Trial design
This study was a double-blind, placebo-controlled clinical trial, registered at the Iranian Registry of Clinical Trials website (IRCT, www.irct.ir) with the Ref. No IRCT20121216011763N44 and the CONOSRT guidelines were used for clinical trial reporting [17]. An information sheet was provided to participants and signed informed consent was obtained prior to the study. Approval was obtained from the Ethics Committee of the Isfahan University of Medical Sciences (approval number: IR.MUI.RESEARCH.REC.1398.532).
Inclusion & exclusion criteria
Women were enrolled from two neurology clinics (Imam Moosa Sadr and Khurshid) affiliated with the Isfahan University of Medical Sciences, Isfahan, Iran, between January 2020 and March 2020. Patients were eligible to participate if they were more than 18 years old until menopause/perimenopause ages diagnosed as having migraine by a neurologist (F.K) based on ICDH-3 criteria [18]; and willing to participate in the trial.
Exclusion criteria were: women with menopause/perimenopause symptoms or/and endometrial and breast cancer, ovarian cysts, uterine fibroids and uterine polyps diagnosed by a gynecologist (H.G); pregnancy or intention to pregnancy and lactation; having other neurologic or endocrine comorbidities (thyroid disease, cardiovascular disease, high blood pressure, diabetes, cancer, hepatic or renal disorders); taking any nutritional or herbal supplements; having a history of anti-inflammatory or contraceptives drugs at least three months prior to the study; diagnosed as having migraine with aura or other types of headache such as headache due to menstrual cycle tension-type headaches, trigeminal autonomic cephalagia, tension-type headache, medication overuse headache, and cluster headache. Women were also excluded if they adopted a specific physical activity and/or a dietary regimen, severe side effects from the treatment, or poor compliance (less than 80%).
Sample size
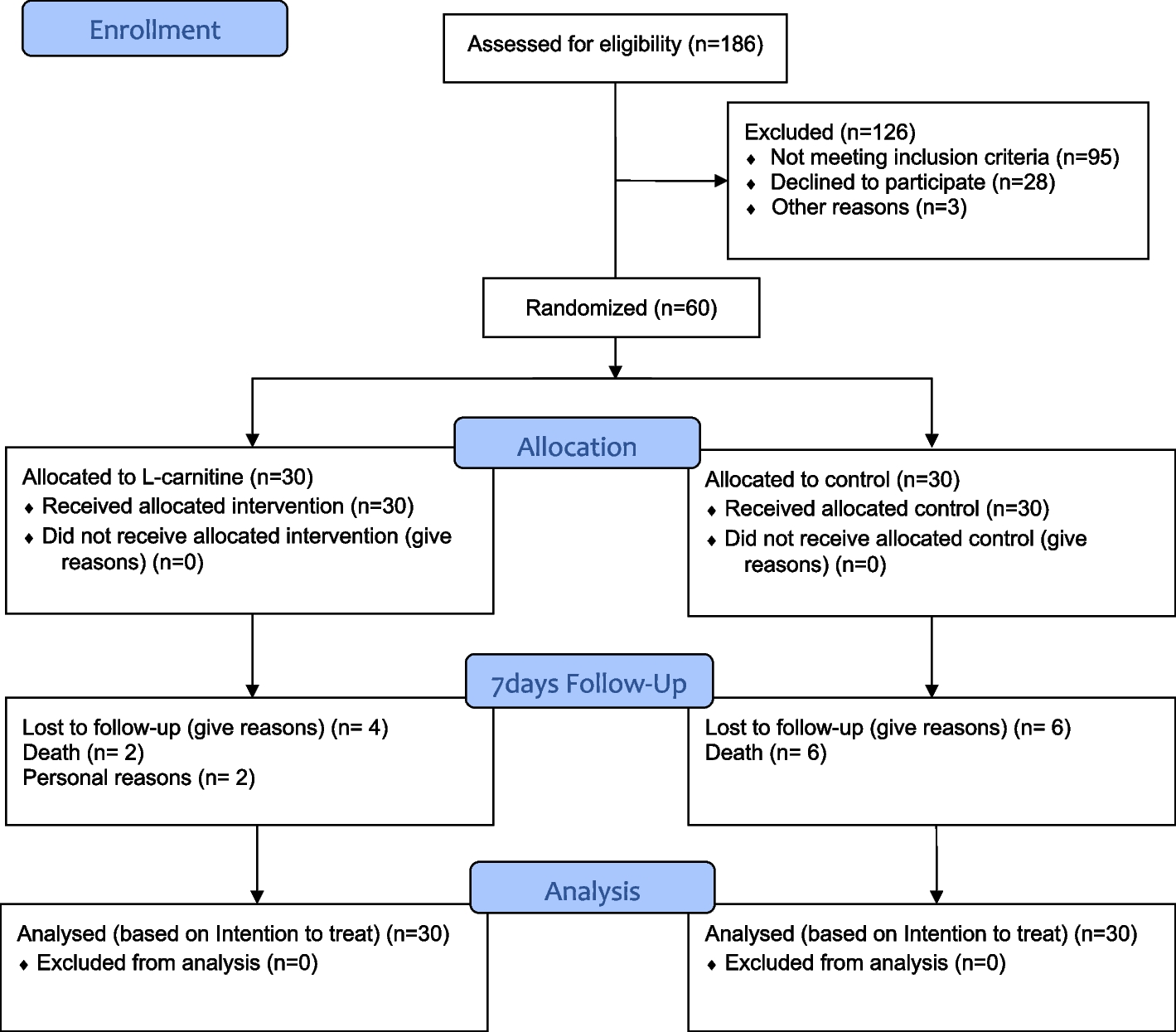
Sample size was determined based on the parallel-two group randomized clinical trial formula with study power of 80%, confidence interval of 95% and based on the severity of attacks [19]. A total of 80 participants (n = 40 per group) was required which was increased to 44 to accommodate a probable 10% dropout rate.
Randomization and blinding
