
記住我

Clinic and epidemiologic studies strongly support the notion that pediatric bipolar (BP)-I disorder afflicts a substantial number of children and adolescents, and its presence is associated with high levels of morbidity and disability (1-3). Although longitudinal course is a key validation criteria for any psychiatric disorder, relatively few studies have assessed the persistence of the disorder over time (4). Geller et al. (5) reported that 44% of children with BP-I continued to have the full disorder by the age of 18 years. Birmaher et al. (6) reported a chronic course of pediatric BP disorder with high rates of relapse and recovery (63% and 82%, respectively) as well as high rates of persistence of subsyndromal presentations and episodes of depression.
For BP disorder, remission from both mania and depression is relevant in follow-up studies assessing the patterns of persistence and remission. However, very few longitudinal studies of pediatric BP disorder have considered the many different forms of persistence. Such forms include not only the persistence of the full threshold disorder but also the persistence of subsyndromal states such as hypomania or cyclothymia.
We recently reported results from a 4-year follow up of 78 youth with the onset of pediatric BP-I disorder, attending to these different definitions of persistence (4). Findings revealed that most youth with BP-I disorder at baseline (73.1%) continued to meet full Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) diagnostic criteria for BP-I disorder at follow up (i.e., syndromatic persistence). Of the non-persistent cases, or cases that did not meet criteria for full BP-I disorder at follow up (26.9%), the overwhelming majority (20.5%) had signs and symptoms of ongoing illness: 6.4% had subthreshold BP-I disorder, 5.1% had no mania but had full or subthreshold major depression, and 9% were euthymic but treated for a mood disorder. Considering the severity of these outcomes, corroboration of these findings is clinically and scientifically important. Longitudinal course/persistence is a cornerstone of the validation of any disorder. This report is one of only three longitudinal studies of pediatric BP disorder, a highly morbid condition. Our focus on the different forms of persistence is a clinically and scientifically relevant way to interpret longitudinal data. Few longitudinal studies of pediatric BP disorder have considered the many different forms of persistence. Such forms include not only the persistence of the full threshold disorder but also the persistence of subsyndromal states such as hypomania or cyclothymia. The persistence of full threshold and subsyndromal depressive and manic states, individually, has also been minimally explored.
To this end, the main aim of the present study was 2-fold: to conduct a 1-year follow-up study in which the methods replicate our previously reported 4-year follow up of our sample of pediatric BP-I disorder, confirming the high level of persistence documented; and to attend to different definitions of remission at follow up, including persistence of the full diagnosis of BP-I disorder as well as the presence of subsyndromal mania and depression. We hypothesized that the persistence of pediatric BP-I disorder would continue and that subsyndromal states would continue to be highly represented into adolescence.
Methods SubjectsWe recruited 105 youths in a longitudinal follow-up study of BP-I disorder. Detailed study methodology has been previously reported (4). Potential BP-I disorder probands were ascertained for a family study of BP disorder from the Clinical and Research Programs in Pediatric Psychopharmacology at the Massachusetts General Hospital, referrals from local clinicians, or self-referral in response to advertisements. Probands were children and adolescents of both sexes who were six to 17 years old. To be included, subjects must have had a full lifetime DSM-IV diagnosis of BP-I disorder plus active symptoms of the disorder at the time of study entry. Subjects were excluded if they had either organic brain dysfunction or mental retardation (IQ < 70) or if their BP disorder was due solely to a medication reaction. All subjects’ parents or guardians signed written informed consent forms and children older than seven years of age signed written assent forms. All study procedures were reviewed and approved by the subcommittee for human subjects of our institution.
Diagnostic proceduresPsychiatric assessments of subjects (probands and first-degree family members) younger than 18 years were made with the Kiddie Schedule for Affective Disorders and Schizophrenia for School-Age Children, Epidemiologic Version (KSADS-E) (7). Assessments of those older than 18 years were made with the Structured Clinical Interview for DSM-IV (8) supplemented with modules from the KSADS-E to cover childhood disorders. At baseline, all subjects were ≤ 17 years old and were thus assessed with the K-SADS-E. At follow up, 53 subjects were ≤ 17 years old and were assess with the K-SADS-E and 15 subjects were > 17 years old and were assessed with the Structured Clinical Interview for DSM-IV supplemented by the K-SADS-E for childhood disorders.
