
記住我

Since late 2019, coronavirus disease 2019 (COVID-19) has spread rapidly worldwide. Due to the high transmission rate, health care workers (HCWs) are required to wear face personal protective equipment (F-PPE) for several hours each working day.1, 2
The skin is the body's defense against the environment; it is constantly exposed to external factors. The protective function of the skin is altered when it is constantly aggravated by the continuous use of F-PPE. The skin is repeatedly subjected to physical and chemical factors, such as friction, tension, and pressure, as well as moisture, humidity, and heat.3, 4 This is associated with the development of friction injuries, skin breakdown, and pressure ulcers.3
During the severe acute respiratory syndrome epidemic in 2003, N95 mask–related adverse skin reactions (ASRs) among Singaporean HCWs included acne, facial pruritus, and rash.5 In the current COVID-19 pandemic, cross-sectional surveys and several case reports have described ASRs related to the use of F-PPE.1, 2, 6-15 The most frequently reported ASRs were dry, itchy, red, scaly, macerated, and/or painful skin, as well as pimples, buds, fissures, scratch marks, pressure marks, and ulcers. A systematic review highlighted cases of occupational dermatitis associated with F-PPE and pointed out the need for well-designed studies to better understand the incidence and management of mask-related dermatitis.6
Studies have described a correlation between skin types and dermatological diseases, for example, acne and atopic dermatitis.16-18 Additional studies have shown that prolonged use of F-PPE can result in the worsening of chronic skin diseases, such as acne or atopic dermatitis.2, 15
In this study, we examined the use of F-PPE, including surgical masks, particulate respirators (FFP3/N95), goggles, and facial shields. The use of different types of F-PPE was based on the recommendations of the authorities. For example, surgical masks were recommended for use in all public indoor areas, whereas FFP3 were prescribed for specific situations for example, caring for patients with COVID-19.
The objectives in this study were to describe self-reported ASRs among HCWs using F-PPE during the COVID-19 pandemic; investigate background factors, such as chronic skin diseases and skin types (dry, oily, combination, sensitive); and determine whether HCWs had taken preventive methods against ASRs.
2 METHODS 2.1 Ethical considerationsThe study was approved by the Danish Data Protection Agency (approval number: P-2020-621) and the crisis management leaders of the Capital Region of Denmark. The research was conducted in accordance with the Declaration of Helsinki. Respondents were informed in writing about the study's objectives and their rights, including anonymity and the freedom to participate voluntarily.
2.2 Survey and participantsThe survey was designed as an online questionnaire (SurveyXact; Rambøll, Oslo, Norway). The questionnaire was developed based on literature review and it included questions on ASRs, chronic skin diseases, allergies, skin types, risk factors, prevention, and treatments.5, 6, 16-18 The survey questions related to ASRs that occurred between October 1, 2020 and February 28, 2021. The questionnaire was emailed to HCWs at six hospitals in the Capital Region of Denmark in February 2021. Reminders were sent to non-respondents after 1 and 3 weeks.
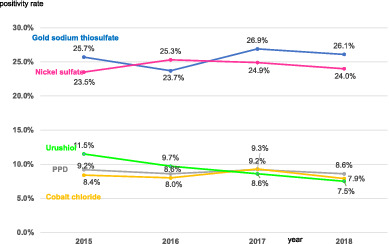
In total, the questionnaire was sent to 22 993 HCWs, of whom 11 855 did not respond, and 622 had an incomplete response (Figure 1). In the analysis of the respondent group (n = 10 516; 45.7%), we excluded HCWs whose answers were invalid, such as those who worked for >168 hours a week, were aged >100 or <18 years old (n = 136), and who did not use F-PPE (n = 93). If participants reported ASRs, they were reported as having ASRs related to the use of one or more types of F-PPE.

Flow chart of participants and drop-outs in the study of adverse skin reactions among health care workers at six Danish hospitals
2.3 Statistical analysesChi-square tests were used to investigate associations between categorical variables. Analysis of variance was used to test differences in age and working hours. Binary logistic regression was used for multiple variable analysis of the risk for ASRs. A P-value of <.05 was considered statistically significant. Statistical analyses were performed using SPSS Statistics for Windows (version 25.0; IBM Corporation, Armonk, New York).
3 RESULTSThe analyzed population comprised 10 287 HCWs (44.7% of 22 993 invited participants) employed at six hospitals in the Capital Region in Denmark. The population consisted of 8854 women, and 1433 men, with a mean age of 44.8 years, and included nurses, physicians, nursing assistants, physiotherapists, radiographers, midwives, and occupational therapists (Table 1). The HCWs were associated with inpatient care (42.3%), outpatient clinic including radiotherapy (36.6%), operating theatre (7.7%), intensive care unit (7.0%), department of anesthesiology (4.9%), or recovery room (1.7%) (Table 2).
