
記住我

The aim of this paper is to pay close attention on a phenomenon that for the past few years has become rather widespread among adolescents and young adults in many countries. This particular form of social withdrawal was observed for the first time in Japan and was thoroughly described by the Japanese psychiatrist Saitō (1988), who called it “hikikomori.” This term describes the voluntary self-reclusion, in their own homes, of adolescents and young adults who do not show clear signs of psychological distress or of mental illness. Several research studies have shown that young hikikomoris do not exclusively live in Japan but also in several Eastern and Western countries such as Oman, China, Korea, Spain, France, United States, Australia, and United Kingdom (1, 2) and Italy (3, 4). This phenomenon is so widespread that one might think that such an issue goes well beyond the range of a specific socio-cultural context (5).
In the course of the past few years, several adolescents coming to the UFSMIA (Functional Mental Health Unit for Children and Adolescents) of Arezzo, Italy, have shown behaviors that are altogether similar to those described by Saitō1. To begin with, these young people did not go to school and never left their homes. These behaviors were accompanied by a progressive abatement of the relationships with their peers and the withdrawal in their own rooms. The sleep-wake cycle showed a remarkable inversion. The time they spent in the room passed without their doing anything or, in the best cases, engaging in solitary activities, like drawing, playing video games, reading comic books, or surfing the web, but always without any contacts with social networks or masturbation. Family relationships seemed to feature a typical constellation: a long-time absent father who, despite his current availability, was unable to recover the relationship with his son/daughter, and a mother strongly attached to her son but constantly anxious, for a number of different reasons about his actions and choices, and unable to properly manage her relationship with him and to set any limits. Almost all of these hikikomori boys and girls had one or more pets, often dogs and sometimes cats, which they saw as very young children that they had to look after with the utmost care and affection. There was no mention of eating disorders or of symptoms that might relate to full-blown psychopathological conditions. It was, however, possible to detect a condition of emotional fragility which, at least in the initial stages, made it difficult to establish a significant therapeutic relationship. This paper aims at illustrating the current scientific debate and to integrate it with the account of a clinical case, which will present the modalities of intervention at the UFSMIA.
Hikikomori: a debate on a 21st century phenomenonWhat drives hikikomori adolescents to withdraw from the world is something different from a manifest mental illness like schizophrenia or any disorder in the autistic spectrum, intellectual disability, or the classic symptoms of a depressive state. The Japanese Ministry of Health has widely researched the phenomenon in 2003, and then again in 2010 and 2016 (6, 7)2, and it has drafted some guidelines, in which it is stated that the hikikomori condition cannot be considered as a syndrome but rather as a psychosocial phenomenon. The Japanese Ministry’s criteria for identifying a hikikomori are the following: this is a condition that affects children, adolescents, and young adults younger than 30 years; their lifestyles are centered on their own homes; their more or less complete withdrawal from society continues for at least six months; a rejection of school and/or work is also present; those who leave their school or their jobs but keep maintaining relationships with their peers outside their own families are not considered as hikikomori; and among the hikikomori population, there may be future patients with schizophrenia, who are included in this group until their mental illness becomes evident.
In the course of the past 20 years, many different hypotheses have been formulated regarding the origin of the hikikomori phenomenon. Some authors claim that this form of withdrawal is of an exclusively psychosocial character. Hikikomori is not a label indicating mental illness but simply a term used to define a condition (12), a state not caused by a mental illness (13), and not a symptom that accompanies a mental disorder (14). In agreement with these positions, sociological and anthropological research studies highlight how these young people’s behavior may be interpreted as a way to avoid the pressures of society, school, and parents (15, 16) or the difficult access to the job market caused by the economic changes that penalize the new generations (8). The behavior of the hikikomori would then be an act of withdrawal from socially shared constraints of time and space in a sort of reaction to the pressures for the pace and performance that must be achieved (17), a form of silent protest (18) against a society, school, and family that – even at the cost of hiding the psychological dimensions underlying this kind of social withdrawal – seem to favor a more traditional cohesiveness among the members of their communities, rather than the right to be different (10). Hikikomori individuals would then constitute a sort of hidden juvenile subculture that deals with the problems of traditional society, like exclusion, bullying, and discrimination, by withdrawing and renouncing their own social status (19).
