
記住我


The use of intravenous (IV) medications via infusion pumps is a complex task inherently associated with patient safety risks.1–6 Because an estimated 90% of hospitalized patients require the controlled administration of medications using the intravenous route, IV infusion pumps are prevalent in health care.7 While there are various types of infusion pumps, large-volume IV smart pumps are the most versatile and thus are the most commonly used type of infusion pump in U.S. acute care.1,8–10
While data indicate that the use of IV smart pumps is associated with reductions in IV medication administration errors, medication errors have not been eliminated, including serious adverse drug events.11–16 Given the critical therapeutic role of IV medication administration using IV smart pumps in acute care, it is noteworthy that minimal research is available, which explores the fundamental causes of IV smart pump medication administration errors and the role of IV smart pumps in IV medication administration safety.
SECONDARY MEDICATION ADMINISTRATIONLarge-volume IV smart pumps are widely used in acute care settings throughout the United States to administer secondary medication infusions, with the antibiotics and electrolytes being the most commonly delivered secondary medications.9 When using a linear peristaltic IV smart pump for secondary medication administration, a head-height differential between the fluid level in the primary and secondary IV bags is required for the secondary medication to infuse. Head-height differential is measured from the top of the fluid level in the primary bag to the top of the fluid level in the secondary bag.6 When this differential between the primary container and the higher secondary container is not sufficient, the secondary will not infuse as intended, a medication error that often remains unnoticed until much later, resulting in medication delays or completely missed doses. Note that if head-height differential is inadequate, unintended flow from the primary container known as “concurrent flow” may result and not be evident at the beginning of the programmed infusion but will begin as the fluid level in the secondary bag decreases over the course of the programmed infusion. Flow rate inaccuracy is of even greater concern when secondary medication infusion rates are high not only for medications like Keppra and IV Tylenol but also for oncology medications, which are high volume, fast delivery rate, and time dependent.
Unfortunately, linear peristaltic IV smart pumps are prone to use error because the setup process must be managed manually at the point of care.6,9,17,18 Failure to adhere to setup specifications during clinical use may lead dangerous medication errors due to deviation in flow rate between what is actually delivered to the patient and what was programmed into the pump by the clinician. Furthermore, it is important to note that all testing results use ±5% as the benchmark for Food and Drug Administration regulatory submissions for flow rate accuracy and only report on single-channel, primary line infusions. Additional details on flow rate accuracy for the Baxter Spectrum IQ (Baxter Healthcare Corporation, Deerfield, Ill), the clinical conditions that impact flow rate accuracy, and the specific testing conditions used to determine flow rate accuracy are described in Appendix B of the Spectrum IQ Operators Manual.19 Clearly, the conditions under which fluid flow accuracy is tested and reported for Food and Drug Administration regulatory approval do not represent the most common conditions under which these IV smart pumps are used in the clinical setting. In addition, adherence to the required setup is often not possible in the clinical setting because of patient care needs, constraints related to clinical workflow, and space limitations. The operator’s manual is extensive and includes technical language that may not be readily incorporated into clinical practice by busy clinicians at the point of care.
In recent guidelines created to optimize IV smart pump safety, the Institute for Safe Medication Practices recommends the use of delivery systems for secondary medication administration that do not use head-height differential.8 We have previously published an observational study of secondary infusion, which included the BD/Alaris IV smart pumps (Becton, Dickinson and Company, Franklin Lakes, NJ).9 The purposes of this study were to complete the collection of data on the same observations using the Baxter Spectrum IQ IV Smart Pump and to add additional exploratory variables of interest, which are described hereinafter. Hypotheses are based on the complexity of setup requirements for head-height differential systems, complexity of operator’s manual, clinical observation, and author experience.
Our work is based on a human factor perspective,20 and in our previous work, we have outlined the limitations of current technology,1,6,21,22 studied clinician knowledge,23 studied the impact of interruptions,24 and looked at the use of the BD/Alaris, ICU Medical (ICU Medical, Inc., San Clemente, CA), and Ivenix large volume IV smart pumps (50 High St Suite 50, North Andover, MA) during actual clinical use.9,25 Thus, for this study, we again chose to use a real-world approach to observe how the Baxter/Sigma IV smart pumps (One Baxter Parkway Deerfield, IL) are used during actual clinical use.
