
記住我



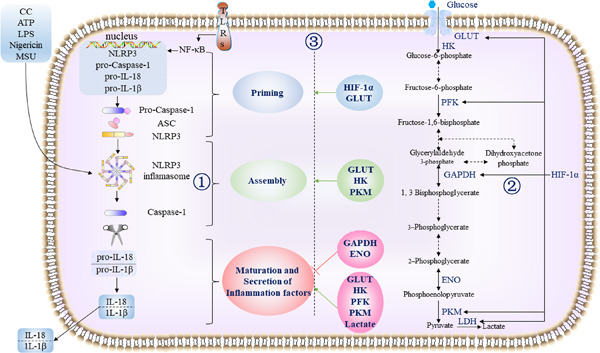
Individuals with obesity and/or type 2 diabetes are more prone to developing severe course of illness upon acquisition of coronavirus disease-2019 (COVID-19).1 Some researchers have proposed that over-activation of the nod-like receptor pyrin domain containing 3 (NLRP3) inflammasome might be the underlying culprit for the development of severe course of COVID-19 in patients with metabolic diseases.2 Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the causative pathogen of COVID-19, is capable of activating the NLRP3 inflammasome, either directly or via diverse cellular/molecular signaling events. In fact, a recent study3 comprised of 124 patients with COVID-19 (49% with obesity; 37% with type 2 diabetes) has confirmed the activation of NLRP3 inflammasome upon acquisition of infection with SARS-CoV-2 and that NLRP3 inflammasome was active in this patient population.
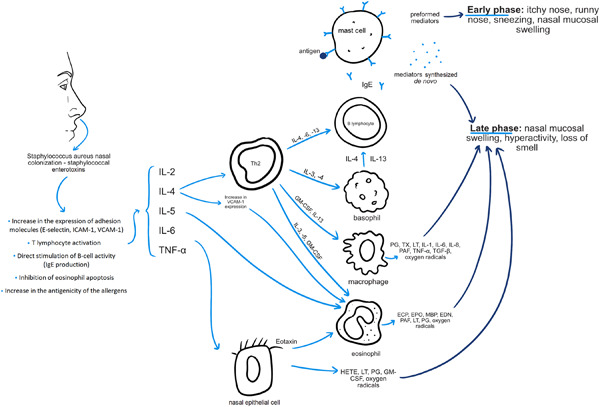
The NLRP3 inflammasome, a multiprotein complex in macrophages, dendritic cells, and other nonimmune cells, is a vital part of the innate immune system for antiviral host defenses. The aberrant activation of the NLRP3 inflammasome during the course of COVID-19 leads to the production of interleukin-1β, facilitating the development of cytokine storm and the subsequent multiorgan injury. Therefore, a well-known NLRP3 inhibitor, colchicine, appears to be promising to be repurposed for the treatment of COVID-19, especially in patients with concurrent obesity or diabetes. While the mechanisms of action of colchicine to inhibit NLRP3 inflammasome remain an area of ongoing research, colchicine has been previously shown to inhibit the activation of NLRP3 inflammasome.4 It is hypothesized that by inhibiting the activation of the NLRP3 inflammasome, colchicine reduces the release of interleukin-1β, thus preventing the subsequent induction of interleukin-6 and tumor necrosis factor for the recruitment of additional neutrophils and macrophages, which could otherwise cause cytokine storm.5
The pilot randomized controlled trial by Demidowich et al.6 has reported a reduction in the serum level of interleukin-6 among patients with obesity and metabolic syndrome upon treatment with colchicine. The beneficial effect of IL-6 inhibition in patients with COVID-19 has been established, and the ability of colchicine to interfere also with the release of cytokines other than interleukin-6 may be more advantageous, at least theoretically. There have been several clinical trials conducted to determine the effect of colchicine in patients with COVID-19. We aimed to perform a meta-analysis of randomized clinical trials investigating the effect of colchicine on the clinical outcomes in patients with COVID-19.