This 5-year follow-up study includes 15 subjects younger than 12 years whose diagnoses were obtained by an interview with the parent about the child. In addition, 53 subjects were aged 12 years or older, and diagnostic data on these subjects were obtained from two sources: a direct interview of the parent about the child and a direct interview of the child about him/herself. We combined these interviews such that an endorsement of a diagnosis in the subject by either the parent or the child resulted in a positive diagnosis.
Extensively trained and supervised psycho-metricians with undergraduate degrees in psychology conducted all the interviews. At the baseline clinical assessment, raters were blind to the study assignment and whether the subject was a proband or sibling. Siblings were studied, but not reported on in this study, as the original study was a family study. Different raters, who were also blinded, performed the follow-up assessments. All diagnoses were reviewed by a sign-off committee of experienced board-certified child and adolescent psychiatrists or clinical psychologists who were blind to the subjects’ ascertainment group, ascertainment site, and data collected from other family members. Based on 500 interviews, the median kappa coefficient between raters and clinicians was 0.99 and the median agreement between individual clinicians and the clinical review committee chaired by the principal investigator (PI) was 0.87. Kappa coefficients for individual disorders have been reported elsewhere (4).
Children were determined to meet DSM-IV criteria for BP-I disorder according to assessments completed with the KSADS-E. The DSM-IV requires subjects to meet criterion A for a distinct period of extreme and persistently elevated, expansive, or irritable mood lasting at least one week, plus criterion B, manifested by three (four if the mood is irritable only) of seven symptoms during the period of mood disturbance. To ensure that the criterion B symptoms were concurrent with the criterion A mood disturbance, subjects were directed to focus on the worst or most impairing episode of mood disturbance while being assessed for the presence of the confirmatory criterion B symptoms. That is, the subject was asked to consider the time during which the criterion A mood disturbance was at its worst for the purposes of determining whether the remaining criterion B symptoms were also evident at the same time as the mood disturbance. The onset of first episode, the number of episodes, the offset of the last episode, and the total duration of the illness were also recorded. Any subject meeting criteria for BP-II or BP disorder not otherwise specified (BP-NOS) was not included in this study. To gauge a distinct episode, our interviewers asked for “a distinct period (of at least one week) of extreme and persistently elevated, expansive, or irritable mood” and further required that the irritability endorsed in this module was “super” and “extreme.”
To meet for a subthreshold diagnosis of mania, a child must have met criterion A for a period of four days or longer, and/or have at least two (three if the mood is irritable only) of the seven criterion B symptoms and associated impairment. One-year prevalence of a disorder was defined as positive if the subject met criteria for a given disorder in the year before the time of the 5-year follow up. To meet for a subthreshold diagnosis of depression, a child must have met criterion A for a period of one week or longer, and/or have at least three of the criterion B symptoms and associated impairment.
We also examined levels of impairment. For the KSADS-E, once a diagnosis was established as full or subthreshold, the rater assigned a severity designation (mild, moderate, or severe), for both past and current diagnoses, based on the clinical material presented. All severity designations were reviewed by the same sign-off committee of experienced board-certified child and adolescent psychiatrists or clinical psychologists who reviewed the diagnoses.
Other subject characteristicsSocioeconomic status (SES) was measured using the 5-point Hollingshead scale (9). We used the DSM-IV Global Assessment of Functioning (GAF) to measure overall level of functioning within the last month (current functioning) (7). Questions regarding academic functioning (tutoring, repeated grades, and placement in special class) were also asked during the interview.
Group assignmentPersistence of subjects returning for the 5-year follow up was described as syndromatic persistence (full BP-I disorder criteria met in the past year) or symptomatic persistence (subthreshold BP-I disorder or full or subthreshold major depression in the past year). Remission of subjects was described as syndromatic and symptomatic remission, or in other words, euthymic. Remission was defined as without full or subthreshold diagnoses of major depression or mania in the previous year. One-year prevalence was defined as positive if the subject met the criteria for a given disorder in the year before the time of the 5-year follow up.