SYSTEM SETUPMost large volume IV smart pumps used in U.S. acute care use linear peristaltic technology for IV infusion, which require very specific system setup for accurate fluid flow.6 Furthermore, clinician knowledge of these setup requirements is low, and proper setup varies across IV smart pump models.23 Currently, the largest shares of the U.S. acute care market are held by 2 brands of linear peristaltic large-volume IV smart pumps: BD/Alaris at more than 50% of the market; and Baxter Spectrum IQ IV Smart Pump, at approximately 25% to 30% of the market.9,26 This study will focus on the Baxter Spectrum IQ IV smart pumps, and details for proper setup according to their manufacturer guidelines are provided hereinafter.19
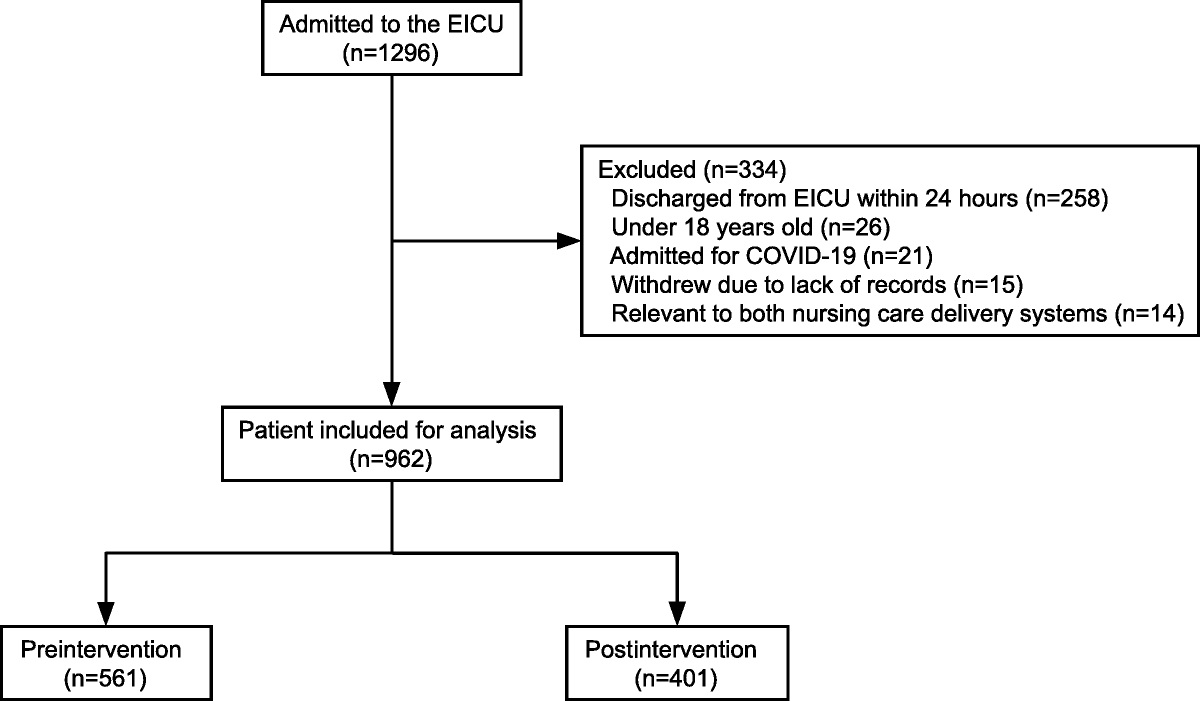
For primary infusion: Place the IV smart pump vertically on the IV pole at the position most level with the IV insertion site. Hang the primary container above the pump, ensuring the top of the fluid line is 24 ± 2 inches above the center of the pump.22 For secondary infusion: The distance required for the Baxter Spectrum IQ to infuse from a secondary medication bag is the same as for a primary infusion, 24 ± 2 inches above the center of the IV smart pump. However, for the secondary bag to infuse instead of the primary bag, the position of the primary bag must be lowered. This should be done by fully extending the secondary infusion hanger to allow for the required head-height differential. This is the minimal distance needed to generate enough hydrostatic pressure to close the check valve (Fig. 1, #1) in the primary tubing and ensure secondary flow (Fig. 1, #2).18 If hydrostatic pressure is not sufficient or there is a failure in the check valve, there will be concurrent flow from both the primary and secondary fluid bags, or no flow at all from the secondary bag while only the primary bag infuses, both resulting in medication error that is difficult to detect. The roller clamp (Fig. 1, #3) on the secondary tubing must be manually opened during the secondary infusion and closed during the primary infusion. No pump alert will occur if the roller clamp remains inadvertently closed during the secondary infusion. Instead, fluid will be infused from the primary bag at the programmed secondary flow rate, also resulting in a secondary medication administration error.The manufacturer guidelines for infusion delivery referenced previously create complexities at the point of care. It is common for the primary bag to be programmed to resume flow after infusion of the secondary medication either as a resumption in therapy or to help flush residual medication out of the tubing and out of the venous access device. Unfortunately, this poses a challenge from a flow accuracy standpoint. For accurate flow, the intended infusion fluid bag must be 24 ± 2 inches above the vertical centerline of the pump. To achieve this, the ideal practice would be to raise the primary bag back to the accurate infusible height of 24 ± 2 inches immediately after the completion of the secondary infusion. Because of time demands, ergonomic limitations, and the realities of the clinical workflow demands, this manual process creates an unreasonable clinical expectation, further adding to deviations from intended flow rate.
