
記住我
Ovarian serous carcinoma has traditionally been graded as well, moderately, and poorly differentiated, suggesting that it is a homogeneous disease from the standpoint of pathogenesis. Multiple different grading systems have been used with variable results (reviewed by Silverberg1), including the International Federation of Gynecology and Obstetrics (FIGO) system based on percentage of solid architecture, the World Health Organization system based on an impression of architecture and cytologic features, the Gynecologic Oncology Group (GOG) system based on histologic type, a system based on a combination of mitotic index and volume percentage of epithelium, a system based on presence/amount of hyperchromatic giant nuclei and solid or cribriform architecture, and a grading index based on a mean of the individual scores for architectural pattern, nuclear pleomorphism, nucleoli, nuclear-to-cytoplasmic ratio, mitotic index, pattern of invasion, capsule penetration, and vascular invasion. A 3-tier grading scheme that has gained much attention over the past several years is the universal grading system, which is also referred to as the Silverberg grade.2 In this system, points are assigned for each of 3 components: architecture (glandular, papillary, or solid), degree of nuclear atypia, and mitotic index. The points for each component are added, resulting in a total score which determines the grade, analogous to that used for breast carcinoma.
More recently, a 2-tier grading system specifically for serous carcinoma, in which tumors are subdivided into low grade and high grade, has been proposed. Seminal clinicopathologic and molecular genetic studies from The Johns Hopkins Hospital and M.D. Anderson Cancer Center have shown that a 2-tier grading system is easy to apply, reproducible, and based on underlying molecular biologic differences between low-grade and high-grade tumors.3–24 The purpose of this review is to provide an update on the pathogenesis and clinicopathologic and immunohistochemical features of ovarian low-grade and high-grade serous carcinomas, and to demonstrate why the fundamental differences between both categories of tumors support a 2-tier classification system. In addition, selected diagnostic problems are addressed.
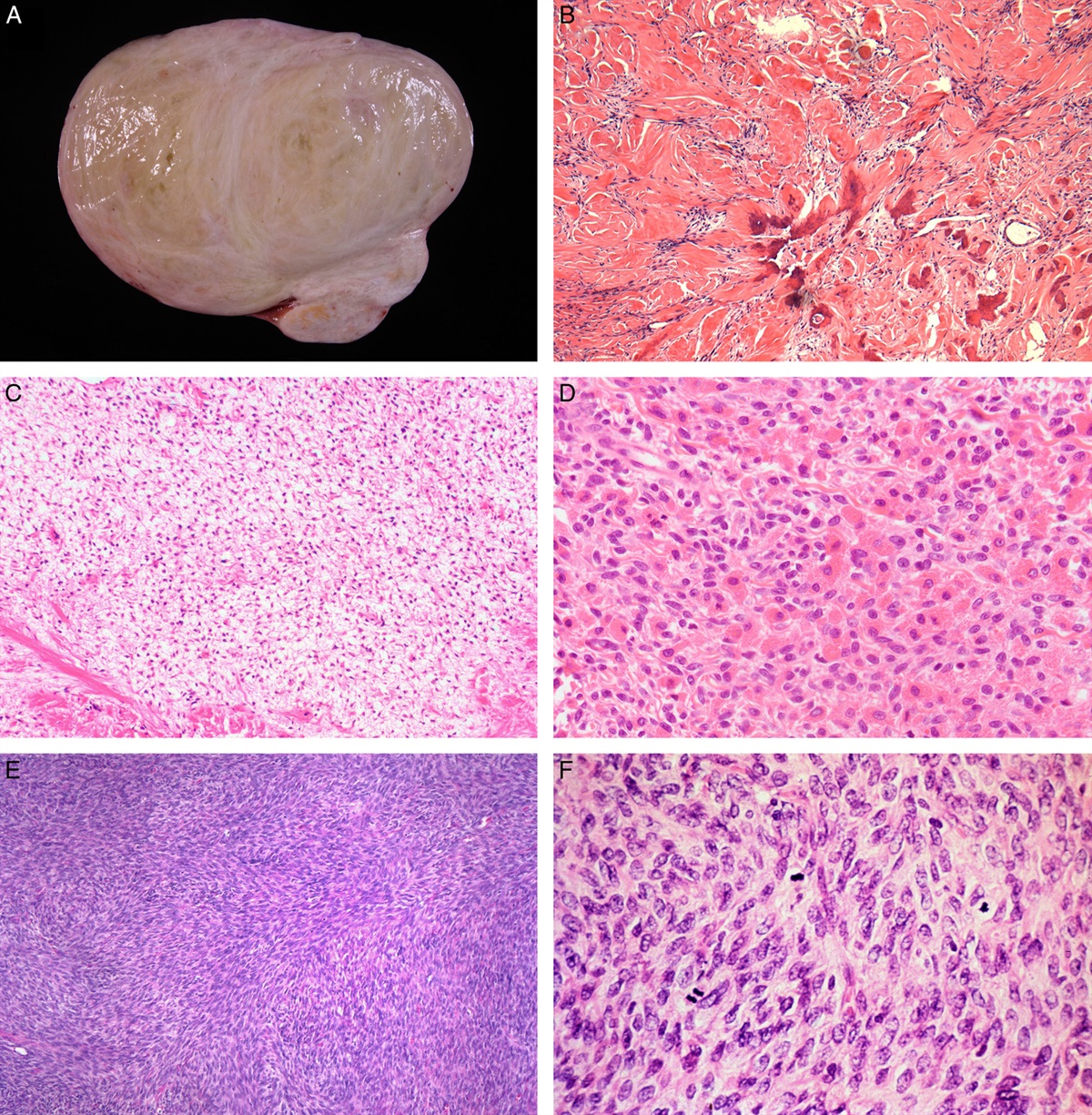
PATHOGENESIS Low-grade Serous Carcinoma (Table 1)Low-grade serous carcinoma [invasive micropapillary serous carcinoma (MPSC)], has been hypothesized to arise from a serous cystadenoma (Fig. 1A) or adenofibroma, which progresses to an atypical proliferative serous tumor (APST) (typical serous borderline tumor) (Fig. 1B), to noninvasive MPSC (micropapillary serous borderline tumor) (Fig. 1C), and then to invasive MPSC in a slow step-wise fashion. This has been described as the Type I pathway and is supported by several morphologic observations. First, invasive low-grade serous carcinoma is associated with noninvasive MPSCs in over three-fourths of the cases (Fig. 1D).10 Second, in occasional tumors, the level of differentiation of the noninvasive tumor is intermediate between APST and noninvasive MPSC, suggesting a morphologically intermediate step. Third, true early invasion in an APST or noninvasive MPSC resembles low-grade serous carcinoma (Fig. 1E).4,23,25,26 Fourth, in several studies, noninvasive MPSCs have a higher frequency of invasive implants (Fig. 1F) compared with APST, and these implants are histologically identical to low-grade serous carcinoma.27,28
 FIGURE 1.:
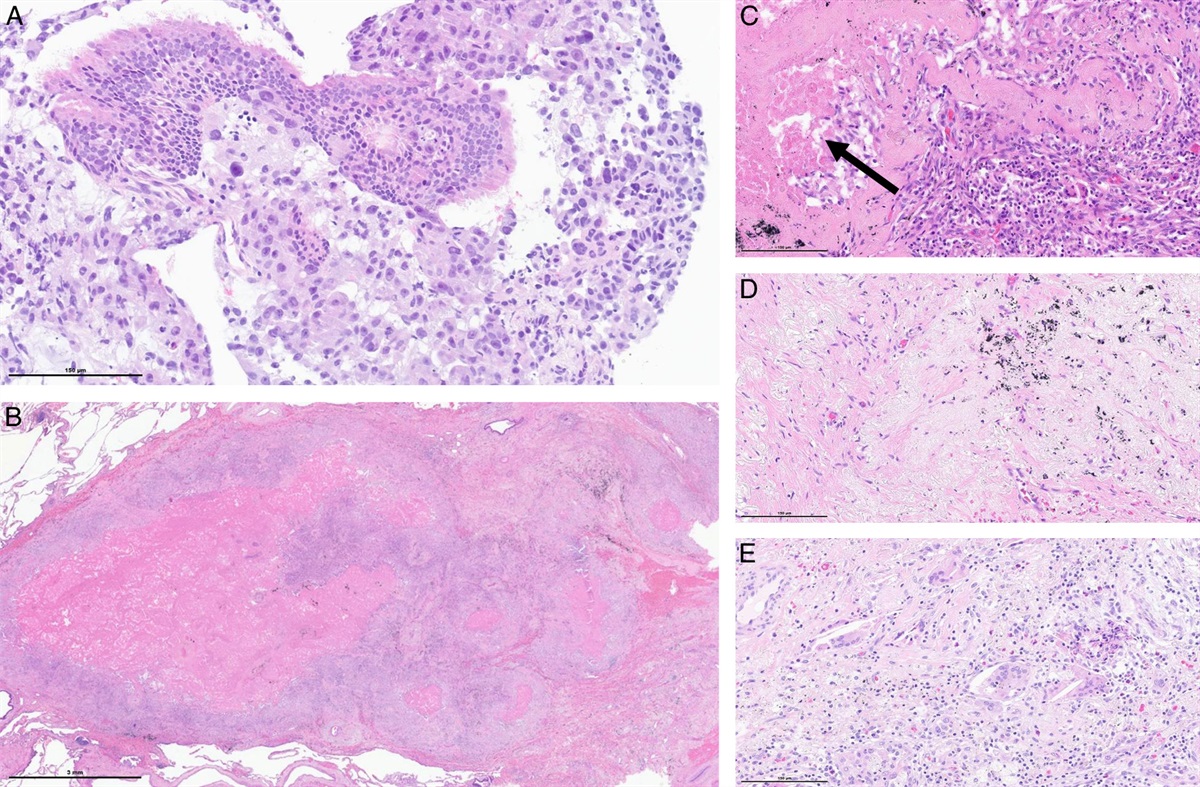