Statistical analysisWe first compared demographics between those lost to follow up and those who returned for follow up using Student’s t-tests for continuous measures, Pearson’s chi-square or Fisher’s exact tests (if expected counts were < 5) for dichotomous measures, and Wilcoxon rank-sum tests for ordinal measures. Next, we compared demographic characteristics among subjects with syndromatic persistence, symptomatic persistence, and syndromatic or symptomatic remission using logistic regression for binary outcomes, exact logistic regression for binary outcomes with zero-cells, linear regression for continuous outcomes, and ordered logistic regression for ordinal outcomes. We then examined specific characteristics of BP disorder. For baseline and lifetime duration and number of episodes, the variances were higher than the means within each group, indicating that over-dispersion was present in the data. Therefore, we analyzed baseline and lifetime duration and number of episodes using negative binomial regression, that is, Poisson regression with an extra parameter to test for over-dispersion. We analyzed the number of symptoms and severe impairment at baseline using linear and logistic regression, respectively.
We compared subjects’ overall level of functioning within the past month using linear regression and school functioning outcomes using logistic regression. Additionally, we analyzed the 1-year prevalence of comorbid psychiatric disorders and family history of psychiatric disorders using logistic regression or, in the event of zero-cells or expected counts less than five, exact logistic regression. We used logistic regression with robust standard errors to account for the non-independence of family members to compare rates of mood disorders in first-degree relatives of probands. All analyses were two tailed and performed at the 0.05 alpha level using Stata® (Version 14).
Results Subject characteristics and retention/attritionOf the 78 subjects at the 4-year follow up, 68 (87%) returned for the 5-year follow up. There were no differences in baseline age (9.7 ± 3.5 vs. 10.6 ± 3.3 years; t103 = −1.27; = 0.21), sex (75% male vs. 86% male; χ2 = 1.91; p = 0.17), or functional impairment (GAF score: 40.2 ± 6.1 vs. 39.1 ± 5.9; t103 = 0.90; p = 0.37) between those who returned for the 5-year follow up (N = 68) and those were lost to follow up at any point since baseline (N = 37). There were statistically significant differences in SES (1.6 ± 0.8 vs. 2.2 ± 1.1; z = −2.99; p = 0.003) and age at onset of BP-I disorder (4.6 ± 3.3 vs. 6.8 ± 3.7 years; z = −3.16; p = 0.002) between the two groups. Those who returned for follow up came from a higher SES bracket and had an earlier age at onset.
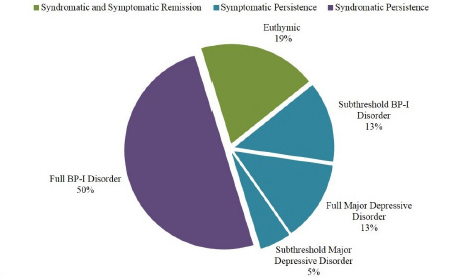
At follow up, returning subjects were 14.9 ± 3.8 years old and had an average age at BP onset of 4.6 ± 3.3 years. The median duration of BP disorder at follow up was 10 years (interquartile range: 7 to 14), and 54% of subjects had reported ultra-rapid or ultradian cycling during their lifetime. As shown in Figure 1, 19% (N = 13) of the returning subjects with BP-I disorder at baseline were euthymic (i.e., syndromatic and symptomatic remission) during the last year. The other 81% (N = 55) of subjects fell into three categories: those who continued to meet full diagnostic criteria for BP-I disorder (N = 34, 50%) (i.e., syndromatic persistence), those who continued to have persistent subthreshold BP-I disorder (n = 9, 13%), and those who had full (N = 9, 13%) or subthreshold (N = 3, 5%) major depression (i.e., symptomatic persistence).
Figure 1.Persistence of DSM-IV BP-I in youth at the 5-year follow-up.