 FIGURE 1:
FIGURE 1: Required components for secondary medication infusion using the head-height differential method (used with permission from Karen K. Giuliano).
RESEARCH AIMS AND HYPOTHESES Aim 1What is the adherence with manufacturer system setup requirements that the pump be placed level with the IV insertion site for the Baxter Spectrum IQ large-volume IV smart pump during actual clinical use?
We hypothesize that the IV smart pump placement relative to the IV insertion site for accurate infusion will be insufficient at least 75% of the time with Baxter Spectrum IQ large-volume IV smart pumps.
Aim 2What is the adherence with manufacturer system setup requirements for primary infusion for the Baxter Spectrum IQ large-volume IV smart pump during actual clinical use?
We hypothesize that the required bag height differentials for appropriate primary infusion will be insufficient at least 75% of the time with the Baxter Spectrum IQ large-volume IV smart pumps.
Aim 3What is the adherence with manufacturer system setup requirements for secondary infusion for the Baxter Spectrum IQ large-volume IV smart pump during actual clinical use?
We hypothesize that the required bag height differentials for appropriate secondary medication administration will be insufficient at least 50% of the time with the Baxter Spectrum IQ large-volume IV smart pumps.
In addition to the 3 primary aims, we also collected data on the following additional variables: type of secondary medication; use of secondary medication hanger; secondary tubing connection; use of a check valve; status of secondary tubing clamp during infusion; presence of concurrent primary flow during secondary infusion; incomplete secondary volume delivery; and primary and secondary rate mismatches. This list of exploratory variables was based on knowledge gained from our previous work. These data will help provide additional context to our findings, will help further inform the results of our research aims, and can provide a foundation for additional inquiry for improving the accuracy and safety of these widely used and important therapeutic devices.
STUDY DESIGN AND METHODOLOGY SettingThe study design was observational and noninterventional. The study site was a 285-bed community hospital in the Boston area. Data collection began shortly after institutional review board approval was obtained, and all data were collected by a single observer.
SampleA total of 200 primary and secondary IV medication administration observations were included in this study: 101 in critical care and 99 in medical-surgical units. Observations were collected in real-time on a case report form, which did not include protected patient health information.
Inclusion CriteriaThose eligible for inclusion in the study were all adult patients, 18 years or older, admitted to either the critical care or medical-surgical units, and requiring at least 1 active secondary IV medication order.
