
記住我

On 11 March 2020 when the World Health Organization (WHO) declared the “coronavirus disease-2019” (COVID-19) a pandemic, the first case was announced by the Ministry of Health in Turkey. COVID-19 pandemic itself and the social restriction measures applied to control the transmission of the virus have influenced many areas of medical interventions including ongoing treatments of chronic diseases all over the world. Meanwhile, statements from specific health organizations have been announced to warn patients and healthcare professionals about the importance of maintaining such treatments under many different clinical conditions. Similarly, a recent Allergic Rhinitis and its Impact on Asthma (ARIA)-European Academy for Allergy and Clinical Immunology (EAACI) statement has addressed issues and recommendations on how to handle allergen immunotherapy (AIT) during the pandemic.1
AIT, the only disease-modifying therapy that confers a long-term clinical benefit for inhalant and venom allergies, has been used as a treatment modality for more than 100 years.2-5 Subcutaneous immunotherapy (SCIT), the oldest route of administration has disadvantages like necessity of regular follow-ups and applications in the clinic when compared to other routes.2, 3, 6 Therefore, it is inevitable that there could be disruptions in SCIT administrations during the COVID-19 pandemic that has deeply affected the healthcare system.
The ARIA-EAACI statement document recommended prolonging injection intervals during SCIT in patients acutely infected by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) like in other respiratory infections. However, by taking necessary precautions, the continuation of SCIT was recommended in asymptomatic patients without suspicious infection and/or possible contact with SARS-CoV-2-positive individuals, in patients with negative test results, in those following an adequate quarantine period and finally in those with high serum IgG levels to SARS-CoV2 with nondetectable virus-specific IgM levels.1 This statement is expected to have an important influence in guiding daily clinical practice of SCIT in many countries since treatment disruptions caused by a pandemic are a new field for the physicians, and it is important to prevent any negative effects on treatment success. Real-life data on SCIT practices during the pandemic are important to show the implementation and further improvement of such recommendations. In this real-life multicenter study, our aim was to investigate adherence to SCIT and influence of treatment disruptions on short-term clinical outcomes in patients on maintenance phase of SCIT with aeroallergens during the COVID-19 pandemic.
2 METHODS 2.1 Study designThis multicenter study was prospectively conducted on adult allergic rhinitis (AR) and/or asthmatic patients receiving the maintenance phase of SCIT with aeroallergens in the coordinating center of the study, the adult immunology and allergy clinic at Istanbul Faculty of Medicine and in three other adult immunology and allergy centers in Istanbul (Yedikule Chest Diseases and Thoracic Surgery Education and Research Hospital, Şişli Hamidiye Etfal Education and Research Hospital, Kartal Dr Lütfi Kırdar Education and Research Hospital).
During the study period of 15 March 2020 and 15 September 2020, patients' routine SCIT injection visits were continued under strict virus transmission prevention measures. All staff members used personal protective equipments during SCIT application visits to ensure standard contact and droplet protection.1 Wearing a surgical mask was mandatory for all patients. Sufficient time was left between each application and interviews to provide ambient ventilation, necessary preparations, and disinfection of materials that might have been contaminated. As recommended, injection visits were not interrupted unless the patient and/or his/her contact persons were infected.1 All allergy clinics participating in the study kept providing their outpatient services in order not to affect patients' adherence during the pandemic period. Coordination between the centers was continued with regular calls during the study period to notice any failures in routine practices.
Treatment interruptions and their reasons were collected through telephone interviews at the end of August 2020. In addition, the patients' educational status, professions, transportation options for reaching the hospital, smoking habits, co-morbid diseases, concomitant drug usage, and concomitant COVID-19 infection were all questioned (For detailed information, please refer to Appendix S1).
The patients were allocated into three groups according to SCIT application periods. The first group consisted of the patients who received SCIT injections in the recommended routine time interval of 1 month. The patients who missed injection doses that resulted in an interval of <2 months and ≥2 months between subsequent injections formed the second and third groups, respectively.2 Patients in Group 3 were considered as nonadherent whereas patients in Group 1 and Group 2 as adherent according to SCIT adherence studies.2 The reasons for missing doses were questioned and identified. Patients' demographic features and clinical diagnostic tests were collected from medical chart records. The measures of asthma control test (ACT),7 symptom, medication, and quality of life (QoL) scores were applied routinely on injection visits every 6 months before the pandemic and once during the pandemic and were compared among adherent and nonadherent groups.