Of the euthymic subjects, none were receiving treatment. Of the 57 subjects who had met with full BP-I at the 4-year follow up, six were lost to follow up, nine remitted, 11 had subthreshold BP-I or full or subthreshold major depressive disorder, and 31 maintained full BP-I at the 5-year follow up. Of the five subjects who were euthymic at the 4-year follow up without treatment, two were lost to follow up, one remained euthymic, one had full BP-I at 5-year follow up, and one had full major depressive disorder at follow up.
Demographic characteristicsThere were no significant differences in sex, ethnicity, age, or SES between those with syndromatic persistence, symptomatic persistence, and syndromatic and symptomatic remission (Table 1).
TABLE 1.Demographic characteristics of subjects with syndromatic and symptomatic remission, syndromatic persistence, and syndromatic persistence
 Characteristics of Bipolar-I Disorder
Characteristics of Bipolar-I DisorderThere were no significant differences in baseline duration of BP-I disorder across the three groups (syndromatic/symptomatic remission, symptomatic persistence, and syndromatic persistence), but there were significant differences in lifetime duration of BP-I disorder (Table 2). Those with syndromatic persistence had a significantly longer lifetime duration compared with the other two groups. There were no significant differences in the rate of subjects with baseline or lifetime ultra-rapid (≥ 20 episodes per year) or ultradian (≥ 300 episodes per year) cycling (see Table 2). The three groups significantly differed in both baseline and lifetime number of symptoms (see Table 2). Those with syndromatic persistence had significantly more baseline symptoms compared with those with full remission and more lifetime symptoms compared with the two other groups. Examining severe impairment at baseline, there were no significant differences among the three groups (see Table 2).
TABLE 2.Characteristics of bipolar disorder
 Psychiatric disorders at follow up
Psychiatric disorders at follow upAt follow up, there were significant differences in the 1-year prevalence of major depressive disorder (Exact, p < 0.001), attention-deficit/hyperactivity disorder (ADHD) (χ22 = 13.42, p = 0.001), oppositional defiant disorder (χ22 = 12.75, p = 0.002), and conduct disorder/antisocial personality disorder (χ22 = 9.76, p = 0.008) among the three groups (Figure 2). Subjects with symptomatic persistence had significantly higher 1-year prevalence of major depressive disorder, ADHD, and oppositional defiant disorder compared with those with syndromatic and symptomatic remission. Subjects with syndromatic persistence had significantly higher 1-year prevalence of all four psychiatric disorders compared with those with syndromatic and symptomatic remission. They also had a significantly higher 1-year prevalence of conduct disorder/antisocial personality disorder compared with those with symptomatic persistence.
Figure 2.One-year prevalences of comorbid psychiatric disorders.
a Compared to syndromatic and symptomatic remission. b Compared to symptomatic persistence. *P<0.05, **P<0.005, ***P<0.001
 Global and school functioning
Global and school functioningAt the 5-year follow up, there were significant differences in overall level of functioning within the past month, as measured by the GAF (F2, 65 = 25.85, p < 0.001), with subjects with syndromatic persistence having significantly more impaired scores than the other two groups and those with symptomatic persistence having significantly more impaired scores than those with syndromatic and symptomatic remission (Figure 3, A).
Figure 3.Current (last month) global functioning and one-year prevalence of school functioning.
a Compared to syndromatic and symptomatic remission.b Compared to symptomatic persistence. *P<0.05, **P<0.005. ***P<0.001

There were significant differences among the three groups in the 1-year prevalence of being placed in a special class (χ22 = 7.08, p = 0.03), but not in the 1-year prevalence of repeating a grade (Exact, p = 0.55) or receiving extra help (χ22 = 3.07, p = 0.22) (Figure 3, B). Those with syndromatic persistence had a significantly higher 1-year prevalence of being placed in a special class compared with the other two groups.
Family history of psychiatric disordersWe found no significant differences in family history of major depressive disorder (Exact, p = 0.81), BP-I disorder (χ22 = 1.14, p = 0.56), ADHD (χ22 = 1.14, p = 0.56), oppositional defiant disorder (χ22 = 5.92, p = 0.05), conduct disorder/antisocial personality disorder (χ22 = 0.21, p = 0.90), multiple anxiety disorders (χ22 = 2.13, p = 0.34), or substance dependence (χ22 = 0.98, p = 0.61) across the three groups (Figure 4, A).
