiting surgery were followed up for a period of 100 days after the completion of the prehabilitation intervention prior to study closure. Participants who did not have their surgery by this follow up timepoint were not included in the postoperative analysis (n = 2 patients).
留言 (0)