Exclusion CriteriaAdult patients hospitalized in the study units without at least 1 active secondary IV medication order were excluded.
Procedures To verify the electronic health record medication orders, patient identification was confirmed for all observations; however, no protected health information was documented on the case report form. A study number was assigned to each secondary medication observation. Direct observation of each secondary medication administration was done to assess the head-height differential setup by: Observing the position of the IV smart pump relative to the IV insertion site. Measuring the distance between the top of the primary fluid level and the vertical centerline of the IV smart pump. Measuring the secondary head-height differential as the difference between the top of the primary fluid level to the top of the secondary fluid level at the beginning of the secondary infusion. Confirming the presence or absence of a primary line check valve. Observing the position of the secondary medication tubing roller clamp as open or closed. Consistent with the Institute for Safe Medication Practices guidance, secondary medications were recorded as given on time if administered within 30 minutes from order time or delayed if administered outside of the 30-minute time window.27 Medication doses documented as omitted medications included those doses not completed before the next scheduled dose. Names of all observed secondary IV medications were collected. Collection of the additional exploratory data. RESULTSData on 200 secondary IV medication administration observations (101 in critical care and 99 in medical-surgical) were completed. All analyses were completed using IBM SPSS Statistics for Windows, Version 25.0 (IBM Corp., Armonk, NY) by Karen K. Giuliano, PhD, RN.
Aim 1What is the adherence with manufacturer system setup requirements that the pump be placed level with the IV insertion site for the Baxter Spectrum IQ large-volume IV smart pump during actual clinical use?
There were 13 IV smart pumps (6.5%) observed that were placed at the level of the insertion site. Of the remaining 187 observations, the mean distance for IV smart pump placement above the IV insertion site was 13.9 inches, standard deviation of 5.3 inches, and a range of 3 to 31 inches above the insertion site. There were no observations where the IV smart pump was placed below the IV insertion site. Independent samples t test found no difference in the mean distance for IV smart pump placement above the IV insertion site between ICU (13.7 inches) and medical-surgical (14.0 inches) observations.
Aim 2What is the adherence with manufacturer system setup requirements for primary infusion for the Baxter Spectrum IQ large-volume IV smart pump during actual clinical use?
A total of 13 observed IV smart pump infusions were placed at the required head height of 24 ± 2 inches (22–26 inches) between the vertical centerline of the IV smart pump and the top of the fluid level in the primary bag. This represents a 6.5% adherence with manufacturer requirements if the secondary infusion was expected to be followed by a primary flush or continuous primary infusion. For all observations, the mean distance for IV smart pump placement was 14.1 inches, standard deviation of 4.0 inches, and a range of 0 to 28 inches. Independent samples t test found no difference in the means between ICU (14.0 inches) and medical-surgical (14.1 inches) observations.
Aim 3What is the adherence to manufacturer system setup requirements for secondary infusion for the Baxter Spectrum IQ large-volume IV smart pump during actual clinical use?
We observed 59 secondary infusions (29.5%) where the hanger was folded and not being used in the fully extended position and, therefore, was not in adherence with manufacturer requirements, thus contributing to the low setup adherence rate. During 139 of the observed secondary infusions (69.5%), the head height differential between the primary and secondary IV bags was equal to or greater than the 12.5 inches. The mean distance for IV smart pump placement relative to the top of the fluid level in the secondary infusion container was 13.3 inches, standard deviation of 3.2 inches, and a range of 5 to 20 inches. Independent samples t test found no difference in the means between ICU (13.6 inches) and medical-surgical (12.9 inches) observations.
ADDITIONAL VARIABLES EXPLOREDThe types of secondary medications delivered are summarized in Table 1. The observations for the additional questions can be found in Table 2.
TABLE 1 - Secondary Medication Type by Therapeutic Class Type of Medication n % Antibiotic 167 83.5% Electrolyte/vitamin 18 9.0% Other 12 6.0% Other anti-infective 3 1.5% Total 200 100%*Not all these observations occurred while the medication was actively infusing, so some aspects of these observations were recorded as uncertain, resulting in some totals that were less than 200.