Before the study, ethical approval from the ethics committee of Istanbul Faculty of Medicine (2020/78367) and authorization from The Ministry of Health for conducting the study (2020-06-04T13_52_49) were obtained. After the clinical data of each patient were filled in medical charts and were ready to be used as study documents, patients' informed consent forms were collected after the telephone interviews in order not to influence the real-life findings of the study.
2.2 Patients' recruitmentThe patients older than 18 years of age with AR and/or allergic asthma who were receiving the maintenance phase of SCIT with pollen, house dust mite (HDM), cat, or mold allergens during the study period and those who had attended their regular SCIT application visits in the pre-pandemic period according to the medical records were included in the study.
2.3 The evaluation of symptom, medication, and quality of life scoresSymptom scores with both the total symptom score-6 (TSS-6) and the visual analogue scale (VAS),8, 9 and QoL with VAS2, 9 are applied to all patients before the initiation of immunotherapy and in every 6 months until the end of the therapy as part of a routine clinical practice at the study centers. The TSS-6 was assessed by the sum of six symptoms related to nasal, ocular, ear, and/or palate with ratings for each symptom ranging from 0 to 3 with a total possible score from 0 (absence of symptoms) to 18 (very severe).2, 9 VAS-symptom scores ranged from “nasal symptoms, not at all bothersome” (0 cm) to “nasal symptoms, extremely bothersome” (10 cm).9 The QoL scores were measured with VAS which ranged from “intolerable bothersome” (0 cm) to “not at all bothersome” (10 cm). The patients were instructed to use rescue medication as a stepwise regiment by stepping it up when symptoms were not sufficiently alleviated. The medication score (MS) from the study by Gelincik et al. was used and defined according to the steps, with a range from 0 to 6 shown in Table S1.2 MSs in the pre-pandemic period were determined from the data in the medical charts, whereas MSs during the pandemic were assessed at the last injection visit.
2.4 Statistical AnalysisAll analyses were performed with the IBM Statistical Package for the Social Science version 21.0 (SPSS Inc., Chicago, IL, USA) for Windows. Descriptive data were given as percentages and as mean ± SD or median (IQR 25-75). The comparisons of ACT, VAS-symptom, TSS-6, VAS-QoL, and MS between the pre-pandemic and during the pandemic periods were performed with the Wilcoxon signed-rank test while the comparisons of ACT, VAS-symptom, TSS-6, VAS-QoL, and MS between the groups were performed with the Kruskal-Wallis H test. The scores of ACT, VAS-symptom, VAS-QoL, MS, and TSS-6 during the pandemic were compared between the groups in pairs with the Mann-Whitney U test. Categorical variables were evaluated using the chi-square test among groups, and significant variables were further evaluated using the logistic regression analysis. Spearman correlation test was used to show the correlation between the delay in the application time of the patients and the differences in VAS-symptom, VAS-QoL, TSS-6, and MSs due to the pandemic. The power of correlation was defined as very weak if r < .2, weak if r = .2–0.4, moderate if r = .4–0.6, strong if r = .6–0.8, very strong if r > .8. The results were assessed at a significant level of p < 0.05 and a 95% confidence interval (CI).
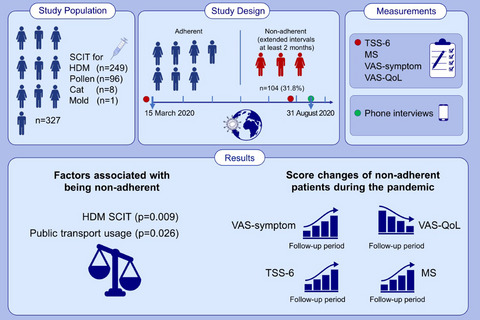
3 RESULTS 3.1 Demographic and clinical features of the study participantsA total of 327 adult patients were included in the study. The mean age was 35.0 ± 11.1 years, and a majority of them (62.4%) was female. 73.4% (n = 240), 26.3% (n = 86), and 0.3% (n = 1) of the patients had AR, concomitant AR and allergic asthma, and allergic asthma, respectively. A total of 249 (76.1%) patients were sensitive to HDM, 96 (29.3%) were sensitive to pollen, 8 (2.4%) were sensitive to cat, and 1 (0.3%) was sensitive to mold. The median duration of SCIT was 23 months (IQR 25–75: 10–36 months). During the COVID-19 pandemic, immunotherapy was administered to 151 (46.1%) patients (Group 1) at recommended intervals, 72 (22.0%) patients at extended intervals of less than 2 months (Group 2), and 104 (31.8%) patients at extended intervals of at least 2 months (Group 3). The demographic and clinical features of the patients are shown in detail in Table 1.