FIGURE 1.: Proposed model of pathogenesis of low-grade serous carcinoma. A, Small atypical proliferative serous tumor (APST) arising in a serous cystadenoma. B, APST. C, Noninvasive micropapillary serous carcinoma (MPSC). D, Tumor progression in the ovary results in invasive MPSC (lower); background of noninvasive MPSC in upper half of the figure. E, Microinvasion (upper left), which is qualitatively identical to low-grade serous carcinoma, arising within a noninvasive MPSC (lower right). F, Invasive implants in the peritoneum are histologically identical to low-grade serous carcinoma.
 TABLE 1:
TABLE 1: Pathogenesis of Low-grade Versus High-grade Ovarian Serous Carcinoma
Both low-grade serous carcinoma and APST/noninvasive MPSC are characterized by mutations of the KRAS, BRAF, or ERBB2 genes, in which approximately two-thirds of tumors have a mutation of one of these genes.19–21,29–32 However, KRAS and BRAF are much more commonly mutated than ERBB2. Mutations of each of these 3 genes are mutually exclusive; thus, a tumor with a KRAS mutation will not have a mutation of the other 2 genes, and vice versa.
KRAS, BRAF, and ERBB2 are upstream regulators of mitogen-activated protein kinase (MAPK). Mutations of any of these genes result in constitutive activation of the MAPK signal transduction pathway, which in turn leads to uncontrolled proliferation.33 In contrast to high-grade serous carcinoma, TP53 mutations are uncommon (8%) in low-grade serous carcinoma.22 Identical mutations of either KRAS or BRAF have been observed in the epithelium of cystadenomas adjacent to the APSTs indicating a shared lineage and suggesting that mutation of KRAS or BRAF is an early event in the transition from a cystadenoma to an APST.34 Serous cystadenomas that do not contain APSTs do not harbor KRAS or BRAF mutations.
Both APST and noninvasive MPSC share several allelic imbalances on multiple chromosomal arms (1p, 5q, 8p, 18q, 22q, and Xp); however, many of these are slightly more frequent in noninvasive MPSC, and some (gain of 16p) are unique to noninvasive MPSC.19,35 Similarly, the multiple shared allelic imbalances are more frequent in low-grade serous carcinoma.19 Thus, the number of allelic imbalances progressively increase from APST to noninvasive MPSC to low-grade serous carcinoma. This gradual chromosomal instability associated with the Type I pathway is in contrast with the high level of chromosomal instability seen in high-grade serous carcinomas.19,35 Gene expression profiling has also shown that invasive MPSC is more closely related to APST/noninvasive MPSC than high-grade serous carcinoma.36
In a recent study, Kuo et al9 assessed DNA copy number changes among affinity-purified tumor cells from ovarian serous neoplasms, including serous borderline tumors, low-grade serous carcinomas, and high-grade serous carcinomas, using high-density 250 K single nucleotide polymorphism arrays. The chromosomal instability indices as measured by changes in DNA copy number were significantly higher in high-grade than in low-grade carcinomas. Hemizygous ch1p36 deletion was common in low-grade serous carcinomas but rarely seen in serous borderline tumors. This region contains several candidate tumor suppressors, including miR-34a.
The morphologic and molecular observations link each of these lesions and provide compelling evidence for the step-wise progression from cystadenomas to low-grade serous carcinoma, and this process is distinctly different from that of high-grade serous carcinoma. This pathway is akin to the adenoma-carcinoma sequence seen in the model of pathogenesis of colorectal carcinoma or hyperplasia-carcinoma sequence in endometrioid carcinoma of the endometrium.