Figure 4.Family history (FHx) of psychiatric disorders.

In addition to family history of psychiatric disorders, we also examined the rates of mood disorders in the first-degree relatives of our probands. There were no significant differences in the rates of major depressive disorder (χ22 = 0.20, p = 0.91), BP-I disorder (χ22 = 1.11, p = 0.58), or any mood disorder (χ22 = 0.35, p = 0.84) among first-degree relatives of probands with syndromatic and symptomatic remission, first-degree relatives of probands with symptomatic persistence, and first-degree relatives of probands with syndromatic persistence (Figure 4, B).
DiscussionAlthough there were more similarities than differences from the 4-year follow up to the 5-year follow up, some differences are of note. Our groupings from the 4-year follow up differed in two ways. In the 5-year follow up, we do not have treatment data to indicate how many youth of the euthymic group were receiving treatment for their disorder. Thus, the euthymic group in the 5-year follow up includes treated and untreated individuals. In addition, in the 4-year follow up, we report on the persistence of major depression, but in the 5-year follow up, we report on the persistence of depression by indicating rates of both full and subthreshold depression. As reported by Vaudreuil et al. (10), subthreshold states of pediatric BP disorder are highly morbid in themselves and, if present, should not be considered remission. Few longitudinal studies of pediatric BP consider the persistence of full and subsyndromal mania as well as full and subsyndromal depression. Thus, we have reported on persistence including both subsyndromal mania and depression.
In the 4-year longitudinal study, 73.1% of subjects continued to meet for full BP-I disorder at the time of the follow-up assessment. In the 5-year study, that group represents 50% of the sample. In contrast, in the first follow-up group, 5.1% had depression without mania, whereas at the 5-year follow up, 18% had depression without mania. In addition, the subthreshold mania group grew from 6.4% to 13%. Taken together, this suggests a waxing waning course between full and subthreshold mania as well as between mania and depression. In both follow ups, a minority of the group was euthymic, 15.4% at the 4-year follow up, and 19% at the 5-year follow up.
The remitted patients in this 5-year follow up are older than the other groups, but the age ranges are similar, and this difference in mean does not reach statistical significance (mean age, 16.9 vs. 14.5 and 14.4). However, if this trend were to continue, it could indicate that age brings an improving course for a subset of patients. Evaluating predictors of improvement and linking an improving trajectory to treatment would be useful for future study.
Ultimately, this 5-year longitudinal follow-up study extended our previous 4-year follow-up findings (4) which documented the persistence of pediatric BP-I disorder. Our original follow-up study’s findings indicated that the overwhelming majority of youth with BP-I disorder at baseline continued to meet full DSM-IV diagnostic criteria for BP-I disorder at follow up (i.e., syndromatic persistence) or either subthreshold (13%) BP-I disorder or full or subthreshold (18%) major depression. The current study’s results further document the high persistence of BP-I spectrum symptomatology in BP-I youth, including subsyndromal manifestations of mania and major depressive disorder. These results provide compelling evidence of the morbidity and dysfunction associated with pediatric BP-I disorder supporting efforts for early identification and treatment of this disabling disorder.
The high level of persistence documented in our sample of youth with BP-I disorder are consistent with findings reported in the pioneering work by Geller et al. (11) who followed-up children with pediatric onset BP disorder at 6, 12, and 18 months, and 2, 3, 4, 5, 6, and 8 years to assess the stability of the BP diagnosis in 115 children diagnosed in the prepubertal years (average age of diagnosis, 7.3±3.5 years). The 2-year follow-up re-ascertained 89 subjects and the 4-year follow up 86, and both of these studies reported high rates of persistence including assessment of both full and subthreshold states of both mania and depression. These authors concluded that their findings validated “the existence, long-episode duration, and chronicity of child mania.” (11). These reports support the importance of assessing subthreshold states of mania and depression at follow up.