TABLE 1. Professions and background of study participants, n (%) Use of F-PPE in a day n (%) Age mean (SD) Sex, male Adverse skin reactions Working hours/week, mean (SD) <3 h/day 3-6 h/day >6 h/day All 10 287 44.8 (12.4) 1433 (13.9) 6372 (61.9) 34.9 (5.6) 692 (6.7) 2891 (28.1) 6704 (65.2) Nurses 5924 (57.6) 44.2 (12.4) 311 (5.2) 4057 (68.5) 34.1 (5.1) 289 (4.9) 1377 (23.2) 4258 (71.9) Nurse assistants 800 (7.8) 52.1 (11.3) 47 (5.9) 509 (63.6) 32.7 (5.9) 31 (3.9) 165 (20.6) 604 (75.5) Physicians 2330 (22.6) 45.3 (12.1) 890 (38.2) 996 (42.7) 38.0 (5.5) 312 (13.4) 930 (39.9) 1088 (46.7) Physiotherapists 376 (3.7) 42.4 (11.9) 84 (22.3) 225 (59.8) 34.9 (4.3) 21 (5.6) 223 (59.3) 132 (35.1) Occupational therapists 131 (1.3) 39.4 (11.0) 14 (10.7) 90 (68.7) 35.4 (3.5) 6 (4.6) 59 (45.0) 66 (50.4) Midwives 351 (3.4) 42.1 (12.7) 2 (0.6) 249 (70.9) 32.1 (5.6) 13 (3.7) 28 (8.0) 310 (88.3) Radiographers 375 (3.6) 42.6 (12.0) 85 (22.7) 246 (65.6) 35.6 (4.8) 20 (5.3) 109 (29.1) 246 (65.6) Pearson's chi-square test, P-value .001 <.001<.001
ANOVA, P-value <.001 <.001 Abbreviations: ANOVA, analysis of variance; F-PPE, face personal protective equipment; SD, standard deviation. TABLE 2. Adverse skin reactions (ASRs) related to departments and different types of masks, n = 10 287, n (%) F-PPE ≥1 types Surgical masks FFP3 used, n = 10 287 With ASRs, n = 6372 used, n = 9946 With ASRs, n = 5910 used, n = 4735 With ASRs n = 2156 In-patient care 4350 2951 (67.8) 4201 2756 (65.6) 2352 1076 (45.7) Outpatient clinic incl., for example, radiotherapy 3748 2016 (53.8) 3578 1890 (52.8) 1042 417 (40.0) Operating theatre 791 436 (55.1) 786 411 (52.3) 371 124 (33.4) Intensive care unit 716 540 (75.4) 708 468 (66.1) 511 330 (64.6) Department of anesthesiology 509 305 (59.9) 505 269 (53.3) 384 173 (45.1) Recovery room 173 124 (71.7) 168 116 (69.0) 75 36 (48.0) P-value <.001a <.001a <.001a Abbreviation: F-PPE, face personal protective equipment. Note: % with ASRs in the specific departments.On a working day, HCWs used one or more F-PPE (surgical masks [n = 9946], FFP3 [n = 4735], face shield [n = 6342], and/or goggles [n = 4955]) (Tables 2 and 3). Approximately 50% of them used both surgical masks and FFP3 (n = 4735), whereas others used only surgical masks (n = 1889), FFP3 (n = 61), goggles (n = 12), or face shields (n = 97).
TABLE 3. Different kinds of F-PPE and associated adverse skin reactions (ASR) and skin symptoms, n = 10 287, n (%) Surgical masks FFP3 Face shields Goggles Used, n 9946 (96.7)a 4735 (46.0)a 6342 (61.7)a 4955 (48.2)a Used without ASRs 4036 (40.6)b 2579 (54.5)b 5230 (82.5)b 4644 (93.7)b Used with ASRs 5910 (59.4)b 2156 (45.5)b 1112 (17.5)b 311 (6.3)b Use F-PPE in h/day <3 h 352 (32.8)b 1042 (48.3)b 357 (32.1)b 105 (33.8)b Between 3 and 6 h 1696 (32.7)b 721 (33.4)b 448 (40.3)b 113 (36.3)b >6 h 3862 (44.9)b 393 (18.2)b 307 (27.6)b 93 (29.9)b P-value = differences between use of hours of the F-PPE <.001c <.001c <.001c <.001c Greasy or sticky skin 1038 (10.4)b 313 (6.6)b 187 (2.8)b 27 (0.5)b Itchy skin 2911 (29.3)b 1037 (21.9)b 485 (7.6)b 48 (1.0)b Dry or scaly skin 2134 (21.5)b 654 (13.8)b 186 (2.9)b 31 (0.6)b Red and irritated skin 3518 (35.4)b 1293 (27.3)b 482 (4.6)b 80 (1.6)b Swollen and irritated eye area 759 (7.6)b 302 (6.4)b 82 (1.3)b 45 (0.9)b Spots or pimples 3697(37.2)b 1013 (21.4)b 339 (5.3)b 39 (0.8)b Tender, burning, or painful skin 1032 (10.4)b 434 (9.2)b 116 (1.8)b 31 (0.6)b Fissures 351 (3.5)b 94 (2.0)b 23 (0.4)b 7 (0.1)b Macerated and exuding skin 83 (0.8)b 36 (0.8)b 16 (0.3)b 1 (0.0)b Pressure mark 1254 (12.6)b 1125 (23.8)b 456 (7.2)b 203 (2.0)b Pressure ulcer 167 (1.7)b 126 (2.7)b 36 (0.6)b 26 (0.3)b Abbreviations: F-PPE, face personal protective equipment.Of the study population, 61.9% self-reported ASRs of the face related to the use of one or more types of F-PPE (Table 1). The ASRs included itchy skin, dry or scaly skin, red and irritated skin, greasy or sticky skin, swollen and irritable eye area, spot or pimples, tender skin, burning or painful skin, fissures, macerated and exuding skin, pressure marks, and ulcers (Table 3).