High-grade Serous Carcinoma (Table 1)Much less is known about the pathogenesis of ovarian high-grade serous carcinoma compared with low-grade serous carcinoma. Unlike low-grade serous carcinoma, mutations of KRAS, BRAF, or ERBB2 occur very infrequently in high-grade carcinoma.19–21,30–32,37,38 In contrast, TP53 mutation occurs in 80% of high-grade tumors, and up-regulation and down-regulation of numerous other genes and various DNA copy number changes have been described.9,13,33,36,39,40
Genome-wide analysis of DNA copy number alterations has demonstrated significant numbers of amplifications and deletions, including homozygous deletions.9 Among homozygous deletions, loci containing Rb1, CDKN2A/B, CSMD1, and DOCK4 were most common, being present in 10.6%, 6.4%, 6.4%, and 4.3%, respectively, of 47 affinity-purified high-grade serous carcinomas. Except for the CDKN2A/B region, these homozygous deletions were not present in either serous borderline tumors or low-grade serous carcinomas.
The identification of the precursor lesion of high-grade serous carcinoma has puzzled investigators for decades. As high-grade serous carcinoma nearly always presents with high-stage disease, the development of this tumor is thought to be rapid, and its origin has traditionally been presumed to be from surface epithelium or epithelial inclusions in the ovary. In an effort to detect putative precursors, investigators have focused on ovaries of women with a family history of ovarian cancer and women with BRCA mutations. Increased p53 immunopositivity has been noted in the epithelium of ovaries from these women compared with controls, but these findings have not been confirmed in other studies. Mutations and/or loss of heterozygosity of TP53 have been identified in early carcinomas and epithelial inclusions of the ovary, including identical mutations in the epithelium and adjacent carcinoma in the same cases.41,42 These molecular findings support the role of TP53 mutation as an early event in the pathogenesis of high-grade serous carcinoma and that the origin for some tumors is the surface epithelium or epithelial inclusions of the ovary. Parenthetically, 10% of ovarian carcinomas are hereditary. Of the hereditary carcinomas, most are related to BRCA mutations, which seem to play a role in the pathogenesis of ovarian carcinoma in this subset of tumors. In all, 12% to 15% of women with ovarian carcinoma, and ∼15% of serous carcinomas, in large population-based series from North America have germline mutations of BRCA, either BRCA1 or BRCA2.43,44 Most of the BRCA-related hereditary ovarian tumors are high-grade serous carcinoma. Low-grade serous carcinoma and APST/noninvasive MPSC do not seem to be related to germline mutations of BRCA.
In a report by Werness et al,42 an incidental ovarian carcinoma in situ from a woman with a germline mutation of BRCA1 exhibited loss of heterozygosity of this gene. Also, loss of heterozygosity of BRCA has been demonstrated in epithelial inclusions/surface epithelium in ovaries from prophylactic oophorectomy specimens. Loss of heterozygosity has also been reported in invasive carcinoma and adjacent epithelium in stage I ovarian carcinomas from women with BRCA germline mutations.41 These studies suggest that loss of heterozygosity of BRCA is an early event in high-grade serous carcinoma for tumors with germline mutations. Similar to TP53, BRCA seems to function as a tumor suppressor gene. Thus, patients inherit a germline mutation of BRCA, and with somatic loss of the wild-type allele, carcinoma develops. The exact interaction between mutations of BRCA and TP53 in ovarian carcinoma is unclear. In addition to germline mutations, other molecular alterations leading to inactivation of BRCA include somatic mutation, promoter hypermethylation, and isolated loss of hetrerozygosity.45,46 These putative precursor lesions are detected in inclusions in the ovary or ovarian surface epithelium and are characterized by tubal-type epithelium with varying degrees of cytologic atypia that have been termed dysplasia/carcinoma in situ (reviewed by Bell47). These findings, although they suggest that a morphologically identifiable precursor of high-grade serous carcinoma may exist in the ovary, are very rarely detected, and, therefore, it has been suggested that these tumors arise de novo.48
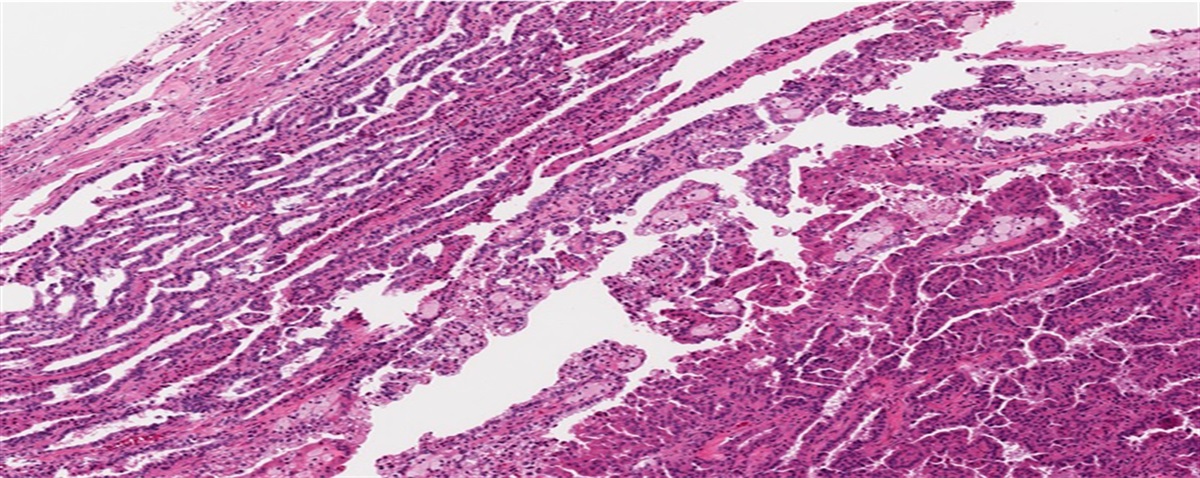
Recently, attention has been drawn to a lesion in the fallopian tube that has the cytologic appearance of high-grade serous carcinoma of the ovary and has been designated tubal intraepithelial carcinoma (TIC) (Fig. 2). These lesions are almost always detected in the fimbriated end of the fallopian tube. The fimbriated end is in close proximity to the ovarian surface, and it has been suggested that the tube is the origin of a subset of “ovarian” high-grade serous carcinomas. This is supported by the following: (1) early serous carcinomas in prophylactic bilateral salpingo-oophorectomy specimens from women with BRCA mutations (ie, women who are at an increased risk for “ovarian” carcinoma) can be detected in the tube, especially the fimbriated end, in the absence of an ovarian tumor, (2) identical TP53 mutations have been reported in TIC and synchronous ovarian high-grade serous carcinomas, and (3) identical TP53 mutations have been reported in TICs and in small foci of histologically normal tubal epithelium that diffusely expresses p53, which has been termed “p53 signature.” It has been suggested that p53 signatures are precursors of TICs, which in turn precede the development of high-grade serous carcinoma.49–55 Moreover, it has been proposed that when there is a synchronous TIC and ovarian high-grade serous carcinoma that the fallopian tube is the primary site of origin for the “ovarian” tumor. In 1 study, all fallopian tube tissue from consecutively accessioned pelvic serous carcinomas was submitted for histologic examination, and 48% of the tumors initially interpreted as ovarian in origin contained a TIC.52 In an analysis of ovarian high-grade serous carcinomas at The Johns Hopkins Hospital in which all tubal tissue was submitted for histologic examination, 45% of cases contained TIC (unpublished data). It has, therefore, been hypothesized that neoplastic cells of TIC, or a small invasive high-grade serous carcinoma in the fallopian tube which developed from TIC, implant on the ovary, developing into a high-grade serous carcinoma that clinically and grossly appears to be an ovarian primary tumor.