2 METHODSA systematic literature search with no language restriction was performed in electronic databases, including PubMed, Google Scholar, Cochrane Central Register of Controlled Trials, and preprint servers (medRxiv, Research Square, SSRN), to identify eligible studies, published up to October 17, 2021. The search strategy was built based on the following keywords and their MeSH terms: “COVID-19,” “SARS-CoV-2,” and “colchicine.” The clinical trial registries of the United States (clinicaltrials.gov), China (chictr.org.cn), and the World Health Organization international (who.int/clinical-trials-registry-platform) were also searched for registered clinical trials involving colchicine in the treatment of COVID-19, in order to identify trials with released findings. Also, the reference lists of relevant articles were reviewed to search for additional studies. Two investigators (Chia S. Kow and Syed S. Hasan) independently performed the literature screening to identify eligible studies. Studies eligible for inclusion were randomized controlled trials comparing the clinical outcomes of colchicine and its comparators in patients with COVID-19. We excluded studies with observational design, single-arm trials, nonrandomized trials, and trials that did not report outcomes of interest.
The outcomes of interest were all-cause mortality and duration of hospital stay. Two investigators (Chia S. Kow and Syed S. Hasan) independently evaluated each trial, who also extracted the study characteristics. The extracted study characteristics included the first author's surname, trial design, country where the trial was performed, age of patients, the dosing regimen of colchicine, the regimen of comparator intervention, mortality events, and duration of hospital stay.
Two investigators (Chia S. Kow and Syed S. Hasan) assessed the risk of bias of the trials included with Version 2 of the Cochrane risk-of-bias tool for randomized trials (RoB 2),7 which is a standardized method for assessing potential bias in reports of randomized interventions. RoB 2 is structured into a fixed set of bias domains, focusing on different aspects of trial design, conduct, and reporting.7
Meta-analysis with the random-effects model was used to estimate the pooled odds ratio (OR) of mortality with the use of colchicine relative to non-use of colchicine, at 95% confidence intervals (CIs). An OR of more than 1 shows increased odds of mortality while a value of less than 1 shows decreased odds of mortality, with CI inclusive of 1 indicates no significant difference in the odds of mortality. In terms of the duration of hospital stay, we estimated the pooled standardized mean difference between colchicine users and non-colchicine users using Cohen's d index. When the duration of hospital stay was not reported in mean and standard deviation, we first estimated the skewness of the data distribution using median and interquartile range with the method developed by Shi et al.8; if the distribution of data was significantly skewed from normality, the trial was excluded for analysis of the standardized mean difference in the duration of hospital stay; if the distribution of data was not significantly skewed from normality, the mean and standard deviation of the duration of hospital stay were extrapolated from the sample size, median, and interquartile range, according to the methods developed by Luo et al.9 and Wan et al.,10 respectively. We examined the heterogeneity between studies using the I2 statistics and the χ2 test, and significant heterogeneity was considered at 50% and p < .10, respectively. Publication bias was examined using the funnel plot. All analyses were performed using Meta XL, version 5.3 (EpiGear International).
3 RESULTSOur systematic literature search retrieved 689 hits, of which 450 were unique (titles retrieved after removing duplications). After screening, we selected 10 randomized controlled trials,11-20 which included 17,976 patients with COVID-19 (8427 patients were randomized to the colchicine group, and 9549 patients were randomized to the control group and did not receive colchicine). Nine of the included randomized trials were from Greece,11 Iran (n = 2),12, 16 Brazil,13 Russia,14 the United Kingdom (n = 2),17, 20 Colombia,18 and Spain,19 respectively. The remaining randomized trial15 was an international multicenter study performed in six countries. Details of the included studies are shown in Table 1. All of the included trials11-20 reported mortality outcomes, whereas six trials11-13, 15, 17, 19 reported the outcome with regard to the duration of hospital stay. A differing dosing regimen of colchicine was noted across the included randomized controlled trials (Table 1); six trials11, 13-15, 17, 19 administered loading doses of colchicine for up to 5 days before the maintenance doses, whereas three trials12, 18, 20 administered maintenance doses of colchicine without a prior loading dose. The maximum duration of use of colchicine across the included trials11-13, 15, 17-20 ranged from 6 to 28 days; the trial by Tardif et al.14 did not report the duration of therapy with colchicine while the trial by Mostafaie (NCT0439214116) did not report the dosing regimen of colchicine.