There were 3 medication errors found during the observations: 1 delayed dose (0.5%) and 2 omitted doses (1%) due to closed secondary clamps. There were also 6 observations where basic infusion/IV fluids was used for dose programming instead of the drug library to program the administration of antibiotics. This is concerning because of the safety features that are available through the use of the drug library to reduce risk of medication error.
DISCUSSIONFor aim 1, it was found that only 6.5% of all observations had the IV smart pump positioned at the level of the IV insertion site. At a mean of 13.9 inches, the distance for IV smart pump placement was substantially above the proper placement for accurate flow. If the IV insertion site is approximately equal in pressure to the pressure in the right atria, then an increase in pump height of 13.9 inches will increase flow rate by 2.5%, and this combined with other factors affecting accuracy could lead to a flow rate deviation that puts the patient at risk.6 In addition, if the level of the IV smart pump is above the level of the patient, it becomes more difficult to achieve required IV bag heights because clinicians are no longer able to actually reach the infusion bags.
Unfortunately, the operator’s manual provided for reference offers very ambiguous guidance regarding the height of the pump relative to the patient.19 It is through an understanding of the technology and our best interpretation of the manufacturer’s guidance that we provide this clinical guidance. The manual19 reads as follows:
“A fluid container is positioned above or below the patient’s administration site, pressure forces associated with the fluid’s head-height (distance measured from the center of the pump to the top of the fluid in the source container) cause deviations in the nominal specification for device flow rate accuracy.” (B-1)
“Always hang the fluid container so that the level of fluid in the container is 610 ± 51 mm (24 ± 2 in) above the center of the infusion pump.” (B-1)
Additional manufacturer information references only the position of the primary and secondary infusions relative to the IV smart pump, and not to patient. Given the importance of primary and secondary infusion placement relative to both the patient and the IV smart pump location that is needed for accurate flow, we find the current manufacturer guidance to be lacking the specificity needed for actual clinical use. This is especially concerning for a device that is ubiquitous in acute care and carries such a high risk for patient safety.
For aim 2, there was 6.5% adherence with manufacturer requirements for primary infusion bag height. If we assume that the pump was programmed to deliver a flush dose or continuous infusion of the primary fluid after the completion of the secondary medication, then the flow of fluid from the primary bag would not be accurate unless it was repositioned to the required primary bag back of 24 ± 2 inches after completion of the secondary infusion. As previously discussed, this an unrealistic expectation for clinicians. Not only is it impractical for nurses to be called back into a patient’s room on completion of every secondary medication, but also the Baxter pump does not allow the clinician to program a secondary infusion without also programming a primary flush. This feature eliminates the opportunity for notification immediately upon secondary infusion completion. Furthermore, if the clinician follows both primary and secondary head-height requirements (placement of primary bag 24 ± 2 inches above the pump and hanging the secondary bag by a fully extended hanger), the secondary infusion would be hanging approximately 36.5 inches above the vertical centerline of the pump, potentially leading to an increase in flow of about 1.2% compared with the programmed rate.6 Thus, the only way to comply with both requirements is to constantly move the positions of the primary and secondary infusions with each secondary medication administration. The complexity of this situation illustrates the clinical impracticality of these manual head-height requirements for high-risk IV medication administration for care of acutely ill patients.