 FIGURE 2.:
FIGURE 2.: Tubal intraepithelial carcinoma (TIC). A, The epithelium of the fallopian tube mucosa with TIC is thicker compared with normal mucosa (upper center). B, The neoplastic cells of TIC show enlarged nuclei, increased nuclear-to-cytoplasmic ratios, and coarse chromatin. C, Immunohistochemical stain for p53 showing diffuse strong expression in TIC whereas the normal mucosa is negative. In B and C, single arrow represents normal epithelium, and double arrows represent TIC.
Thus, the morphologic and molecular observations detailed above suggest that possibly half of “ovarian” high-grade serous carcinomas may be of tubal origin. In the other half of tumors, primary origin may have been ovarian or peritoneal. It should be noted that the criteria for distinction of primary ovarian versus peritoneal origin are quite arbitrary. Bona fide well-defined precursor lesions in the ovary are rare and have not been identified in the peritoneum.
In summary, the pathogenesis of high-grade serous carcinoma (Type II pathway) is characterized by: (1) rapid development from what are now believed to be intraepithelial carcinomas very likely of tubal origin, (2) TP53 mutations, (3) a high level of chromosomal instability, (4) in hereditary tumors, BRCA germline mutations, and (5) absence of mutations of KRAS, BRAF, or ERBB2.
Development of High-grade (Type II) From Low-grade (Type I) Serous CarcinomaThe Type I and Type II pathways of development of low-grade and high-grade serous carcinomas are generally independent. Furthermore, when low-grade serous carcinomas recur, they typically maintain their low-grade appearance throughout multiple recurrences, supporting the view that high-grade serous carcinoma does not progress from low-grade serous carcinoma. However, infrequent high-grade serous carcinomas seem to have evolved from a low-grade tumor (Fig. 3). Two percent of high-grade serous carcinomas in the series by Malpica et al10 were associated with a serous borderline tumor. Another case of high-grade serous carcinoma arising within a serous borderline tumor has been reported elsewhere.56 In a report by Parker et al,57 2 women with serous borderline tumors recurred as high-grade serous carcinoma.
 FIGURE 3.:
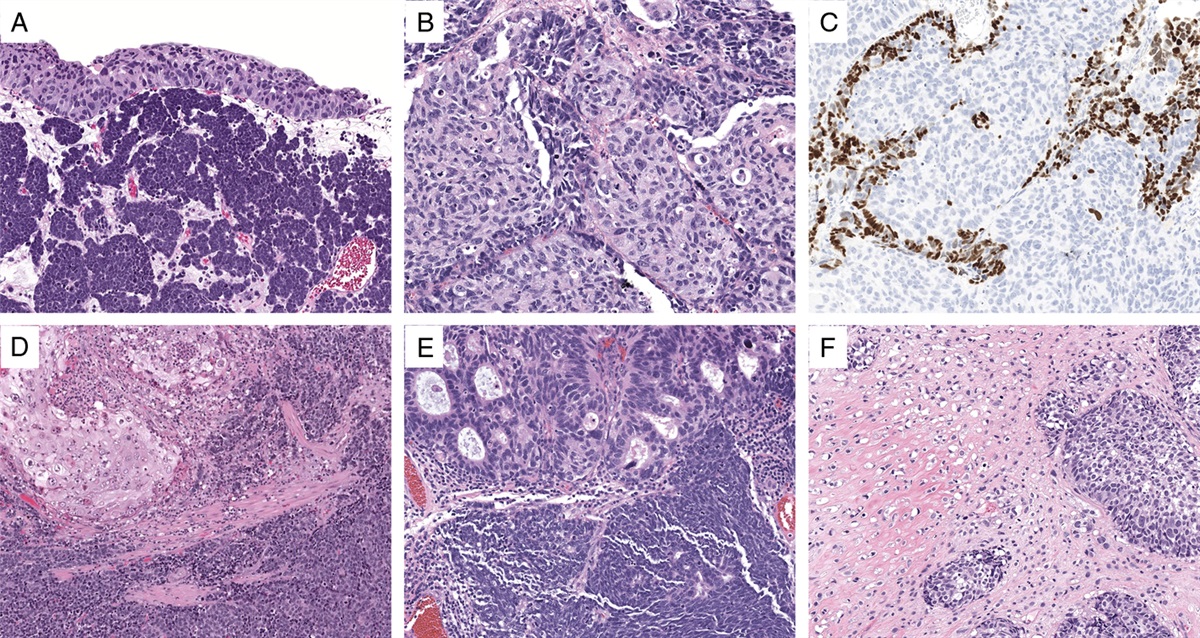
FIGURE 3.: High-grade serous carcinoma arising in a background of low-grade serous carcinoma. A and B, Low-grade component. C and D, High-grade component.
At The Johns Hopkins Hospital (both in-house and consultation cases), 3% of serous carcinomas contained both high-grade and low-grade components. The latter were either APST (3 cases) or invasive carcinoma (3 cases).5 In 4 of the 6 cases, a morphologic continuum could be identified between the low-grade and high-grade components. Two of the 6 cases contained identical KRAS mutations in both the low-grade and high-grade components. The other 4 cases lacked KRAS mutations in both components, and all 6 cases did not have BRAF or TP53 mutations in either component. The finding of identical KRAS mutations in both components establishes a clonal relationship between the low-grade and high-grade tumors in those 2 cases. The remaining 4 cases were molecularly uninformative as they did not have mutations for comparison in either component. However, the lack of TP53 mutations in all 6 cases contrasts with the high frequency of mutations typically seen in high-grade serous carcinoma (80%). These observations suggest that a very small minority of high-grade serous carcinomas may evolve from an APST, a noninvasive MPSC, or a low-grade serous carcinoma.