At the 8-year follow up by Geller et al., 54 subjects were aged 18 years or older, and 44.4% of that group met full criteria for an episode of mania after the age of 18 years at the follow-up interview. Recovery in this study was defined as eight consecutive weeks without meeting full DSM-IV criteria for mania, and remission was defined as two to seven weeks without meeting full DSM-IV criteria for mania. This study did not address subthreshold states of mania or the presence of full or subthreshold depression. Although 44.4% strongly supported continuity of pediatric BP disorder onto the adult years, subjects who had subthreshold symptoms of mania or full or subthreshold depression were not included in this outcome measure. This study provides important validation that pediatric onset BP disorder persists onto the adult years.
Our findings are also consistent with those of Birmaher et al. (3) and the Course and Outcome of Bipolar Youth longitudinal study. In their 2-year follow-up study of 152 children and adolescents with BP disorder, these authors reported that 50% of their subjects had at least one syndromal recurrence and had syndromal or subsyndromal symptoms during 60% of the follow-up time. The authors included BP spectrum diagnoses and defined BP-NOS as the presence of an abnormal mood state with change in functioning for at least four hours within one 24-hour period for four different days lifetime, that was either elated (plus two associated symptoms of mania) or irritable (plus three associated symptoms of mania). In this study, 45% of subjects with BP-NOS switched to BP- or BP-II with the median time to conversion of 58 weeks (12). This study highlights the importance of assessing and following subthreshold symptoms of BP disorder in youth.
The Longitudinal Assessment of Mania Symptoms (LAMS) study (13) followed 703 children aged seven to 12 years with manic symptoms based on a parent-completed questionnaire. The majority of this sample, 77%, did not meet the criteria for any BP disorder, even BP-NOS as defined by the Course and Outcome of Bipolar Youth study. In this study, 15% of the children with manic symptoms showed high and rising or unstable symptoms of mania over time, suggesting a worsening course. This study provides useful information about children with manic symptoms who do not meet criteria for a BP disorder diagnosis at baseline, and the findings suggest that a subset of children with manic symptoms, but no diagnosis, may be at risk for a worsening course.
Highly consistent with our previously reported findings (4), in our 4-year follow-up study, persistent and non-persistent cases at the 5-year follow-up mark had similarly high levels of psychiatric comorbidity, familiality of mood disorders, and school dysfunction rates. These poor functional outcomes are consistent with the studies of pediatric onset BP (14) and suggest the importance of including functional correlates in follow-up studies in addition to symptoms of mania and depression.
Our findings of high levels of subthreshold persistence are noteworthy. Many studies of pediatric and adult BP disorder document the familiality, morbidity, and disability associated with subthreshold forms of BP-I disorder. We recently documented similar familial underpinnings for subsyndromal and full pediatric BP disorder (15). Using data from a community sample, Lewinsohn et al. (16) reported that youth with subthreshold BP-I disorder had impairment, comorbidity, and suicide attempts that were as severe as those with a full BP diagnosis. Adult studies have similar findings. For example, the National Comorbidity Survey of more than 9000 adults (17) reported that subthreshold BP disorder in adults is associated with high morbidity and disability. More clinical and scientific attention is needed to further characterize and intervene in subthreshold BP-I disorder.
LimitationsOur findings should be considered in the context of methodological limitations. Although we did not administer structured diagnostic interviews directly to children younger than 12 years of age, a clinical diagnosis of BP-I in the index children was corroborated by clinical assessment by an expert clinician before study inclusion (18). In addition, as the mean age at follow up was 15 years, most subjects underwent direct structured interview at follow up; however, 15 subjects were still younger than 12 years, and in those cases, diagnoses were obtained from maternal interview only, whereas for older subjects, we established diagnoses by combining parent and child reports. To support this practice, in the past, we have examined the concordance between mother and child reports for the diagnosis of pediatric BP disorder. In a 2009 report (19), of 98 pairs from two family studies of pediatric BP disorder, only four had a positive youth report combined with a negative maternal report. Of the 98, the majority, 59 pairs, were concordant (both mother and child reported the diagnosis) and 35 were discordant (the mother endorsed BP disorder, but the child did not). An analysis of the 35 concordant and discordant groups found no differences in onset, duration, or impairment of mania; rates of psychiatric hospitalization; cognitive variables; or rates of disorders in family members. We concluded that maternal reports, which were more common than youth-alone reports, are informative in the diagnosis of pediatric BP disorder, lending support to their use in our younger than 12 years group of subjects. Thus, for the current 5-year follow up, data were combined such that endorsement of a diagnosis by either the parent or the child resulted in a positive diagnosis.
