
記住我



The first part of the current study was conducted on 173 COVID-19 hospitalized (severe) patients, of which 91 (52.6%) were male and 82 (47.4%) were female. This gender infection rate with SARS-CoV-2 is similar to that of other studies.19-21 The first study group was divided into two categories: survivors (143; 79 males, 64 females) and deceased (30; 12 males, 18 females; Figure 2).

First studied COVID-19 patients, including hospitalized 173 patients (male, 91 and female, 82). Studied COVID-19 patients divided into two categories; survivors patients, 143 (male, 79 and female, 64) and dead patient, 30 (male, 12 and female, 18)
The rate of death among females (18/82; 21.9%) in the current study was generally higher than that of males (12/91; 13.1%). This result conflicts with data from a study conducted with more than 1500 COVID-19 patients from different areas of the world, which concluded that male patients have a higher mortality rate than females.19 This discrepancy may be due to age, as the females in the current study were older (60.16 ± 12.11 years) than the males (59.35 ± 10.25 years), and older patients are more vulnerable to severe disease and death from SARS-CoV-2 infection.22, 23
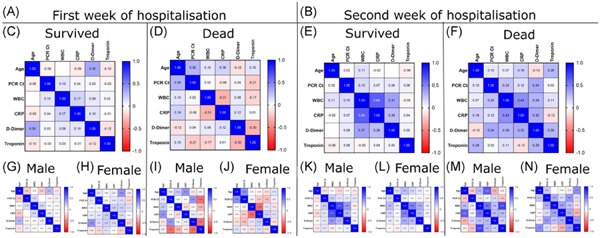
In the first week of admission to the hospital, there was no correlation among any studied parameters (Figure 3A). This was likely because the immune system requires sufficient time to react specifically to a disease, so when the body encounters the SARS-CoV-2 virus for the first time, the immune system cannot work properly and illness may then occur.24

Correlation between studied parameters; Age, PCR-Ct, WBC, CRP, D-dimer and troponin at the COVID-19 patients first week of admission (A) in male (C) and female (D). Also at the second week of admission (B) in male (E) and female (F). CRP, C-reactive protein; PCR-Ct, polymerase chain reaction–cycle threshold; WBC, white blood cell
In the second week of hospitalization, we found a positive correlation (r = 0.73, p < 0.0001) between WBCs and CRP (Figure 3B). When patients were divided by gender, the positive correlation remained (male, r = 0.75, p < 0.0001; female, r = 0.72, p < 0.0001; Figure 3F,G). In addition, a positive correlation (r = 0.69, p < 0.0001) was observed between WBCs and D-dimer in female patients (Figure 3G), but the correlation was much weaker in males (r = 0.49, p < 0.0001; Figure 3F).
When the immune system reacted with the SARS-CoV-2 virus during the second week of hospitalization, the WBC and CRP levels were elevated in a positively correlated manner. Elevation of blood leukocytes and CRP may be used as an indicator of the severity of COVID-19.25 During the course of COVID-19, elevation of leukocyte count and CRP is common among hospitalized COVID-19 patients. Although elevated D-dimer levels are consistently observed, their gradual increase during the course of the disease is particularly associated with disease worsening.26 The difference in correlation strength between D-dimer and WBCs regarding male and female patients may be a second factor, in addition to age, to explain the previously mentioned high rate of death among females (see Figure 2).
When the results were analyzed by category (survivors and deceased), neither survivors nor deceased patients showed any correlation among the studied parameters during their first week of hospital admission (Figure 4A). In the second week of the hospitalization, however, we found a positive correlation (r = 0.71, p < 0.0001) between WBCs and CRP in male survivors (Figure 3K). CRP is a universal inflammatory factor that has been evaluated under many conditions27 and recently, it has been found that WBC count, coupled with CRP, is involved in the prognosis of COVID-19.28, 29

Correlation between studied parameters; Age, PCR-Ct, WBC, CRP, D-dimer and troponin at the first week of COVID-19 patient admission (A) in survived (C); male (G), female (H) and dead COVID-19 patients (D); male (I), female (J). Also at the second week of the patient admission (B) in survived (E); male (K), female (L) and dead COVID-19 patients (F); male (M), female (N). CRP, C-reactive protein; PCR-Ct, polymerase chain reaction–cycle threshold; WBC, white blood cell
A strong positive correlation (r = 0.73, p = 0.007) was observed between WBCs and troponin in deceased male patients (Figure 4M), indicating a vital role for troponin in predicting death from COVID-19. Troponin levels are a well-established marker of myocardial injury,30 and early studies in patients with COVID-19 reported that elevated plasma troponin levels were common and associated with a more severe clinical course and increased in-hospital death.31-34
There was a highly significant difference in age (p < 0.0001, 10.76 ± 2.102 years) between survivors (57.8 years) and those who died (68.6 years; Figure 5), supporting the likelihood that age may play a role in the rate of death. Reports from different countries refer to a greater risk of death and high mortality rate among older patients with COVID-19, in comparison with younger patients.35-37