TABLE 1. Clinical and demographic data of the patients Patients p * Group 1 (n = 151) Group 2 (n = 72) Group 1+2 (Adherent) (n = 223) Group 3 (Nonadherent) (n = 104) Age, mean 36.5 ± 11.3 32.9 ± 10.7 35.4 ± 11.2 34.3 ± 10.8 NS Sex, n (%) Women 90 (59.6) 45 (62.5) 135 (60.5) 69 (66.3) NS Men 61 (40.4) 27 (37.5) 88 (39.5) 35 (33.7) Diagnosis of respiratory diseases, n (%) Allergic rhinitis 111 (73.5) 56 (77.8) 167 (74.9) 73 (70.2) NS Allergic asthma 0 (0) 0 (0) 0 (0) 1 (1.0) NS Allergic rhinitis and asthma 40 (26.5) 16 (22.2) 56 (25.1) 30 (28.8) NS Type of allergen, n (%) HDM 87 (57.6) 55 (76.4) 142 (63.7) 82 (78.8) .003 Weed pollens 24 (15.9) 6 (8.3) 30 (13.5) 8 (7.7) NS Grass pollens 9 (6.0) 2 (2.8) 11 (4.9) 2 (1.9) NS Grass and cereal pollens 10 (6.6) 6 (8.3) 16 (7.2) 3 (2.9) NS Grass and weed pollens 2 (1.3) 0 (0) 2 (0.9) 0 (0) NS Grass, cereal, and weed pollens 1 (0.7) 0 (0) 1 (0.4) 0 (0) NS Cat 1 (0.7) 0 (0) 1 (0.4) 1 (1.0) NS Alternia alternata 1 (0.7) 0 (0) 1 (0.4) 0 (0) NS HDM and weed pollens 6 (4.0) 0 (0) 6 (2.7) 1 (1.0) NS HDM and grass pollens 1 (0.7) 2 (2.8) 3 (1.3) 3 (2.9) NS HDM, grass, and cereal pollens 5 (3.3) 1 (1.4) 6 (2.7) 2 (1.9) NS Cat and grass pollens 2 (1.3) 0 (0) 2 (0.9) 0 (0) NS HDM and cat 2 (1.3) 0 (0) 2 (0.9) 2 (1.9) NS Any pollen with or without another concomitant allergen 60 (39.7) 17 (23.6) 77 (34.5) 19 (18.3) .003 Duration of immunotherapy (month) Median (IQR 25–75) 24 (9.5–37) 20 (10–36) 21 (10–36) 24 (12–34) NS Cigarette, n (%) User 30 (19.9) 14 (19.4) 44 (19.7) 25 (24.0) NS Nonuser 121 (80.1) 58 (80.6) 179 (80.3) 79 (76.0) Level of education, n (%) Not educated 1 (0.6) 0 (0) 1 (0.4) 2 (1.9) NS Primary school 24 (15.8) 6 (8.3) 30 (13.4) 19 (18.2) NS Intermediate school 15 (9.9) 9 (12.5) 24 (10.7) 4 (3.8) NS High school 42 (27.8) 17 (23.6) 59 (26.4) 23 (22.1) NS University 69 (45.6) 40 (55.5) 109 (48.8) 56 (53.8) NS Occupation, n (%) Blue collar workers 39 (25.8) 11 (15.3) 50 (22.4) 16 (15.4) NS White collar workers 23 (15.2) 12 (16.7) 35 (15.6) 17 (16.3) NS Government employee 20 (13.2) 7 (9.7) 27 (12.1) 13 (12.5) NS Healthcare workers 5 (3.3) 4 (5.6) 9 (4.0) 6 (5.8) NS Tradesmen 3 (2.0) 3 (4.2) 6 (2.6) 3 (2.9) NS Students 15 (9.9) 13 (18.1) 28 (12.5) 14 (13.5) NS Retired 4 (2.6) 1 (1.4) 5 (2.2) 1 (1.0) NS Housewives 38 (25.2) 18 (25.0) 56 (25.1) 29 (27.9) NS Unemployed 4 (2.6) 3 (4.2) 7 (3.1) 5 (4.8) NS Transportation options for reaching the hospital, n (%) Public transport 63 (41.7) 40 (55.6) 103 (46.2) 64 (61.5) . 010 Private vehicle or on foot 88 (58.3) 32 (44.4) 120 (53.8) 40 (38.5) Note Group 1 = routine intervals; Group 2 = extended intervals (<2 months); Group 3 = extended intervals(≥2 months); NS = nonsignificant; HDM = house dust mite. Statistical significance level was set at < .05 and value of statistical significance was marked in bold. 3.2 Adherence rates and reasons for extending SCIT administration intervalsA total of 104 (31.8%) patients (Group 3) were considered as nonadherent, whereas 72 (22.0%) patients (Group 2) who extended injection intervals for less than 2 months and 151 (46.1%) patients (Group 1) who received injections on routine injection visits were adherent.