It should be noted that the high-grade serous carcinomas that seem to have evolved from low-grade serous tumors (Type I tumors) do not differ morphologically from those that developed along the Type II pathway. In particular, a high-grade serous carcinoma with a micropapillary pattern does not necessarily indicate origin from a low-grade tumor, as such tumors have been shown to lack KRAS mutations and exhibit TP53 mutations.3,21 In future studies, it will be important to evaluate whether both types of high-grade serous carcinomas (those with mutated KRAS or BRAF and wild-type TP53 vs. those with wild-type KRAS and BRAF and mutated TP53) have a different clinical outcome and/or response to chemotherapy.
CLINICAL ASPECTS, HISTOLOGIC FEATURES, AND SELECTED DIAGNOSTIC PROBLEMS Low-grade Serous Carcinoma (Table 2)Patients with low-grade serous carcinoma are younger than those with high-grade tumors, with mean ages of 45 to 57 years and 55 to 65 years, respectively.6,10,58 Almost all patients in both groups present with advanced stage disease, and the majority of low-grade and high-grade tumors are bilateral.
 TABLE 2:
TABLE 2: Clinicopathologic Features of Low-grade and High-grade Serous Carcinomas
Low-grade serous carcinoma (invasive MPSC) accounts for a small proportion of all ovarian serous carcinomas. In the series by Seidman et al,58 in which the 2-tier system was used, 9% of serous carcinomas were low grade. In other large series using the 3-tier universal grading system, 6% to 22% of serous carcinomas were grade 1.2,59
Low-grade and high-grade serous carcinomas in the 2-tier system correspond to grade 1 and grade 2 or 3, respectively, in the universal grading system. In the series by Malpica et al,10 94% of low-grade serous carcinomas were grade 1 in the universal grading system, and the remaining 6% were grade 2. Likewise, all high-grade serous carcinomas were grade 2 or 3. Conversely, all grade 1 tumors in that study were low grade, and 94% of all grade 2 or 3 tumors were high grade.
Low-grade serous carcinoma is frequently associated with a noninvasive component–either serous adenofibroma, APST, or noninvasive MPSC (Fig. 1D). The noninvasive component may be absent, but when present, it can vary from focal to extensive. The invasive component is characterized by micropapillae and small round nests of cells that infiltrate the stroma in a haphazard pattern (Figs. 4A, B). The micropapillae are small and either lack fibrovascular cores or have very thin, delicate fibrovascular cores. The micropapillae and small solid nests of cells are frequently surrounded by a clear space or cleft (Fig. 4B). In tumors with marked architectural complexity, the micropapillae can anastomose with one another, forming thin, elongated, and branching structures (Fig. 4C). The surface of the micropapillae may be smooth or irregular due to hobnail cells. Occasionally, papillae are larger and contain broad fibrous cores (Fig. 4D). Rarely, other nonmicropapillary invasive components include small-sized to medium-sized simple glands. The medium-sized and large-sized papillae and glands, if present, typically account for only a small proportion of the tumor and are intimately admixed within the micropapillary-rich component. Psammoma bodies are common and may be numerous (Fig. 4D). Necrosis or multinucleated tumor giant cells are not features of low-grade serous carcinoma.
 FIGURE 4.:
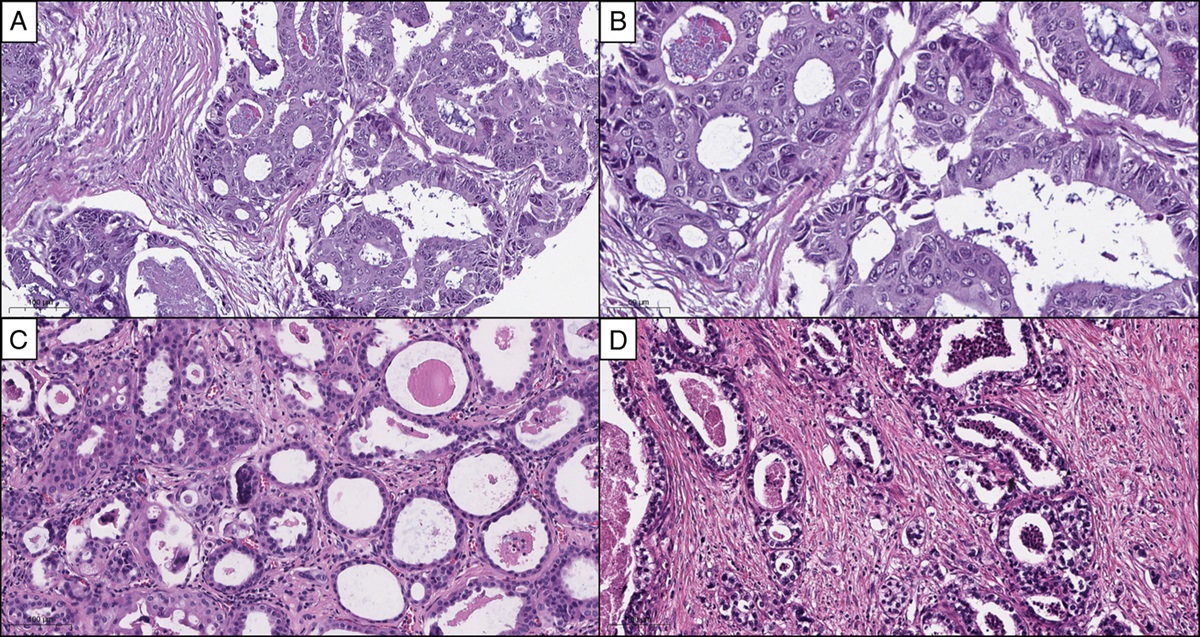
FIGURE 4.: Low-grade serous carcinoma. A and B, Carcinoma invades stroma and is composed of small micropapillae. B, The papillae either lack fibrous cores or contain thin attenuated fibrous cores and are surrounded by clear spaces. C, In some instances, the papillae fuse to form anastamosing patterns. D, Larger papillae may be seen. Psammoma bodies are also present. E, The nuclei of the micropapillae are small, uniform, and round, with evenly dispersed chromatin and small nucleoli.
The neoplastic cells can have either scant cytoplasm or a moderate amount of eosinophilic cytoplasm. However, the nuclear-to-cytoplasmic ratio may be high, and the nuclei are uniform, small, and round to oval. The chromatin is even and does not exhibit hyperchromasia. Small nucleoli may be present. Only mild variation in size and shape of nuclei are tolerated for a designation of low-grade serous carcinoma (Fig. 4E). Per the criteria in the study by Malpica et al,10 tumors with cells showing ≥3:1 variation in nuclear size and shape are classified as high-grade serous carcinoma. In that study, most low-grade serous carcinomas had a mean mitotic index of 4 mitotic figures per 10 high-power fields (range, 1-12 MFs/10 HPFs). In our practice, we do not employ mitotic counts for the distinction of low-grade from high-grade serous carcinoma. Rather, we consider low-grade serous carcinoma as having only infrequent mitotic figures whereas high-grade serous carcinoma has readily identifiable mitotic activity.