Distancing themselves from the opinions expressed in the previous paragraph, several authors see the hikikomori condition as a psychopathological syndrome; some psychiatrists attribute the same condition to pre-existing diagnostic categories (20); for some others the hikikomori condition is a form of “modern-type depression” (21); and for others, who think it cannot be classified as a psychiatric disorder already included in the DSM (22) or the ICD (23); it would be necessary to assess whether it is appropriate to insert this condition in a culture-bound syndrome or define it as a new form of psychiatric disorder (24). The psychiatric assessment of adolescents and young people in a hikikomori condition is made even more complex by the fact that self-reclusion, albeit voluntary, may in itself determine the development of psychopathological symptoms that range from insomnia to the acute reversal of the sleep-waking cycle, from anxious states to obsessive-compulsive disorders and from regression to infantile behavior to domestic violence (25); thus, making any attempt at defining unequivocal diagnostic criteria is very complex indeed.
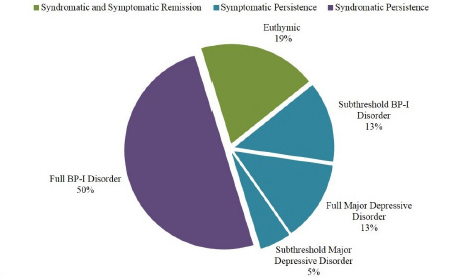
Many authors differentiate between two kinds of hikikomori: a primary type, in which this state should not be considered as a mental illness but rather as a condition that implies behavioral problems, and a secondary type, characterized by a pervasive developmental disorder (26, 9). The clinical experience of our Mental Health Unit belongs to the second type. The subdivision of the hikikomori population into two groups, primary and secondary, has found confirmation in an epidemiological research study on the relationship between the hikikomori condition and psychiatric disorders, which was carried out as a part of an initiative of the World Mental Health Survey Initiative (WMH-J)3. The survey showed that about half of the sample of interviewed hikikomori individuals displayed social withdrawal in comorbid with a psychiatric disorder (mood disorders, anxiety, impulse control disorders, or substance-related disorders), whereas the other half of the sample did not show any comorbidity (28). The concept of primary hikikomori has been criticized and defined as a paradox, a psychiatric category created in order to single out those who do not belong to the psychiatric field of research (29). However, the grouping of one part of the cases of social withdrawal under the category of primary hikikomori has made it possible to get out of the constraints of a rigid psychiatric classification, with the possibility of paying more attention to the relational, developmental, and psychological aspects that characterize the life course of these adolescents (30).
Among the main risk factors for the development of a hikikomori condition, there is a temperamental predisposition to withdrawal; an early mother-child altered relationship, sometimes conditioned by cultural factors; an insecure-ambivalent attachment style; and family relationships featuring an overprotective mother, extremely attached to her child, on one hand, and a substantially absent father on the other (31). The child who is developmentally at potential risk of social withdrawal is often the depositary of the idealizations and the great expectations of the mother, and he feels the obligation to emulate his distant father, as well as to replace him in the relationship with the mother (32). When, in the course of childhood, this kind of relational constellation has been established, a single triggering event in early adolescence (bullying episodes, but also a lack of integration in the peer group, or even simple requests from the school, experienced as excessive) may be enough to drive an adolescent to forms of withdrawal that can be more or less accentuated, and more or less severe, according to the internal organization that has been developed in the course of the young person’s growth (33). Social withdrawal manifests itself in a continuum that ranges from a general predisposition to being on one’s own to the condition of an extreme form of social withdrawal (34).
In a research study on the psychosocial factors leading to withdrawal in the course of a young person’s development, Krieg and Dickie (35) observed that the sample hikikomori participants, unlike the subjects of the control group, displayed a shy temperament and an ambivalent style of attachment. These young persons reported that during their childhood, on many occasions, their parents had threatened them with the possibility of interrupting any relationship with them4, and that in their early adolescence, but not during their primary school period, they had been rejected and bullied by their peers. According to the authors, a shy temperament is not a predictor of a hikikomori condition. Only the combination of a particularly negative growth process with uncaring parent-child relationships, the development of an anxious-avoiding attachment, and episodes of rejection and bullying in early adolescence can lead to extreme social withdrawal.