Until IV smart pumps with less setup complexity become more widely used, clinicians who use head-height dependent IV smart pumps such as the Baxter Spectrum IQ cannot practically expect flow rate accuracy during actual clinical use. Finally, the head-height requirement for accurate flow only impacts the intake pressure (pressure generated above the pump) needed for accurate flow.6 Outlet pressure (pressure below the IV smart pump which creates resistance to forward flow) also decreases flow rate accuracy and is caused by common clinical factors such the use of long, narrow venous access devices, the use of needless connector, long extension tubing, and high fluid viscosity.6
For aim 3, there was 69.5% adherence with the required setup using a fully extended hanger. The concern for the other 29.5% of infusions is that the inadequate head-height differential that results from use of a folded hanger will lead to concurrent flow from both primary and secondary bags, which will likely worsen as fluid level in the secondary bag decreases. Furthermore, even with the use of a fully extended hanger, when the primary and secondary infusions are hung on separate IV poles, the head-height differential may be insufficient despite a fully extended hanger. In either case, the result is decreased secondary flow rate or concurrent flow with the primary. In the worst case, the secondary medication may not flow at all while the primary fluid infuses at the secondary programmed rate. When the pump indicates that the secondary infusion has completed, there will still be fluid volume in the secondary bag despite the pump indicating delivery of the fully programmed volume. This is because volume displayed by the pump is calculated based on the infusion duration and the programmed rate, not secondary fluid volume, something most clinicians do not realize.23
With regard to the additional exploratory variables, several of the findings are of interest because of their impact on the accuracy of IV smart pump fluid flow.
While the hangers for secondary infusion were used 100% of the time, almost 30% of the time they were used incorrectly. This practice likely caused a decrease in actual IV flow rate, contributing to secondary medication underdelivery and occult medication administration error. There were 5 observations (2.5%) where the secondary medication was connected to a Y-site below the level of the pump. This setup completely bypasses the ability of the IV smart pump to regulate the secondary infusion, making the flow rate dependent on the manual adjustment of the roller clamp. When this occurs, the flow of the secondary medication is entirely gravity dependent with no flow regulation from the pump. In addition, once the fluid in the secondary medication has been fully infused, there is no IV pump safeguard to identify alert the user if air from the medication infusion has entered the IV tubing, creating a potentially serious safety hazard to the patient. Concurrent fluid flow from the primary infusion during secondary infusion was observed 24% of the time, and in 61% of the observations, there was volume remaining in the secondary medication bag after the pump indicated that the infusion was complete. Finally, there were observations where the primary was infusing at the secondary rate, and where the secondary was infusing at the primary rate. These are all important findings that should be of concern to all acute care clinicians as these findings provide additional evidence that nonadherence with these complex system setup requirements is having a negative impact on the delivery of IV smart pump medication administration. The findings presented in Table 1 documenting the frequency of secondary medication type are consistent with the findings from previous research regarding the types of medications that are most commonly administered using secondary infusion.9 LIMITATIONSThe authors recognize that the study used a point prevalence, convenience sample approach, and made no attempt to observe each infusion from beginning to end. This limits the ability to fully understand the full implications of the observations. Data were collected in a single site, which may or may not reflect overall infusion practices in all U.S. acute care hospitals. In addition, nurses were not interviewed about their decision-making process regarding setup choices made. Given the complex setup requirements of head-height dependent IV smart pump systems and the lack of frontline clinician knowledge19 regarding these requirements, the authors acknowledge that there are times in real-world clinical environments in which the ideal setup is difficult or impossible to achieve. Thus, in the short term, we need clinicians to be well-informed regarding the technical limitations of head-height dependent systems, so clinicians can weigh options to minimize overall risk. A larger-scale trial including multiple sites, additional IV smart pump types, various hospital sizes, clinician interviews, and a larger sample size is needed to more fully understand IV smart pump medication administration practices that can be generalized to broader populations.
CONCLUSIONS AND IMPLICATION FOR FUTURE RESEARCHThese findings provide additional evidence to support that adherence to manufacturer setup requirements of head-height dependent IV smart pump is difficult, if not impossible, to achieve during actual clinical use. Acute care clinical settings have substantial physical space limitations at the bedside, there is competition for space with other bedside equipment, workflow realities such as the need for patient mobility and transport, and the limited availability of appropriate and mobile IV poles all contribute to the ability of clinicians to comply with IV smart pump head-height differential system setup requirements. Furthermore, as the vast majority of nurses are women with an average height of 5′3.5″,28 most would need to stand on stools to achieve the required head heights, which is not realistic and also creates a significant clinician safety hazard.