Excellent interobserver and intraobserver reproducibility of the 2-tier low-grade/high-grade system has been demonstrated. In a study by Malpica et al,11 80 serous carcinomas, including 40 low-grade and 40 high-grade tumors per the original diagnosis, were evaluated among 9 pathologists with 2 rounds of review. In the first and second rounds of review, all pathologists agreed on grade in 75% and 84% of tumors, respectively. In the first round of review, the κ values for agreement between different reviewers ranged from 0.717 to 1.000, and the range in the second round was 0.701 to 1.000. The intraobserver reproducibility yielded κ values ranging from 0.725 to 1.000. All of the κ values in this study were in the good to excellent range. These findings confirm the ease and reproducibility of using the 2-grade system in routine practice.
A potential pitfall in the evaluation of low-grade serous tumors of the ovary is that some low-grade serous carcinomas exhibit an inverted “macropapillary” form of invasion, which can be misdiagnosed as serous adenofibroma (Fig. 5). Such variants of low-grade serous carcinoma are characterized by a haphazard infiltration of medium-sized round papillae surrounded by a clear space. These types of papillae, in contrast to micropapillae of conventional low-grade serous carcinoma, contain a fibrous stromal core; however, they are lined by the same type of neoplastic epithelium as seen in the classic micropapillae. We previously reported our experience with 14 cases of this macropapillary variant of low-grade serous carcinoma.60 The ovarian tumor in such cases contained a background of either APST, noninvasive MPSC, and/or conventional low-grade serous carcinoma. The macropapillary component accounted for 20% to 100% of the entire invasive component in the ovarian tumors. Three of the 9 cases with extra-ovarian disease had macropapillae in extra-ovarian sites. Molecular analysis was performed on 7 tumors, and in 4, both the macropapillary and micropapillary components contained identical KRAS mutations. In one of these tumors, the same KRAS mutation was also present in macropapillae in a lymph node metastasis. In another tumor, identical BRAF mutations were present in the macropapillary and micropapillary components. Two tumors contained wild-type KRAS and BRAF and were, therefore, molecularly uninformative. These morphologic and molecular findings support the interpretation that the macropapillary component is a form of low-grade invasive carcinoma.
 FIGURE 5.:
FIGURE 5.: Low-grade serous carcinoma with inverted macropapillary pattern. A and B, The invasive papillae are medium to large in size, haphazardly arranged, and surrounded by clear spaces. The papillae are lined by cells with low-grade nuclei similar to those in the conventional micropapillary pattern.
High-grade Serous Carcinoma (Table 2)High-grade serous carcinomas may exhibit mixtures of papillary, glandular, nested, and diffuse/solid growth patterns although any component may predominate in a given tumor (Figs. 6A–C). The papillae tend to be large and complex. The epithelium lining the papillae is usually stratified with an irregular slit-like configuration (Fig. 6A). Although a micropapillary growth pattern is typical of low-grade serous carcinoma, it should be emphasized that occasional high-grade carcinomas can also exhibit this architecture (Fig. 6D); however, they have high-grade nuclei and typically have an admixed solid growth pattern. The latter would be unusual for low-grade tumors. The glands in high-grade serous carcinoma may be round and simple or complex with irregular slit-like spaces (Fig. 6B). Some tumors may have such extensive solid architecture with diffuse sheets of neoplastic epithelium that a careful search for a glandular or papillary component may be necessary for distinction from undifferentiated carcinoma. Obvious destructive stromal invasion is generally present, but some neoplasms may be predominantly intracystic and, therefore, misdiagnosed as APST/noninvasive MPSC. The presence of high-grade nuclei excludes that possibility. Necrosis is common in high-grade serous carcinoma. Psammoma bodies can be seen but are typically less frequent compared with low-grade serous carcinoma.
 FIGURE 6.:
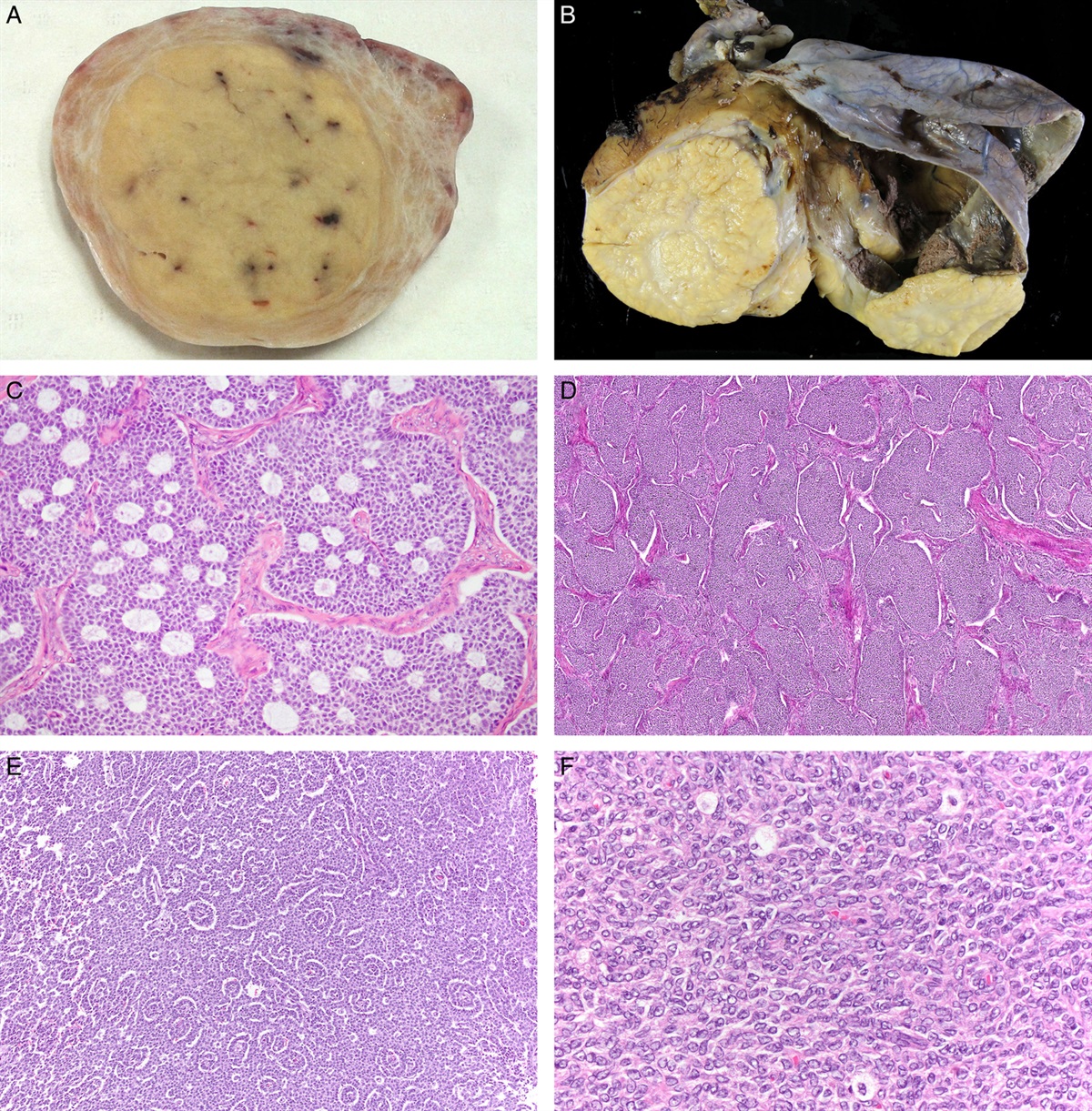
High-grade serous carcinoma. A, Typical papillary pattern showing irregular slit-like spaces. B, Glandular pattern. C, Diffuse, solid pattern. D, Micropapillary pattern. E, In contrast to low-grade serous carcinoma (Fig. 4E), the nuclei of high-grade serous carcinoma are larger with greater pleomorphism and larger nucleoli. F, Endometrioid carcinoma-like pattern. G, Serous carcinoma with clear cytoplasm. H, Transitional cell carcinoma-like pattern. I, Signet ring change simulating signet ring cells of metastatic adenocarcinoma involving the ovary.