A stratified (based on age and experimental group) permuted block randomization (with block size 4) was performed using a random number table to randomly allocating participants into intervention or placebo groups (1:1). Placebo and isoflavones supplements were boxed and labelled by the supplement manufacturer to ensure blinding. Participants, investigators and laboratory staff were blinded to the treatment assignment.
Intervention
Patients in the intervention group received one tablet containing 50 mg isoflavones (Standardized based on 20–27 mg genistein). Placebo group received starch tablets with similar weight and appearance to intervention tablets. Participants in both groups were instructed to consume one tablet a day for eight weeks. Based on previous studies, a dose of 50 mg was sufficient to induce beneficial effects, with no significant gastrointestinal discomfort or adverse side effects [20]. Participants were provided with a sufficient supply of supplements at baseline and each follow-up visit. Isoflavones and placebo supplements were produced and packaged by Goldaru pharmaceutical company, Isfahan, Iran. The investigators and participants remained blinded to treatment allocation. To increase compliance rate, all patients received weekly phone calls during the two months of the intervention. They returned unused supplement packages as an estimate of compliance. The compliance was calculated based on the following formula: Compliance rate: (Tablet taken/Tablet prescribed) *100. All participants were instructed to continue their routine physical activity, dietary intake, and medication throughout the study but not to consume any soy products. They were also advised to inform the researchers of any changes to their therapy or adverse effects of the supplements.
Assessment of migraine attacks characteristic
Migraine attack characteristics of participants at baseline and the end of the intervention were collected using a self-administered 30-day headache diary. Verbal and written instructions on how to complete the diary were provided. Participants were asked to record the time of migraine attack onset, duration, and severity of the attack (scored from 0 “no pain” to 10 “the worst imaginable pain” based on a visual analog scale (VAS) after each migraine attack regardless of the time of day. The frequency of attack was also recorded as the number of headaches per month. Clinical symptoms of migraine including migraine index (MI), headache diary result (HDR) and migraine headache index score (MHIS) were then calculated using the following formula: MI = frequency × severity; HDR = frequency × duration; and MHIS = frequency × duration × severity [21].