According to Hattori (37), the hikikomori condition originates from traumatic conditions experienced in early childhood. In a research study carried out by this author, none of the 35 young hikikomori participants displayed a secure style of attachment, and all of them reported negative experiences and rejection on the part of their parents. For Hattori, to adapt to emotionally dysfunctional parents, these hikikomori patients had repressed their emotions and original personalities, creating a false identity for themselves. Moreover Suwa and Suzuki (9) dwell on the issue of the construction of a false identity in the history of hikikomori adolescents. The five main characteristics that can be helpful in the identification of primary hikikomori patients are the aspects and the consequences of the process of constructing a false identity: a strong investment of the parents in their child’s ideal self; an image of the ideal self originating from other people’s desires rather than from one’s own; the necessity or the need to preserve the self-image expected by other people; an avoidant behavior aimed at maintaining a positive assessment of one’s self on the part of other people; and episodes of “defeat without a struggle,” that is of an a priori relinquishment of one’s objectives.
These research studies seem to confirm what we know about social withdrawal in infancy. The newborn’s biological and temperamental characteristics, the mother-baby relationship, and the type of attachment that is established between the neonate and the caregiver are predictors of the future inhibited behaviors of the child and the adolescent (38). The early interactions between babies and parents are crucial for the construction of a secure attachment (39, 40). When the newborn finds self-regulation difficult and is looked after by relatively insensitive parents, an insecure attachment is very likely to occur, negatively affecting the baby’s future social behavior, establishing distressing relationships and difficult internalization processes (41).
The hikikomori behavior originates in infantile relationships, when developmental drives are inhibited and distorted by the need to fulfil the needs of other members of the primary group. The child in a hikikomori family usually serves as a support for the mother in the management of anxieties that she is unable to manage, either because she lacks the adequate cognitive and affective tools or because of the limited support of her partner, who is emotionally distant from the life of the family. The mother puts herself at the center of her child’s psychological world, relinquishing her support to his personal and emotional growth in the shared mental space of their intersubjective relationship. The form of attachment that is created is of an insecure-ambivalent type. Having experienced the unpredictability of the maternal figure, the baby tries to keep extremely close to her, renouncing any autonomous exploration. If the child, once he becomes an adolescent, is forced to face a rejection from his peers, either because he is isolated, bullied, or unable to keep up with his schoolmates’ academic performances, the likelihood of a voluntary withdrawal becomes much greater (42).
Treatment of acute social withdrawal in adolescenceMental health professionals generally believe that a condition of acute social withdrawal needs professional support (43). At the same time, the condition of self-reclusion, albeit originating from a voluntary act, is very often experienced by the adolescent with anxiety or irritation (28). Despite the subjective experience of discomfort and the distressing feeling of being unable to interrupt this state of isolation, it is quite difficult to get the adolescent involved in a treatment. The establishment of a single contact may represent the final aim of many months of intervention, and the attempts of a single clinician or an attending team may not necessarily have a positive outcome. Several different approaches may be tried, for example, preliminary interviews with the parents, house visits, and attempts at establishing contact by phone, e-mail, and social networks (44, 45). After the start of the treatment, it must be constantly modulated according to the characteristics of the withdrawal, as the condition of the young person gradually changes. The current experiences at the UFSMIA in Arezzo aim for rehabilitative-therapeutic strategies that can be differently modulated for each case, rather than defined a priori within a specific protocol.
On a number of occasions, a combination of individual psychotherapy and family interventions (family consultations or psychotherapy), sometimes associated with programs run by social workers, has resulted in a reactivation of the patient’s social contacts and relationships with other people. In other cases, additional forms of intervention become necessary: from psychopharmacological treatments to reports to the juvenile court, with the activation of the social services for the removal of adolescents from their family and their placement in a community. The single program is progressively adjusted according to the psychological and human resources of the family and the single adolescent, to the degree to which the family relationship are compromised, and with regard to the response given to the interventions that have been suggested (33). What follows is a part of a rehabilitative-therapeutic treatment, which was activated at the UFSMIA of Arezzo, to illustrate this presentation and to contribute to the discussion. This case is representative of the UFSMIA’s clinical approach. Other similar cases are reported in previous articles (42, 46, 33).