FIGURE 6.:
High-grade serous carcinoma. A, Typical papillary pattern showing irregular slit-like spaces. B, Glandular pattern. C, Diffuse, solid pattern. D, Micropapillary pattern. E, In contrast to low-grade serous carcinoma (Fig. 4E), the nuclei of high-grade serous carcinoma are larger with greater pleomorphism and larger nucleoli. F, Endometrioid carcinoma-like pattern. G, Serous carcinoma with clear cytoplasm. H, Transitional cell carcinoma-like pattern. I, Signet ring change simulating signet ring cells of metastatic adenocarcinoma involving the ovary.The neoplastic epithelial cells are heterogeneous and may be a mixture of low cuboidal, columnar, and hobnail shapes. Typically, there is marked variation in size and shape. The nuclear-to-cytoplasmic ratios are generally high, but at times, abundant eosinophilic cytoplasm is present. Most tumors have variable combinations of enlarged round or oval nuclei, irregular nuclear membranes, irregular chromatin distribution, hyperchromasia, large nucleoli, and abundant mitotic figures, including atypical forms (Fig. 6E). In the study by Malpica et al,10 the median mitotic index was 38 mitotic figures per 10 high-power fields (range, 14-137 MFs/10 HPFs). Bizarre mononuclear or multinucleated tumor giant cells are common (Figs. 3C, D).
At times high-grade carcinomas can display an appearance, mimicking endometrioid carcinoma (Fig. 6F). When the glands have irregular serrated luminal contours, large complex papillae lined by stratified epithelium with irregular slit-like patterns, hobnail cells, bizarre tumor giant cells, and psammoma bodies, a serous carcinoma is favored. In contrast, tumors with peripheral palisading of solid islands and nests, squamous metaplasia, or a background of atypical proliferative (borderline) endometrioid tumor or endometriosis favor high-grade endometrioid carcinoma. Immunohistochemical staining for Wilms' tumor suppressor gene-1 (WT-1) has been advocated as useful for this differential diagnosis, but in our experience it is not reliable. At times, distinction of high-grade serous carcinoma from high-grade endometrioid carcinoma (FIGO grade 2 or 3) is not possible, and classification as “high-grade adenocarcinoma, not otherwise specified” with a descriptive comment is necessary.
Some tumors may contain cells with clear cytoplasm. If the tubulocystic and papillary patterns characteristic of clear cell carcinoma are not present, these tumors should not be interpreted as clear cell carcinoma (Fig. 6G). When the epithelium lining surface of large rounded papillae is smooth, a transitional cell carcinoma (TCC)-like appearance can be produced and may be mistaken for ovarian TCC (Fig. 6H). Opinions vary among gynecologic pathologists as to whether pure TCC of the ovary is a distinctive entity or simply a TCC-like pattern of high-grade serous carcinoma. At present, the “jury is still out.” Glandular differentiation has been described in transitional cell carcinoma; however, a diagnosis of serous carcinoma is favored when the glands merge with complex, branching papillae exhibiting epithelial tufting and solid nests surrounded by a space and irregular slit-like spaces are present. Also, psammoma bodies are more typical of serous carcinoma. Immunohistochemistry is not helpful as WT-1 expression has been described in both serous and transitional cell carcinomas.
Rarely, microcystic or signet ring cell-like change can be seen in high-grade and also in low-grade serous carcinoma (Fig. 6I).61 Microcystic change in such tumors is produced by the presence of back-to-back cells with signet ring change and can simulate the reticular pattern of yolk sac tumor. The combination of older age, bilaterality, large papillae lined by complex and stratified epithelium, glands with irregular slit-like spaces, and psammoma bodies favors serous carcinoma. On the other hand, the combination of younger age, unilaterality, microcystic patterns which blend with other classic patterns of yolk sac tumor, such as Schiller-Duval bodies, polyvesicular-vitelline, intestinal, and myxoid patterns, and hyaline globules favors yolk sac tumor. An elevated serum α-fetoprotein level is characteristic of yolk sac tumor. Immunohistochemistry may be helpful in that expression of WT-1, estrogen receptor (ER), progesterone receptor (PR), cytokeratin 7, and epithelial membrane antigen are more frequent in serous carcinoma whereas expression of α-fetoprotein and absence of the other markers listed above are more typical of yolk sac tumor.
The distinction of low-grade from high-grade serous carcinoma is based on nuclear features, as described by Malpica et al,10 and detailed above. In most tumors, the nuclei of low-grade and high-grade serous carcinomas are typically grade 1 and grade 3, respectively, in a 3-tier system; thus, the diagnosis in most of the tumors is straightforward. Some tumors (approximately 4% of serous carcinomas3), however, exhibit nuclear features that are intermediate between low grade and high grade. These “grade 2” nuclei are larger and have coarser chromatin, more mitotic activity, and larger nucleoli than grade 1 nuclei. They are also relatively uniform and are smaller and less pleomorphic and have less coarse chromatin than grade 3 nuclei (Fig. 7). Thus, classification of these tumors with intermediate-grade nuclei as low-grade versus high-grade serous carcinoma will be difficult.