The reasons for extending the SCIT administration intervals during the pandemic in Group 2 (n = 72) in decreasing significance order were as follows; staying at home due to precautionary reasons for 33 patients (45.8%), unwilling to go to the hospital for 18 patients (25.0%), transportation problems for 6 patients (8.3%), delay in the import of the vaccine for 4 patients (5.6%), having acute COVID-19 for 4 patients (5.6%), the thought that allergy clinics were closed during the pandemic for 4 patients (5.6%), and personal reasons unrelated to the pandemic for 3 patients (4.2%).
In Group 3, the reasons of nonadherence were as follows; staying at home due to precautionary reasons for 48 patients (46.2%), unwilling to go to the hospital for 12 patients (11.5%), transportation problems for 17 patients (16.4%), delay in the import of the vaccine for 16 patients (15.4%), having acute COVID-19 for 5 patients (4.8%), having a health problem other than COVID-19 for 2 patients (1.9%), the thought that allergy clinics were closed during the pandemic for 2 patients (1.9%), and personal reasons unrelated to the pandemic for 2 patients (1.9%), respectively.
Univariate analysis revealed that AIT with HDM and public transport usage were higher in the nonadherent group than the adherent group (p = 0.003, p = 0.010, respectively), whereas the patients receiving pollen SCIT with or without another concomitant allergen (n = 96) were more adherent (p = 0.003) (Table 1). In the logistic regression analysis, AIT with HDM and public transport usage were significantly higher among nonadherent patients (patients in Group 3) than adherent patients (patients in Group 1 and Group 2) (p = 0.009, p = 0.026, respectively) (Table 2).
TABLE 2. Logistic regression analysis of the factors associated with being nonadherent Variable p value Odds ratio 95% confidence interval Type of allergen: HDM .009 2.107 1.207 3.678 Public transport usage .026 1.731 1.069 2.803When categorizing the patients according to their duration of maintenance phases as those in the 1st, 2nd, or the 3rd year, we could not show any significance among adherent and nonadherent groups.
3.3 Comparison of AIT effectiveness and quality of life between groupsBefore the pandemic, the median TSS-6, VAS-symptom, MS, and VAS-QoL scores were similar in all groups (p > 0.05 for each comparison). During the pandemic, the median TSS-6 and VAS-symptom scores were the highest in Group 3 compared with other groups (p < 0.001 for each comparison) and these values were similar between Group 1 and Group 2 (p > 0.05, p > 0.05, respectively). The median MSs were similar in all groups during the pandemic (p > 0.05). Median VAS-QoL scores were the lowest in Group 3 compared with others (p < 0.001 for each comparison) and were lower in Group 2 than Group 1 (p = 0.043) (Figure 1).