Table 1. Study characteristics of included trials Study Study design Country Age (median/mean) Proportion of patients with diabetes Body mass index (kg/m2; mean/median) Regimen of colchicine in the intervention group Regimen of comparative intervention in the controlled group Mortality Duration of hospital stay Risk of biasa Colchicine users (n/N; %) Non-colchicine users (n/N; %) Colchicine users (median/mean; days) Non-colchicine users (median/mean; days) Deftereos et al.11 Open label, randomized controlled trial GreeceColchicine users = 65
Non-colchicine users = 63
N/AColchicine users = 27.3
Non-colchicine users = 27.7
Colchicine + standard care
Loading dose: Oral colchicine 1.5 mg followed by another 0.5 mg 60 min later if no adverse gastrointestinal effects were observed (in the case of azithromycin coadministration, a single 1.0 mg loading dose of colchicine was administered)
Maintenance dose: oral colchicine 0.5 mg twice daily (reduced to once daily among patients with body weight <60 kg) until hospital discharge or a maximum of 21 days
Standard care (hydroxychloroquine/chloroquine and/or azithromycin) 1/55; 1.8 4/50; 8.0 12 (IQR: 9–22) 13 (IQR: 9–18) Some concerns Salehzadeh et al.12 Open label, randomized controlled trial IranColchicine users = 56.6
Non-colchicine users = 55.6
11% N/A Oral colchicine 1 mg daily + hydroxychloroquine + azithromycin for 6 days Placebo + hydroxychloroquine + azithromycin for 6 days 0/50; 0 0/50; 0 6.28 ± 2.51 8.12 ± 2.66 Some concerns Lopes et al.13 Randomized, double-blind, placebo-controlled trial BrazilColchicine users = 54.5
Non-colchicine users = 55.0
39%Colchicine users=33.5
Non-colchicine users=29.7
Oral colchicine 0.5 mg three times daily for 5 days, followed by 0.5 mg twice daily for 5 days (if body weight ≥80 kg, the first dose was 1.0 mg; if a patient had chronic kidney disease with glomerular filtration rate under 30 ml/min/1.73 m2, colchicine dose was reduced to 0.25 mg three times daily for 5 days, followed by 0.25 mg twice daily for 5 days) + institutional treatment Placebo + institutional treatment (azithromycin 500 mg once daily for up to 7 days + hydroxychloroquine 400 mg twice daily for 2 days, then 400 mg once daily for up to 8 day + unfractionated heparin 5000 UI three times daily + methylprednisolone 0.5 mg/kg/day for 5 days) 0/36; 0 2/36; 5.6 7.0 (IQR: 5.0–9.0) 9.0 (IQR: 7.0–12.0) Some concerns Tardif et al.14 Randomized, double-blind, placebo-controlled trial GlobalColchicine users = 54.4
Non-colchicine users = 54.9
20%Colchicine users = 30.0
Non-colchicine users = 30.0
Oral colchicine 0.5 mg twice daily for the first 3 days followed by 0.5 mg once daily for 27 days Placebo 5/2075; 0.2 9/2084; 0.4 N/A N/A Some concerns Mareev et al.15 Open label, randomized controlled trial RussiaColchicine users = 54.4
Non-colchicine users = 54.9
12%Colchicine users = 30.2
Non-colchicine users = 30.6
Oral colchicine 1 mg daily for the
first 3 days followed by 0.5 mg daily + antibiotic + anticoagulant; duration not reported
Antibiotic + anticoagulant 0/21; 0 2/22; 9.0 13.0 (IQR: 11.0–15.0) 17.5 (IQR: 12.5–19.8) High Mostafaie (NCT04392141)16 Randomized, placebo-controlled trial IranColchicine users = 53.0
Non-colchicine users = 54.1
N/A N/A Oral colchicine (dosing regimen not reported) and herbal phenolic monoterpene fractions + standard care Standard care (details were not mentioned) 1/60; 1.7 6/60; 10.0 4.17 ± 1.34 6.39 ± 2.59 Some concerns Horby et al.18 Open label, randomized controlled, platform trial United Kingdom All participants = 63.4 25% N/ALoading dose: Oral colchicine 1 mg followed by another 0.5 mg 12 h later
Maintenance dose: 0.5 mg twice daily for 10 days in total or until discharge (once daily for patients receiving a moderate CYP3A4 inhibitor or who had renal impairment) + randomization to other treatments (convalescent plasma, monoclonal antibody, aspirin, baricitinib, or tocilizumab + usual care
Usual care (corticosteroids, azithromycin, or remdesivir) 1173/5610; 20.9 1190/5730; 20.8 10.0 (range: 5.0–28.0) 10.0 (range: 5.0–28.0) Some concerns Gaitán-Duarte et al.17 Open label, randomized controlled trial ColombiaColchicine (+ rosuvastatin) users = 56.1