Coupled with a larger-scale study, additional knowledge assessments of frontline caregivers on this topic are warranted. Learning more about the overall knowledge level of professional nurses regarding technical requirements, limitations, and clinical outcomes, as well as potential for error during secondary medication administration, is needed. This crucial information can be used to inform the development and application of educational materials to assist clinical decision making to improve the safety of the secondary medication administration process, even if only in the interim as more comprehensive practice-based research data are collected. Even if relevant knowledge is provided to every frontline nurse, the present system requirements for using head-height differential systems to obtain flow rate accuracy are too complex to achieve consistency at the point of care, putting patients at risk for serious medication error. The use of head-height differential IV smart pumps, which require a check valve, is outdated and risk-prone even when applied to relatively low risk uses such as small volume antibiotic doses, the complexity of the manual setup process is unacceptable and poses a significant risk to patient safety. To improve this process for both nurses and patient safety, consideration of alternative human factors–designed technology that can replace manual processes is needed. This need has already been recognized by the Institute for Safe Medication Practices in their most recent guidance, where they recommend the use of systems for secondary medication infusion that do not require a head-height differential.8
Clearly, there is an urgent need for IV smart pump innovation, based on human factors usability design, to create solutions which better address the real-life clinical issues that exist at the point of care. The need to improve IV smart pump usability sits at the crossroad of clinical workflow and patient safety, and IV smart pump manufacturers have a responsibility to invest in more innovative technology solutions to improve the process of care in this very important area of patient safety.
REFERENCES 1. Giuliano KK. Intravenous smart pumps: usability issues, intravenous medication administration error, and patient safety. Crit Care Nurs Clin North Am. 2018;30:215–224. 2. Giuliano KK. IV Smart pumps and error-prone programming tasks: comparison of four devices. Biomed Instrum Technol. 2018;52(s2):17–27. 3. Ding Q, Barker KN, Flynn EA, et al. Incidence of intravenous medication errors in a Chinese hospital. Value Health Reg Issues. 2015;6:33–39. 4. Fahimi F, Sefidani Forough A, Taghikhani S, et al. The rate of physicochemical incompatibilities, administration errors. Factors correlating with nurses’ errors. Iran J Pharm Res. 2015;14(Suppl):87–93. 5. Di Muzio M, De Vito C, Tartaglini D, et al. Knowledge, behaviours, training and attitudes of nurses during preparation and administration of intravenous medications in intensive care units (ICU). A multicenter Italian study. Appl Nurs Res. 2017;38:129–133. 6. Giuliano KK, Blake JWC, Butterfield R. Secondary medication administration and IV smart pump setup. Am J Nurs. 2021;121:46–50. 7. Husch M, Sullivan C, Rooney D, et al. Insights from the sharp end of intravenous medication errors: implications for infusion pump technology. Qual Saf Health Care. 2005;14:80–86. 8. Institute for Safe Medication Practices (ISMP) Guidelines for Optimizing Safe Implementation and Use of Smart Infusion Pumps. 2020. Available at: https://www.ismp.org/guidelines/safe-implementation-and-use-smart-pumps. Accessed July 1, 2022. 9. Giuliano KK, Penoyer D, Mahuren RS, et al. Intravenous smart pumps during actual clinical use: a descriptive comparison of primary and secondary infusion practices. J Infusion Nurs. 2021;44:128. 10. Smart pumps in practice: survey results reveal widespread use, but optimization is challenging. Institute for Safe Medication Practices. 2018:11. Published April 5, 2018. Available at: https://www.ismp.org/resources/smart-pumps-practice-survey-results-reveal-widespread-use-optimization-challenging. Accessed July 2, 2019. 