Although some of the sample was lost to follow up after 5 years, few differences (age of onset of BP disorder and SES) between those lost to follow up and those included in the study were found. Because this sample was clinically referred and primarily white, these results may not generalize to non-referred children or to families of other ethnic groups. Our definition of persistence and remission by the presence of full or subthreshold syndromes of mania or depression occurring in the past year at the time of follow up differed from those used by other investigators (3, 5-6) who defined remission as an 8-week period of loss of full syndrome. Although the establishment of the best definition of remission and persistence for pediatric BP-I disorder awaits additional research, we consider our definition to be a strength as it captures a clinically meaningful time period and symptom picture.
Clinical significanceDespite these considerations, this 1-year extension of a previously reported longitudinal 4-year follow-up study onto mid adolescence confirms the high level of persistence of pediatric BP-I disorder. In addition to the high levels of persistence of the full syndromatic persistence of BP-I disorder, we confirmed previous findings showing high levels of persistence of subthreshold BP-I disorder as well as full and subthreshold states of depression. These results contribute to a growing scientific literature documenting the high morbidity and persistence of pediatric BP-I disorder from childhood onto late adolescence and young adulthood. Our findings emphasize the critical need for early identification and appropriate interventions for children with BP-I and associated disorders.
Post et al. (20) demonstrated that more adverse outcomes among adults with BP disorder is associated with early-onset as well as delayed treatment. Early identification of both full and subsyndromal presentations of the disorder, as well as early intervention, is imperative for improved outcomes. The importance of subsyndromal states is increasingly recognized, which will facilitate early identification and can lead to earlier treatment. There are currently many United States Food and Drug Administration (US FDA)-approved medications for the treatment of pediatric BP disorder. These approved medications include, for manic or mixed states in youth ages 13 to 17 years, lithium and olanzapine. For manic or mixed states in youth ages 10 to 17 years, US FDA-approved medications include risperidone, aripiprazole, and asenapine. Quetiapine is FDA-approved as monotherapy or as adjunct to lithium or divalproex sodium, for manic states, in youth age 10 to 17 years, and lurasidone is approved for BP depression in youth age 10 to 17 years (21). However, clinicians may be reluctant to extend these treatments to younger patients.
In addition, the second-generation antipsychotic medications are fraught with adverse effects such as weight gain—which can affect adherence and increased risk for cardiovascular disease and metabolic disorders (22-24). Other FDA-approved treatments for BP include mood stabilizers such as lithium. However, these medications have shown only moderate effectiveness in children and adolescents and is fraught with both serious and annoying adverse effects which limit its use, such as acne, weight gain, and need for regular blood test monitoring (25, 26). Studies examining the ameliorating effects of complementary and alternative supplements provide promising results and may prove especially useful in cases of mild to moderate illness as well as for very young children, in whom clinicians may wish to avoid exposure to medications which have known and unknown adverse effects. According to our pilot and interim analyses (27, 28), the use of natural supplements such as omega-3 fatty acids, inositol, and N-acetylcysteine produces positive improvements in the reduction of both manic and depressive symptoms in children and adolescents. If confirmed, these natural treatments could provide clinicians with a safe alternative for some cases of early onset of BP disorder, thus mitigating persistence and morbidity.
Future DirectionsConsidering the significant amount of longitudinal data we have collected through the past 5 years of follow up, we plan to examine whether critical measures from baseline predict the number of symptoms presented by a patient, or the group assignment of a patient, at follow up. Such measures could include specific diagnoses, severity in symptoms, cognitive measures, GAF, school attainment, SES, or age.
留言 (0)