Colchicine (+ rosuvastatin and emtricitabine/tenofovir) users = 56.1
Non-colchicine (emtricitabine/tenofovir) users = 54.1
Non-colchicine (standard of care) users = 54.1
12% N/A Oral colchicine 0.5 mg twice daily + rosuvastatin and/or emtricitabine/tenofovir) + standard care for 14 days Standard care (dexamethasone, ivermectin, albendazole, enoxaparin, or acetaminophen) 39/312; 12.5 50/321; 15.6 N/A N/A Some concerns Pascual-Figal et al.19 Open label, randomized controlled trial SpainColchicine users = 51.8
Non-colchicine users = 50.3
15% N/AColchicine + standard care
Loading dose: Oral colchicne 1 mg followed by another 0.5 mg 2 h later
Maintenance dose: 0.5 mg every 12 h for the next 7 days and 0.5 mg every 24 h until the completion of 28 days
Standard care (dexamethasone, remdesivir, tocilizumab, baricitinib) 0/52; 0 2/51; 3.9 6.60 ± 3.86 5.76 ± 4.89 Some concerns PRINCIPLE trial20 Open label, randomized controlled trial United KingdomColchicine users = 48.5
Non-colchicine users = 61.7
11% N/A Oral colchicine 0.5 mg daily for 14 day + usual care Usual care (antipyretics) 0/156; 0 9/1145; 0.8% N/A N/A Some concerns Abbreviation: IOR, interquartile range; N/A, not applicable.The overall risk of bias assessed by RoB 2 is presented in Table 1. The trial by Mareev et al.15 had an overall high risk of bias; high risk of bias was determined for the domain of randomization because not every patient in the control group was being randomized, whereas some concerns of bias were determined for both the domain of deviations from intervention and the domain of measurement of the outcome, due to open-label design of the trial. The remaining trials had some concerns over the overall risk of bias; the trial by Deftereos et al.,11 the trial by Pascual-Figal et al.,19 and the PRINCIPLE trial20 had some concerns of bias in both the domain of deviations from intervention and the domain of measurement of the outcome, due to open-label design of the trial; the trial by Salehzadeh et al.12 had some concerns of bias in the domain of randomization since the information on allocation sequence was not reported and in both the domain of deviations from intervention and the domain of measurement of the outcome, due to open-label design of the trial; the trial by Lopes et al.13 had some concerns in the domain of selection of the reported results since the protocol and statistical analysis plan were not available; the trial by Tardif et al.14 had some concerns in the domain of randomization since the information on allocation sequence was not reported; the trial by Mostafaie (NCT04392141)16 had some concerns in the domain of randomization since the information on allocation sequence was not reported; the trial by Gaitán-Duarte et al.17 had some concerns in the domain of measurement of the outcome since the outcome assessors were not blinded; the trial by the trial by Horby et al.18 had some concerns of bias in the domain of deviations from intervention due to open-label design of the trial. All the trials above11-15 had a low risk of bias for other domains assessed.
The meta-analysis revealed no significant difference in the odds of mortality with the use of colchicine among patients with COVID-19 relative to non-use of colchicine; the estimated effect though indicated mortality benefits (Figure 1; pooled OR = 0.76; 95% CI 0.53–1.07, n = 17,976), but is without adequate evidence against the hypothesis of “no significant difference” at the current sample size. Nevertheless, the meta-analysis revealed a statistically significant reduction in the duration of hospital stay with the use of colchicine among hospitalized patients with COVID-19 relative to non-use of colchicine; the estimated effect indicated reduction of hospital stay by about 0.6 days (Figure 2; pooled standardized mean difference = −0.59; 95% CI −1.09 to −0.13, n = 438), with some evidence against the hypothesis of “no significant difference” at the current sample size. A funnel plot (or scatter plot) of the effect estimates from individual studies revealed no or limited bias as all studies are within a triangle centered on a fixed effect summary estimate and extending 1.96 standard errors on either side (Figure S1).