A 15-year-old girl, whom we will conventionally call B 5, dropped out of school because of many absences and after failing an oral examination. She was attending her last year of middle school. The drop out was a surprise for the school. Seemingly, B had a good relationship both with her teachers and her peers and her overall school results were not so bad. A few months later, the school reported her absence to the authorities (school attendance is compulsory in Italy until the age of 16 years), and after several failed attempts at resolving the situation, the appointed social worker contacted the UFSMIA. During the first interview with B’s parents, the psychologist realized that it would be difficult to meet the girl: B no longer left her home, she interrupted all her social relationships, and she clearly did not accept any form of intervention. The decision was made to keep seeing the parents for a number of meetings, waiting for B (who had also been invited) to join them. During the meetings, the parents reported that B had always been a kind and obedient child. When she was a little girl, B enjoyed playing with the children she met at the park near their house. In the memories of the couple, B had been a very quiet and nice little girl. About two months passed before B decided to take part, albeit silently, in one of these encounters with the psychologist and her family. At the end of the meeting, the clinician asked B to spend some time with her alone. The interview lasted not more than ten minutes. B appeared to be a fragile young girl; when asked a few questions, she reacted by trembling and replying with one-word answers. That would, however, mark the beginning of a long psychotherapeutic treatment.
Her family history is complex. Her mother, a woman in her mid-forties, apparently extroverted but actually very reluctant to engage in social relationships, had always lived at home with her parents, now deceased. As an adult, she met B’s future father, a skilled worker of her age, who came to town from another region looking for a job. The man, who constantly had to travel for his job, began to spend time with her, undergoing long journeys. Their lifestyle did not change after the birth of B, who was in fact brought up by her grandparents and by the mother, in the absence of the father. The grandparents passed away when B was a child, but this, once again, did not change the couple’s lifestyle. B’s father came back home for brief periods of time, being away for work even for months, whereas the mother looked after the house and the child.
The therapeutic-rehabilitative program that was initiated included weekly individual psychoanalytical psychotherapy with the patient, family meetings every three weeks, and a monitoring activity on the part of the social worker, who also liaised with the school and with the juvenile court. Staff meetings for intervision activity were scheduled every 45 days. Once the psychotherapy started, the mother always took the girl to her sessions. B often brought one of her dogs with her in the consultation room. The mother, in turn, always came with her partner, and in the periods of his absence, a neighbor came with her. The first sessions were difficult. Every contact with B, even visual contact, was difficult. When B understood that she could talk about what she wanted, that the sessions were not an attempt to bring her to school and that the psychotherapist had a sincere interest in her, the therapeutic relationship progressively improved. B showed a great interest in rap music and in her four dogs, which she looked after as if they were her children. She never talked about her school, a topic which for her was too painful and difficult to face. About a year later, things seemed to have improved: B tried to go out, initially only in the evening, to walk her dogs, then she started to go out with a friend for a walk, and finally she began going out with a small group of girls her age. The contents of the sessions became deeper: the girl seemed to explore the world (relationships, feelings, and affects) through the words of her favorite rap singers, bringing to her psychotherapist several notebooks in which she had written down all the songs’ lyrics. On a number of occasions, the discussion on a few lines of these songs filled the entire session. One day, B said something about her parents. Until that moment she had always provided a softened, quickly sketched image of them, whereas on this occasion she said, “They are always quarrelling.” Such rows, which had been kept accurately hidden, were constant, made more serious by a period of unemployment of B’s father and by his forcedly prolonged permanence at home. B took his side, criticizing her mother for her ways, her rejection of any possible change, and for her closure to the external world. During the summer, the father suggested they should go on holiday to his native region, as they had done in the previous years. His partner refused to go, making futile excuses. So the man left and B went with him, the two of them being alone for the first time. When B came back, she talked about the incessant phone calls from her mother, with her constant requests for contact, and of the week that ended with her mother’s admission to the local emergency room because of an undefined illness. Despite all these calls, father and daughter did not renounce their holiday plans, a full week, and they went back home just when they had planned to. For the first time B wondered whether her parents would split. B’s mother, clearly in trouble (anxious attacks as well as a partial alteration of her sense of reality), saw her daughter’s psychotherapist, asking for his help. He took this opportunity to refer her to the Service of Mental Health for