Differences in parameters between survivors and the dead COVID-19 patients at first and second week of the COVID-19 disease. CRP, C-reactive protein; PCR-Ct, polymerase chain reaction–cycle threshold; WBC, white blood cell. NS, 0.1234; **0.0021; ****<0.0001.
In the first week of patient admission, there was a highly significant difference (p < 0.0001) between both groups in D-dimer (226.2 ± 41.53 ng/ml) and CRP (5.000 ± 0.9403 mg/L) levels. D-dimer elevation has been linked to coagulopathy and, with disseminated intravascular coagulation,12, 38 can lead to COVID-19-associated coagulopathy,39, 40 subsequently developing into capillary microthrombosis, as observed in post-mortem studies.41 In addition, CRP can be considered an early indicator of pneumonia and the severity of COVID-19.42, 43
In the first week of admission, there were also significant differences between both groups regarding troponin (p = 0.0038; 0.05817 ± 0.01984), WBCs (p = 0.0074; −0.4137 ± 0.1526), and PCR-Ct (p = 0.001; −2.502 ± 0.7484; Figure 5). Levels of D-dimer, CRP, troponin, and viral load were higher in patients who died than in survivors, whereas WBC count was higher among survivors. Troponin increases indicate myocardial injury and have been correlated positively with mortality,44 and some studies have considered it a predictor of death in COVID-19 patients.45 Although a number of studies have shown that immune cells may play a serious role in COVID-19 severity and susceptibility,46-48 the relation between WBC levels and severity of COVID-19 remains unclear. Interestingly, for unknown reasons, the viral load of deceased patients in their first week of admission was significantly lower than that of survivors.49
In the second week of hospitalization, all studied parameters differed highly significantly (p < 0.0001) between survivors and deceased COVID-19 patients, with the exception of PCR-Ct. Mean differences between survivors and those who died were 0.7782 ± 0.08275 for troponin, 1685 ± 176.4 for D-dimer, 25.10 ± 2.500 for CRP, and 10.32 ± 0.8450 for WBC count. When the levels of troponin, D-dimer, CRP, and WBCs had returned to normal in the survivors, all remained elevated in the patients who died. If we take into account that the PCR-Ct value was negative for both categories, it may be concluded that secondary infection50 and multiorgan dysfunction51 caused by the SARS-CoV-2 virus were possible causes of death. Elevation of cardiac injury and coagulation pathways may be relevant in defining the risk of mortality related to elevated troponin levels in patients with SARS-CoV-2.52
The current study showed that there were no significant differences in any parameters between male and female patients in both weeks of admission (Figure S1).
3.2 Second studyIn the second part of this study, COVID-19 patients were re-categorized into two groups. The first group comprised seven families (41 patients; 23 males, 18 females) that lost more than one member due to COVID-19, with a total of 15 deaths recorded (seven males, eight females). The second group, which was the control (132 patients; 69 males, 63 females), also recorded 15 deaths (five males, 10 females; Figure 6).

COVID-19 patients were re-categorized into two category: first, families who lost >1 member due to COVID-19 (41 patients; male, 23 and female, 18). Death number in this group was 15 (male, 7 and female, 8). Second, the control (132 patients; male, 69 and female, 63), this group lost 5 male and 10 females)
There was a significant difference in age between families in which more than one death occurred and the COVID-19 patient control group (p = 0.003, −5.911 ± 1.946; Figure 7). Detailed data related to parameters correlated with families who recorded more than one death or the control group during the first and second week of patient hospitalization, taking into account gender differences, are presented in Figure S3.

The differences between families with >1 death and control group in some parameter value in the first and the second week of COVID-19 disease first and second week of the COVID-19 disease. CRP, C-reactive protein; PCR-Ct, polymerase chain reaction–cycle threshold; WBC, white blood cell. NS, 0.1234; *0.0332; **0.0021; ***0.0002; ****<0.0001.
In the first week of patient admission, both groups differed significantly in PCR-Ct (p < 0.0001, 3.542 ± 0.6321), WBC count (p = 0.001, 0.4515 ± 0.1344), CRP (p = 0.006, −2.484 ± 0.8835), and D-dimer (p = 0.044, −80.29 ± 39.58), but there were no significant differences in troponin levels (Figure 7).
In the second week of hospitalization, patients in families with more than one death differed highly significantly from the control group in relation to troponin (p = 0.0006, −0.3055 ± 0.08769), WBC count (p = 0.0005, −3.517 ± 0.9938), and CRP (p = 0.024, −6.273 ± 2.765). Conversely, there were no significant differences between the groups in D-dimer and PCR-Ct (Figure 7).
Levels of WBC, CRP, D-dimer, and troponin (not clearly significant) during the first week of hospital admission differed between families that lost more than one member and the control group (Figure 7). These differences remained and appeared more clearly in the second week, especially the differences in troponin and D-dimer. Family variation could explain why some families lost more members than others. The difference in death rate among families could be due specifically to some genetic variations among these families. For example, the predicted binding peptides for SARS-CoV-2 were found in patients with the HLA gene allele HLA-B*46:01,53 suggesting that individuals in families harboring this allele may be particularly vulnerable to COVID-19.54 Additionally, the HLA-C*05 allele was correlated with COVID-19 mortality in an ecological study.55
The host's genetic background influencing the susceptibility and outcome of multiple infectious diseases has been previously reported56, 57 and a global project has been started to understand the pathogenesis of COVID-19, especially severe cases in young people.57 In addition, the “COVID-19 Host Genetics Initiative” has been launched to bring the human genetics community together to identify the genetic determinants of COVID-19 susceptibility, severity, and outcomes.58 Here, family genetic sequencing studies are needed to investigate increased troponin and WBC levels in families who are highly susceptible to death.
To conclude, the current study observed that levels of troponin, D-dimer, CRP, and WBCs were significantly higher in COVID-19 patients who died than in COVID-19 survivors. High troponin and WBC levels, especially within the second week of admission, were considerably associated with families that lost more than one member, when compared with the unrelated COVID-19 patient control.
留言 (0)