Changes in TSS-6 (A), VAS-symptom (B), VAS-QoL (C), and MS (D) according to the immunotherapy application interval during COVİD-19 pandemic. NS = nonsignificant; A = TSS-6; B = VAS-symptom; C = VAS-QoL; D = MS; Red = Group 1 (Routine intervals); Purple = Group 2 (extended intervals - <2 months); Green = Group 3 (extended intervals - ≥2 months)
When comparing adherent and nonadherent patients, the median TSS-6, VAS-symptom, MS, and VAS-QoL scores were similar before the pandemic (p > 0.05 for each comparison). During the pandemic, the median TSS-6 and VAS-symptom scores were higher and the median VAS-QoL score was lower in the nonadherent patients than the adherent patients (p < 0.001 for each comparison). However, the median MS was similar in both groups during the pandemic (p > 0.05) (Figure 2).

Changes in TSS-6 (A), VAS-symptom (B), VAS-QoL (C), and MS (D) according to the immunotherapy application interval during COVİD-19 pandemic for adherent (Group 1 + Group 2) and nonadherent patients (Group 3). NS = nonsignificant; A = TSS-6; B = VAS-symptom; C = VAS-QoL; D = MS; Blue = adherent; Green: nonadherent
Since the study period corresponds to the pollination period of common pollen allergens in our geographic region, the patients who received and those who did not receive pollen immunotherapy were compared in terms of short-term clinical outcomes of AIT. Changes in MS, VAS-symptom, VAS-QoL, and TSS-6 scores between the pandemic and the pre-pandemic periods were similar among these patients (p > 0.05 for each comparison).
3.4 Comparison of AIT effectiveness and quality of life within groupsMedian TSS-6, VAS-symptom, MS, and VAS-QoL scores calculated before and during the pandemic were similar in Group 1 (p > 0.05 for each score). In Group 2, median values of VAS-symptom were higher during the pandemic than the pre-pandemic period while TSS-6 and MS were similar in both periods (p = 0.002, p > 0.05, p > 0.05). Also, median values of VAS-QoL decreased during the pandemic compared with pre-pandemic period in the same group (p < 0.001) (Figure 1).
In adherent patients, VAS-symptom increased and VAS-QoL decreased during the pandemic compared with the pre-pandemic period (p = 0.013, p < 0.001, respectively) and the median values of TSS-6 and MS were similar in both periods in adherent patients (p > 0.05 for each comparison). In nonadherent patients, median values of TSS-6, VAS-symptom, and MSs were higher and median value of VAS-QoL was lower during the pandemic than the pre-pandemic period (p < 0.001, p < 0.001, p = 0.005, p < 0.001, respectively) (Figure 2).
In the adherent and nonadherent patients, the correlation analysis between the duration of SCIT and changes in the different scores was performed and we could not show any significant correlation.
3.5 Evaluation of patients with concomitant asthmaComparison of ACT scores between and within the groups during the pandemic and pre-pandemic periods was similar (p > 0.05 for each comparison).
3.6 Correlation analysis between the delay in SCIT injections and changes in symptom, medication, and quality of life scores in pre-pandemic and pandemic periodsFirstly, the changes in MS, VAS-symptom, VAS-QoL, and TSS-6 scores between the pandemic and pre-pandemic periods were calculated. Then, the increased SCIT application intervals were assessed separately with the changes in these four scores with the correlation analysis. A moderate correlation between the increase in the interval of SCIT application and the differences in VAS-symptom (r = .509, p < 0.001), VAS-QoL (r = .516, p < 0.001), and TSS-6 (r = .521, p < 0.001) scores was observed. The difference in MSs between pre-pandemic and during the pandemic periods showed a very weak correlation (r = .188, p < 0.001) (Figure 3).

The correlation between delay in the SCIT application and changes of VAS-symptom, VAS-QoL, MS, and TSS-6. A = VAS-symptom, B = VAS-QoL, C = MS, D = TSS-6
3.7 AIT effectiveness and quality of life in patients diagnosed with COVID-19 infection during the study periodDuring the study period, 12 patients were diagnosed with COVID-19. The mean age of the patients was 37.5 ± 11.5, and 7 (58.3%) of them were female. Eleven (91.7%) patients had AR, and 1 (8.3%) had concomitant allergic asthma. In 9 patients (75.0%), AIT was for HDMs and in 3 patients (25.0%), it was for pollens.