 FIGURE 7.:
FIGURE 7.: High-grade serous carcinoma with “grade 2 nuclei.” A and B, The nuclei are more uniform and smaller than in typical high-grade serous carcinomas but larger than low-grade serous carcinoma. The combination of (B) slightly increased variation in nuclear size, coarser chromatin, nucleolar prominence, and increased mitotic activity (arrows), (C) abnormal mitotic figures, and (D) necrosis allows for distinction from low-grade serous carcinoma.
In a previous study, we analyzed 11 serous carcinomas with “grade 2” nuclei.3 All 10 with staging data were FIGO stage IIIC. A significant micropapillary pattern was present in 6 (55%). Five (45%) had multiple small foci of necrosis. The mean mitotic index was 11 mitotic figures per 10 high-power fields (range, 4 to 18 MFs/10 HPFs). Molecular analysis was performed in all 11 tumors. None contained KRAS, BRAF, or ERBB2 mutations, but TP53 mutations were identified in 10 (91%). Of these 10 with follow-up, 7 patients died of disease at 6 to 30 months, 2 died of other causes, and 1 had no evidence of disease at 6 months. The clinicopathologic and molecular findings support grading tumors with intermediate-grade nuclei as high-grade serous carcinoma. It should be noted that these tumors with intermediate-grade (grade 2) nuclei are not synonymous with the rare high-grade serous carcinomas that truly have an admixed component of low-grade serous carcinoma (Fig. 3). See Development of High-grade (Type II) from Low-grade (Type I) Serous Carcinoma in Pathogenesis above for additional details.
High-grade serous carcinomas are architecturally heterogeneous, in that they correspond to moderately differentiated and poorly differentiated grades in 3-tier grading systems because some are predominantly papillary or glandular whereas others are mostly solid. However, they do not seem to be different from a molecular and in vitro drug resistance standpoint. In a study of high-grade serous carcinomas in which moderately differentiated and poorly differentiated were compared, there were no significant differences in the frequency of TP53 mutation or extreme drug resistance for each of 10 chemotherapeutic agents.24 In addition, the survival for patients with grades 2 and 3 serous carcinomas using the universal grading system is closer to each other compared with survival for patients with grade 1 and 2 tumors.10,62 These biologic and clinical findings suggest that moderately and poorly differentiated tumors can be combined into a single category, justifying the use of a 2-tier rather than a 3-tier grading system.
BehaviorThe few studies that have compared outcome between both types of serous carcinomas using the 2-tier system have shown that patients with low-grade tumors have better survival. In the study by Malpica et al, the 2-tier grading system was found to be of independent prognostic significance upon multivariate analysis, and the survival of patients with low-grade tumors was significantly higher than with high-grade tumors.10 In that study, death due to disease was more rapid with high-grade carcinoma. The median survival was 1.7 years for patients with high-grade tumors compared with 4.2 years for women with low-grade tumors. Furthermore, in a large clinical study of only low-grade serous carcinoma, the median overall survival with stage III or IV disease was 6.8 years. Persistent disease after primary chemotherapy was the only variable associated with shorter survival time.6 With high-grade serous carcinoma, survival beyond 5 years is unusual, but survival over 10 years can be seen in a subset of low-grade serous carcinomas. The 5-year survival rates for low-grade and high-grade tumors in the study by Malpica et al were 40% and 9%, respectively.10 In the study by Seidman et al58 in which the criteria for the 2-tier system of Malpica et al10 were used, the 5-year survival rates for low-grade and high-grade serous carcinomas were 56% and 34%, respectively; however, this difference was not statistically significant. These 5-year survival rates for low-grade serous carcinoma in the studies by Malpica et al10 and Seidman et al58 are similar to our experience.23
Few studies have compared survival using the 2-tier versus 3-tier grading systems. In the study by Malpica et al,10 serous carcinomas were graded using the 2-tier low-grade/high-grade, 3-tier universal, and 3-tier FIGO systems. All 3 grading systems showed statistically significant prediction of survival. In view of its simplicity in application and excellent reproducibility, we advocate using the 2-tier system in routine practice.
Primary Site of OriginDiagnostic problems may arise in the distinction of high-grade serous carcinoma of primary ovarian versus peritoneal or tubal origin. The GOG has proposed criteria for determining peritoneal origin for tumors synchronously involving the peritoneum and ovary. They are: both ovaries must not be enlarged because of tumor involvement; the extent of nonovarian disease must be greater than that involving the ovaries; microscopically, the ovary must show either no tumor or involvement of ovarian surface and ovarian parenchyma/stroma by tumor measuring <5 mm in greatest dimension; and the extra-ovarian tumor must display a histologic appearance consistent with that seen in ovarian serous carcinomas.63 The criteria are arbitrary and have not been scientifically validated. We do not strictly adhere to the 5 mm-criterion. Although a tumor with ovarian surface involvement and without ovarian parenchymal/stromal involvement would qualify as a peritoneal primary per the GOG criteria, we designate a tumor ≥5 mm in size involving the ovarian surface and without ovarian parenchymal/stromal involvement as an ovarian primary, unless the growth pattern on the surface of the ovary is characterized by tumor imbedded in a desmoplastic plaque typical of secondary ovarian involvement, as some primary ovarian carcinomas without significant peritoneal involvement may be predominantly located on the surface of the ovary.
The traditional criteria for determining fallopian tube origin for tumors synchronously involving the tube and ovary by Hu et al64 and subsequently modified by Sedlis65 are: (1) tumor arises from the fallopian tube mucosa, (2) histology of the tumor resembles tubal mucosa, (3) there is a transition from benign to malignant epithelium, and (4) the size of the fallopian tube tumor is larger than the ovarian tumor. Recently, the presence of TIC has been proposed as indicating fallopian tube origin for cases with a synchronous ovarian mass (see High-grade Serous Carcinoma section for Pathogenesis above for additional details).50,52,55
In cases wherein the primary site cannot be determined, this distinction usually will not be critical as most cases will typically be high stage, and the treatment and prognosis for a high-grade serous carcinoma simultaneously involving ovary and peritoneum/fallopian tube is similar regardless of which site is designated the primary site of origin.63,66–75
IMMUNOHISTOCHEMICAL FEATURES p53 (Table 3)Although TP53 is frequently mutated in ovarian high-grade serous carcinoma, numerous studies have erroneously made the assumption that p53 “immunopositivity” equates with a mutation. Rather, it is the pattern of immunohistochemical staining that correlates with mutation as opposed to simply a positive or negative stain. In the endometrium, a diffuse pattern of expression, which is typically 90% to 100% positive cells, generally correlates with a TP53 mutation. In the ovary, that correlation is not as strong.
 TABLE 3:
TABLE 3: Immunohistochemical Features of Low-grad
留言 (0)