11. Ohashi K, Dalleur O, Dykes PC, et al. Benefits and risks of using smart pumps to reduce medication error rates: a systematic review. Drug Saf. 2014;37:1011–1020. 12. Ohashi K, Dykes PC, McIntosh K, Buckley E, Wien M, Bates DW. Evaluation of intravenous medication errors with smart infusion pumps in an academic medical center. Paper presented at: AMIA 2013 Annual Symposium. November 19, 2013 - November 20, 2013. Washington Hilton hotel, Washington, DC. 13. Kane-Gill SL, Kirisci L, Verrico MM, et al. Analysis of risk factors for adverse drug events in critically ill patients. Crit Care Med. 2012;40:823–828. 14. Nuckols TK, Bower AG, Paddock SM, et al. Programmable infusion pumps in ICUs: an analysis of corresponding adverse drug events. J Gen Intern Med. 2008;23 Suppl 1(suppl 1):41–45. 15. Schnock KO, Dykes PC, Albert J, et al. The frequency of intravenous medication administration errors related to smart infusion pumps: a multihospital observational study. BMJ Qual Saf. 2017;26:131–140. 16. Schnock KO, Dykes PC, Albert J, et al. A multi-hospital before-after observational study using a point-prevalence approach with an infusion safety intervention bundle to reduce intravenous medication administration errors. Drug Saf. 2018;41:591–602. 17. Cassano-Piché A, Fan M, Sabovitch S, et al; Health Technology Safety Research Team; Institute for Safe Medication Practices Canada. Multiple intravenous infusions phase 1b: practice and training scan. Ont Health Technol Assess Ser. 2012;12:1–132. 18. Chan KY-Y, Pinkney S, Fan M, et al. Mitigating Risks Associated with Secondary Intravenous Infusions: An Empirical Evaluation of a Technology-based, Trainingbased, and Practice-based Intervention. The Canadian Medical and Biological Engineering Society, Vol 36, published May 21, 2013. Available at: https://proceedings.cmbes.ca/index.php/proceedings/article/view/400. Accessed July 1, 2022. 19. Baxter Healthcare. Operators Manual Spectrum IQ Infusion System With Dose IQ Safety Software Version 9. Deerfield IL; 2018. Available at: https://service.baxter.com/tsportal. Accessed July 1, 2022. 20. Carayon P, Wetterneck TB, Hundt AS, et al. Obseving Nurse Interaction With Infusion Pump Technologies. 2005. Advances in Patient Safety. 2005;2:349–364. 21. Blake JWC, Giuliano KK. Flow accuracy of IV smart pumps outside of patient rooms during COVID-19. AACN Adv Crit Care. 2020;31:357–363. 22. Blake JW, Giuliano KK, Butterfield RD, et al. Extending tubing to place intravenous smart pumps outside of patient rooms during COVID-19: an innovation that increases medication dead volume and risk to patients. BMJ Innovations. 2021;7:379–386. 23. Giuliano KK, Jeannine W, Blake C. Nurse and Pharmacist Knowledge of Intravenous Smart Pump System Setup Requirements. Biomed Instrum Technol. 2021;55:51–58. 24. Campoe KR, Giuliano KK. Impact of frequent interruption on nurses’ patient-controlled analgesia programming performance. Hum Factors. 2017;59:1204–1213. 25. Penoyer D, Giuliano K, Middleton A. Comparison of safety and usability between peristaltic and pneumatic large-volume intravenous smart pumps during actual clinical use. BMJ Innovations. 2022:bmjinnov-2021-000851. 26. Market and Markets. Infusion Pump Market by Product [Accessories (Dedicated, Non-dedicated), Devices (Volumetric, Insulin, Syringe, Ambulatory)], Technology (Traditional, Specialty), Application (Cancer, Diabetes), & Setting (Hospital, Homecare) (2022 – 2026). Available at: https://www.marketsandmarkets.com/Market-Reports/infusion-pumps-accessories-market-90374506.html. Accessed July 5, 2022. 27. Institute for Safe Medication Practices (ISMP). Acute Care Guidelines for Timely Administration of Scheduled Medications. 2011. Available at: https://www.ismp.org/sites/default/files/attachments/2018-02/tasm.pdf. Accessed July 1, 2022. 28. Centers for Disease Control and Prevention. US body measurements. National Center for Health Statistics Web site. Available at: https://www.cdc.gov/nchs/fastats/body-measurements.htm. Published 2020. Accessed July 1, 2022.
留言 (0)