Nine out of the 12 patients missed SCIT administration due to having COVID-19 infection whereas the remaining 3 patients had SCIT injections on time after completing the quarantine period. While 11 patients had mild symptoms, 1 patient had to stay in hospital due to severe COVID-19 disease.
TSS-6, VAS-symptom, and MSs of the patients (n = 3) who had administration on time were similar during pre-pandemic and the pandemic periods. Two out of the 3 patients had similar VAS-QoL scores during the pre-pandemic and the pandemic periods, whereas the pre-pandemic VAS-QoL score was 10 and pandemic score was 9 in the third patient. The TSS-6, VAS-symptom, VAS-QoL, and MS median (IQR 25-75) scores during the pre-pandemic period in the patients (n = 9) who missed administration were 3 (1–4), 3 (1–5.5), 8 (7.5–9), and 0 (0–1), respectively, and during the pandemic, they were 5 (2.5–14.5), 7 (3–9.5), 7 (2.5–7.5), and 1 (0–2), respectively.
4 DISCUSSIONOur study is the first multicenter study which has evaluated adherence to SCIT with aeroallergens during the COVID-19 pandemic and its influence on the short-term clinical outcomes in real-life. We observed that in half of the patients (53.8%), SCIT injections were delayed and one third (31.8%) of the patients were nonadherent during COVID-19 pandemic. Delays in SCIT administration have led to deterioration in the AIT effectiveness and QoL, and the deterioration was even greater in the nonadherent patients.
Adherence to long-term treatments in chronic diseases is very crucial for the success of the treatment.3 The definition of adherence to SCIT differs in studies; however, we referred to a previous study which was conducted by our group and considered the cutoff time interval for being nonadherent as 2 months accordingly.2 Moreover, we also determined the clinical results of shorter delays of less than 2 months in injection intervals in a separate patient group in order to strengthen our findings. By this way, we have captured all significant clinical consequences of delays in injection intervals. Since our study is the first adherence study during the pandemic, we could only compare our results with previous SCIT adherence studies published before the pandemic. In the majority of the adherence studies on SCIT, the adherence rates are less than 70.0%.2, 10-13 Furthermore, they are even lower according to real-life data.2, 14, 15 In our study, 68.2% of the patients were adherent to SCIT during the pandemic. We can speculate that this acceptable adherence rate in our study may be due to continuous treatment with appropriate preventive measures applied and the close cooperation that had been established between the allergists and the patients in the study centers before the pandemic despite the negative effects of the pandemic. In the centers of the study, in order to provide the close cooperation, the same allergy specialists observed the patients before and 30 min after each shot and the same allergy nurses applied the injections throughout the therapy. In every visit, the physicians evaluated the improvement of the clinical conditions, gave detailed information to the patients and specified the next injection appointment. As the clinical practice in SCIT visits has not changed during the pandemic, we believe the adherence rate observed during the study period reflects the influence of the pandemic on SCIT adherence in our patients.
As a main finding of our study, delay in SCIT administrations led to deterioration in AR symptoms and QoL of our patients. Delays of less than 2 months between subsequent SCIT injections worsened QoL and symptom scores in Group 2 patients, whereas in the nonadherent group MSs were additionally disrupted. This disruption is due to the fact that anti-allergic medication was needed to relieve their symptoms. Therefore, we suggest that it is important to continue SCIT injections without extending intervals more than recommended in order not to affect the short-term effectiveness of AIT even during a pandemic.16 Prolonged intervals in the SCIT applications are also an important issue to make appropriate dose adjustments to restart SCIT after gaps in the administration.17 In our study, after interruptions of maintenance doses especially in nonadherent patients, dose adjustments starting with frequent lower dose injections caused frequent hospital visits which can probably bring additional burden on the healthcare system.
The two main reasons of nonadherence to SCIT in our study were using public transport for reaching the hospital and receiving SCIT with HDMs. In accordance with our findings, a study from the USA reported that one of the reasons of premature cessation of SCIT was the inconvenience of travel.
留言 (0)