Assessment of mental status & quality of life assessment
To assess the quality of life of migraine patients, the study completed the migraine-specific quality of life (MSQ) questionnaire for each patient. It included 14 questions and assessed the quality of life of patients during the previous month. Each question was scored with a six-choice answer categorized as 1 (never) to 6 (always). All responses were summed to compute an overall score ranging from 14 to 84. To facilitate interpretation, scores were transformed to a scale of 0 to 100 and then they were reduced from 100. Finally, higher scores indicated a better quality of life The validity of the questionnaire has been examined by Zandifar et al. in Iran [22].
DASS (Depression Anxiety and Stress Scale) questionnaire was completed for each person to assess depression, stress, and anxiety. This questionnaire had 21 phrases. Each subscale of depression, stress and anxiety was evaluated by 7 different phrases. The questionnaire had been validated in previous studies[23]
Blood collection and biochemical measurements
A 10 ml blood sample was collected from each participant by a trained phlebotomist at the baseline and end of the intervention. After centrifuging the blood samples for 10 min at 2500 rpm (Beckman Avanti J-25; Beckman 174 Coulter, Brea, CA, USA) at room temperature, serum samples were stored at -80ºC until analysis. The serum levels of CGRP was measured by ELISA (Crystal Day Bio-Tec, China).
Body weight and blood pressure assessment
After screening based on eligibility criteria, participants were asked to complete a questionnaire on the sociodemographic and medical history. Body weight and height were determined with a digital Seca scale (Saca 831, Hamburg, Germany) and a portable stadiometer (Seca, Hamburg, Germany), respectively. Body mass index (BMI) was calculated as weight (kg) divided by the square of the height (m2). SBP and DBP measurements were made, in the right arm, with a conventional mercury sphygmomanometer and an appropriately sized cuff, after the participant seated and rested for 10 min. Two measurements were done at least 30 s apart and the average of the two measurements was used for analyses.
Assessment of diet and physical activity levels
A reliable and valid 3-day food record including two weekdays and 1 weekend during a week, was collected from each participant at baseline and the end of the study to calculate the total energy and nutrients intake relative to migraine. A trained nutritionist blinded to the treatment assignment instructed participants on how to complete their 3-day food record. Dietary intake was then converted to gram/day using Iranian Household Measures. To calculate daily energy and nutrient intake, the Nutritionist IV software (based on the US National Nutrient Databank) modified for Iranian foods was used. The validated Iranian version of the international physical activity questionnaire (IPAQ), was used to compute the level of PA [24]. PA levels were reported as metabolic equivalent hours per day (MET/h/day).
Statistical analysis
The analyses were conducted on the basis of an intention-to-treat (ITT) approach by using the last value carried forward (LOCF) protocol. The ITT analysis included all patients randomly assigned to isoflavones and placebo groups, regardless of their level of adherence to the trial or withdrawal. Following LOCF protocol, the last available measurements for individuals prior to withdrawal from the study were included in the analysis [25]. Shapiro Wilk test was used to assess the normal distribution of data. Data was reported as mean and Standard Deviation (SD) (for continuous data) and frequency and percentage (for categorical data). To compare qualitative variables, the chi-square test was used and expressed as a number (%). To identify between-group differences, independent sample t tests and for within-group differences paired-sample t tests were performed. All quantitative variables were shown as mean ± SD. Analysis of covariance (ANCOVA) was performed to detect differences between two groups adjusted for baseline value. A P-value < 0.05 was considered statistically significant. All statistical analyses of the trial were done by Statistics specialist (Z.H) using SPSS software version 22 (SPSS Inc., Chicago, Illinois).

留言 (0)