The sites of ASRs included the area around the mouth (n = 3583), cheeks (n = 3541), chin (n = 3419), nose (n = 3042), ears (n = 1191), eyes (n = 976), forehead (n = 732), and neck (n = 779).
In the six hospitals, there were no statistically significant differences in the frequency of ASRs (P = .40). The frequency of ASRs was related to the department where the HCWs worked (Table 2). For example, the frequency of ASRs was significantly higher in intensive care units (F-PPE, 75.4%; surgical masks, 66.1%; and FFP3, 64.6%) than in the department of anesthesiology (F-PPE, 59.9%; surgical masks, 53.3%; FFP3, 45.1%) (P < .001).
3.1 SexThe frequency of ASRs was significantly higher in women (n = 5832; 65.9%) than in men (n = 540; 37.7%) (P < .001). Some female HCWs (n = 3573; 40.4%) applied make-up under the F-PPE. However, there was no significant difference in the frequency of ASRs between women who did (n = 2328; 65.2%) and did not (n = 3504; 66.4%) apply make-up (P = .25).
Men with beards (n = 694) reported significantly more ASRs (n = 285; 41.1%) than those without (n = 255; 34.5%) (P = .012).
3.2 AllergiesNearly one third of HCWs had allergies (n = 3046; 29.6%) to pollen (n = 1960;19.1%), house dust mites (n = 1099; 10.7%), furred animals (n = 889; 8.6%), nickel (n = 674; 6.6%), perfume (n = 465; 4.5%), adhesive tape (n = 234; 2.3%), and latex (n = 208; 2.0%). HCWs with allergies reported ASRs significantly more frequently (n = 1972; 64.7%) than HCWs without allergies (n = 1074; 60.8%) (P < .001).
3.3 ProfessionsPhysicians reported significantly less ASRs (42.7%) than nurses (68.5%), nurse assistants (63.6%), physiotherapists (59.8%), occupational therapists (68.7%), midwives (70.9%), and radiographers (65.6%) (P < .001) (Table 1).
3.4 Duration of F-PPE useThe study population worked for a mean of 35 hours per week (standard deviation: 5.6). This is the typical number of working hours for HCWs in Denmark (Table 1). Most respondents used F-PPE daily (85.4%), followed by 3-4 days per week (11.3%), and 1-2 days per week (3.3%). F-PPE was worn for >6 hours per day (65.2%), followed by 3-6 hours per day (28.1%), and < 3 hours per day (6.7%). The differences in frequencies of ASRs were associated with the duration of F-PPE use. ASR differences between F-PPE use >6 hours per day (n = 4585; 69.9%), 3-6 hours per day (n = 1520; 52.6%), and < 3 hours per day (n = 167; 24.1%) were statistically significant (P < .001).
3.5 Chronic skin diseasesOne fifth of respondents (19.1%) reported chronic skin diseases, such as atopic dermatitis (5.4%), rosacea (4.0%), psoriasis (3.9%), acne (3.7%), seborrheic dermatitis (1.4%), and other skin diseases (hand eczema [n = 308], urticaria [n = 32], periorbital dermatitis [n = 41], and perioral dermatitis [n = 41]) (Table 5). The proportion of HCWs who received treatment for chronic skin diseases was 7.6% (n = 778). Treatments included topical corticosteroids (n = 582), tacrolimus (n = 41), ketoconazole (n = 17), antihistamines (n = 29), and various treatments for acne and rosacea (n = 178).
The frequency of ASRs was significantly higher in HCWs with chronic skin diseases (n = 1407; 71.6%) than in those without (n = 4965; 59.7%) (P < . 001). This was also true for acne (84.2% vs 61.1%; P = .001), atopic dermatitis (72.3% vs 61.3%; P < .001), and rosacea (79.6% vs 61.2%; P < .001), but not for psoriasis (66.5% vs 61.8%; P = .10) (Tables 4 and 5).
TABLE 4. Chronic skin diseases, adverse skin reactions (ASRs), and skin symptoms related to F-PPE use, n = 10 287 with ASRs, n (%) Total Acne AD Rosacea Psoriasis
留言 (0)