Pooled odds ratio of mortality between colchicine users and non-colchicine users with coronavirus disease-2019. CI, confidence interval; OR, odds ratio

Pooled standardized mean difference of duration of hospital stay between colchicine users and non-colchicine users with coronavirus disease-2019. CI, confidence interval
4 DISCUSSIONThe ability of colchicine to reduce the length of stay in hospitalized patients with COVID-19 is consistent with its potential to prevent cytokine storm via inhibition of NLRP3 inflammasome, which could prevent clinical deterioration of colchicine users with COVID-19. Indeed, a significant reduction in the inflammatory marker, C-reactive protein, was noticed in the trial by Mareev et al.15 among colchicine users (from a median of 99.4 mg/dl to a median of 4.2 mg/dl; p < .001), while no significant reduction was observed among non-colchicine users. Furthermore, the trial by Deftereos et al.11 also reported lower maximal C-reactive protein levels among colchicine users than non-colchicine users (3.1 vs. 4.5 mg/dl). However, the difference is not statistically significant.
Nevertheless, such beneficial effects of colchicine did not translate into mortality benefits. It is likely that the proportion of enrolled patients with concurrent obesity and/or diabetes (ranged from 11% to 39%) who can have more pronounced activation of the NLRP3 inflammasome was too low to allow detection of mortality benefits (Table 1).21, 22 In the trial by Tardif et al.,14 where the participants had a median body mass index of 30.0 kg/m2, there was a significant reduction in the odds for a composite of death or hospitalization due to COVID-19 in colchicine users compared to non-colchicine users (OR = 0.75; 95% CI: 0.57–0.99). Noteworthily, the aforementioned trial14 investigated the use of colchicine among nonhospitalized patients with COVID-19. Besides, the prespecified subgroup analysis reported that the odds for a composite of death or hospitalization due to COVID-19 was trended towards a significant effect in patients with concurrent diabetes receiving colchicine (OR = 0.37; 95% CI: 0.37–1.01).14 Therefore, with the wisdom of hindsight, future randomized trials with colchicine should focus on the population of patients with COVID-19 with concurrent obesity and/or diabetes, at the early (mild) stage of illness, to prevent clinical deterioration.
This study has its limitations. First, a variety of dosing regimens of colchicine was being investigated across the trials; therefore, it is not known with certainty the most appropriate regimen in patients with COVID-19. Second, none of the included randomized trials are of high-quality without apparent risks of bias. Third, the trials included for the estimation of pooled standardized mean difference of the duration of hospital stay were of relatively small sample size; however, there was no heterogeneity (0%) across the trials.
CONFLICT OF INTERESTSThe authors declare that there are no conflict of interests.
AUTHOR CONTRIBUTIONSConceptualization: Chia S. Kow and Syed S. Hasan. Formal analysis: Chia S. Kow, Learn-Han Lee, Syed S. Hasan, and Long C. Ming. Methodology: Chia S. Kow, Dinesh S. Ramachandram, Syed S. Hasan, and Hui P. Goh. Writing – original draft: Chia S. Kow, Learn-Han Lee, Dinesh S. Ramachandram, Syed S. Hasan, and Long C. Ming. Writing – review and editing: Chia S. Kow, Syed S. Hasan, Long C. Ming, and Hui P. Goh.
All data generated or analyzed during this study are included in this published article.
Filename Description iid3562-sup-0001-Supplementary_File_S1.docx22.5 KB Supporting information.Please note: The publisher is not responsible for the content or functionality of any supporting information supplied by the authors. Any queries (other than missing content) should be directed to the corresponding author for the article.