Adults, where she was assessed by a psychiatrist and later offered a psychological treatment. Meanwhile, B seemed to be full of projects: she wanted to learn how to play guitar, to cook, and maybe even to find a job. Father’s going back to work after a long period of unemployment, however, led the girl to a state of gradual social withdrawal. Once again B showed her inability to carry out her plans by herself, expecting to be helped by her mother who, instead, managed to hinder her daughter in many ways, for example, by postponing her visit to a youth center where guitar courses were held, by not having B’s mobile fixed and by constantly using the home PC to surf the internet and use various social networks. Despite all these difficulties, B gradually seemed to recover, and she even found a friend, which allowed her to have some social experiences of her own. One day she presented her psychologist with a cake, the first that she made by herself. B’s attempts at autonomy once again turn into conflicts in the parental couple, but during one of the rare family meetings, made even more infrequent because of the father’s absence, after a heated discussion owing to financial reasons, B’s mother, for the first time, expressed her need to go back to work. To the psychotherapist’s surprise, B’s father stated that he was the Male in the family and therefore he had to provide for his family’s support. “That is the reason why I never accepted that my partner goes to works; however, considering the current crisis and our financial problems …” At that point, B, who had been silent until then, took advantage of the situation to say, to the surprise of both parents, that she, too, would like to find a job. Thus, in the session, the rigid roles that imprisoned each participant were disclosed. Just a fortnight later, a new dramatic turn of events took place: nobody talked about finding a job, but B’s mother asked her partner to marry her. They started a discussion in which their positions seemed to become even clearer: a couple that had never really become a proper one, and a daughter waiting for her parents to make up their minds about her destiny, as well as theirs. On this occasion, the therapist utilized the metaphor of the “waiting room”: it was as if B were at the station, waiting for a train which would never arrive.
ConclusionsThe research studies that compare the therapeutic-rehabilitative programs carried out in different countries with young and adolescent hikikomoris indicate that the individual psychotherapeutic approach constitutes the preferred treatment, followed by those based on a combination of psychotherapy and pharmacological therapy (47). Moreover, other approaches are described in the current literature, such as family therapy, socio-rehabilitative treatments, home visits or web-medicine interventions for completely self-retreated hikikomoris. To these, we can also add support groups for young people and their families, as well as community treatments with educational and/or psychotherapeutic approaches (48). On the basis of its own clinical experience, the UFSMIA of Arezzo has articulated an approach based on several interventions, fine-tuned for each case and each individual moment. No rigid protocol was defined, rather therapeutic programs are organized following a careful assessment of the degree and the typology of social withdrawal, its comorbidity with other clinical conditions, the existence of withdrawal-based psychopathological symptoms, and the personal and family resources that can be activated (49, 50). The actions of different professionals (child neuropsychiatrists, psychologists, teachers, social, and community workers) must be combined and arranged according to the concept of modularity (51), which should aim each single intervention at well-defined and specific objectives within a wide-ranging clinical project. Failure to consider the overall condition of young hikikomori patients and simply aiming at partial therapeutic treatments for their social adjustment, more than for their personal needs (e.g., forcing them to go back to school, not considering their subjectifying needs, which are typical of adolescents), may represent a dangerous attack on their possibility of reaching a personal harmony of their own (52), which can harm their mental health. The clinical case presented in this paper highlights the interconnections between the individual difficulties of the patient, the relational dysfunctions of her family, and the effect of socio-cultural factors. Such a condition entails the need to work on several levels simultaneously. Only a constant monitoring of the sense of social withdrawal for young people and their families will allow a working group to find their bearings and dynamically interface with the patient’s needs. This choice implies an exercise in institutional flexibility and tolerance. The Mental Health Service allows for individual room for maneuver, helping patients not to transform their attempts to re-enter into the community in traumatic experiences that might once again promote social withdrawal. Professionals stand by these young people so that they can make further steps in acknowledging and developing their personal pathways, even when they diverge from the ones planned by their adults of reference. Following Li and Wong (31), interpretations of acute social withdrawal can be very different, either negative or positive. Our clinical perspective is that for confused adolescents going through a transitional period, social withdrawal can be a form of psychological moratorium to regain control over the environment and gradually reestablish direction, and reconstruct identity (13). A good clinical intervention aims at facilitating their evolutionary need.
留言 (0)