REFERENCES
1Corona G, Pizzocaro A, Vena W, et al. Diabetes is most important cause for mortality in COVID-19 hospitalized patients: systematic review and meta-analysis. Rev Endocr Metab Disord. 2021; 22: 1- 22. 2Bertocchi I, Foglietta F, Collotta D, et al. The hidden role of NLRP3 inflammasome in obesity-related COVID-19 exacerbations: lessons for drug repurposing. Br J Pharmacol. 2020; 177(21): 4921- 4930. 3Rodrigues TS, de Sá KSG, Ishimoto AY, et al. Inflammasomes are activated in response to SARS-CoV-2 infection and are associated with COVID-19 severity in patients. J Exp Med. 2021; 218(3):e20201707. 4Martinon F, Pétrilli V, Mayor A, Tardivel A, Tschopp J. Gout-associated uric acid crystals activate the NALP3 inflammasome. Nature. 2006; 440(7081): 237- 241. 5Fordham JN, Kirwan J, Cason J, Currey HL. Prolonged reduction in polymorphonuclear adhesion following oral colchicine. Ann Rheum Dis. 1981; 40(6): 605- 608. 6Demidowich AP, Levine JA, Apps R, et al. Colchicine's effects on metabolic and inflammatory molecules in adults with obesity and metabolic syndrome: results from a pilot randomized controlled trial. Int J Obes. 2020; 44(8): 1793- 1799. 7Sterne JAC, Savović J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019; 366:l4898. 8Shi J, Luo D, Wan X. Detecting the skewness of data from the sample size and the five-number summary. arXiv. 2020. 9Luo D, Wan X, Liu J, Tong T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat Methods Med Res. 2018; 27(6): 1785- 1805. 10Wan X, Wang W, Liu J, Tong T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol. 2014; 14: 135. 11Deftereos SG, Giannopoulos G, Vrachatis DA, et al. Effect of colchicine vs standard care on cardiac and inflammatory biomarkers and clinical outcomes in patients hospitalized with coronavirus disease 2019: the GRECCO-19 randomized clinical trial. JAMA Netw Open. 2020; 3(6):e2013136. 12Salehzadeh F, Pourfarzi F, Ataei S. The impact of colchicine on the COVID-19 patients: a clinical trial study. Research Square. 2020. 13Lopes MI, Bonjorno LP, Giannini MC, et al. Beneficial effects of colchicine for moderate to severe COVID-19: a randomised, double-blinded, placebo-controlled clinical trial. RMD Open. 2021; 7(1):e001455. 14Tardif J-C, Bouabdallaoui N, L'Allier PL, et al. Colchicine for community-treated patients with COVID-19 (COLCORONA): a phase 3, randomised, double-blinded, adaptive, placebo-controlled, multicentre trial. The Lancet Respiratory Medicine. 2021; 9:(8): 924– 932. doi:10.1016/s2213-2600(21)00222-8 15Mareev VY, Orlova YA, Plisyk AG, et al. Proactive anti-inflammatory therapy with colchicine in the treatment of advanced stages of new coronavirus infection. The first results of the COLORIT study. Kardiologiia. 2021; 61(2): 15- 27. 16Colchicine plus phenolic monoterpenes to treat COVID-19. ClinicalTrials.gov identifier: NCT04392141. April 20, 2021. Accessed July 11, 2021. https://www.clinicaltrials.gov/ct2/show/NCT04392141 17Gaitán-Duarte HG, Rincon-Rodriguez CJ, Yomayusa-Gonzalez N. Effectiveness of rosuvastatin plus colchicine, emtricitabine/tenofovir and a combination of them in hospitalized patients with SARS Covid-19. medRxiv. 2021. 18Colchicine in patients admitted to hospital with COVID-19 (RECOVERY): a randomised, controlled, open-label, platform trial. The Lancet Respiratory Medicine. 2021; doi:10.1016/s2213-2600(21)00435-5 19Pascual-Figal DA, Roura-Piloto AE, Moral-Escudero E, et al. Colchicine in recently hospitalized patients with COVID-19: a randomized controlled trial (COL-COVID). Int J Gen Med. 2021; 14: 5517- 5526. 20Dorward J, Yu LM, Hayward G. Colchicine for COVID-19 in adults in the community (PRINCIPLE): a randomised, controlled, adaptive platform trial. medRxiv. 2021. 21
留言 (0)