
記住我

There is a long tradition in follow-up studies on adults with autism spectrum disorder (hereafter, autism) of using the concept of “overall outcome” to summarize how they are faring. Outcome ratings are generally based on independence and social competence regarding employment, friendship, and living arrangements and are categorized accordingly as ranging from “very poor” to “very good” (1, 2). Reviews of follow-up studies of adults with autism show that overall outcome was variable, where the diversity of the samples is an important contributing factor. However, only around 20% of participants fulfilled the criteria for “very good/good” outcome, and around 50% had “very poor/poor” outcome (3, 4).
Many long-term studies have also evaluated outcomes in specific areas, such as autism diagnosis, IQ, adaptive behavior and co-occurring disorders. A systematic review of follow-up studies in adulthood showed that the diagnostic status of autism remained stable, although most studies reported some overall improvements in autism symptoms. There was great individual variability in terms of stability and/or change in IQ over time, but the general trend was stability or some decrease. Although variability was also observed in adaptive behavior scores, they were relatively low over time, with some improvements (5).
Co-occurring disorders can affect the outcome of individuals with autism, influencing well-being, behavior and development. They can be a further cause of impairment and reflect additional disability (6, 7), but at least three of every four individuals with autism meet diagnostic criteria for another disorder (6, 8).
Quality of life has received increased attention as an important part of outcome measures, including assessments of both objective and subjective perceptions (by the individual and by persons close to the individual) of his or her well-being, and also how well the environment meets the individual’s needs (1). A recent meta-analysis (9) showed that adults with autism had significantly lower quality of life than adults without autism. However, studies on quality of life in adults with autism have reported more positive results, compared with those based on the objective overall outcome measures (10, 11). Thus, to get a more complete picture of overall outcome, both objective and subjective criteria need to be taken into account.
Over the years, studies have indicated some improvements in outcome for people with autism. The reasons may be diverse, for example, young people with autism may have more opportunities now than before and, in most instances, they have received earlier diagnosis and specialized intervention. Furthermore, more individuals with good intellectual ability are nowadays diagnosed with autism (2, 5, 8, 12).
Lovaas’ pioneer study (13) on early intensive behavioral intervention (EIBI) showed outstanding results, where intellectual ability and academic performance improved significantly. EIBI has repeatedly demonstrated success for children with autism, where they have outperformed children in control groups in cognitive functioning, language, and adaptive behavior (14-16). However, information on long-term effects into adolescence is limited, but promising (17).
The aim of this pilot study was to examine the long-term outcome of children with autism who received different forms of early intervention during their preschool years, enquiring two research questions: 1) How do these individuals with autism fare in early adulthood? 2) To what extent do the different gains achieved during preschool years by different interventions persist into adult life?
Method ParticipantsIn the years between 1995 and 2000, a small group of children participated in the Iceland Young Autism Project (IYAP) and received intervention based on the UCLA model for EIBI (Supplement 1). Inclusion criteria were (i) a diagnosis of childhood autism according to ICD-10/F84.0 (18); (ii) chronological age between 24 and 42 months at intake; (iii) a ratio IQ/DQ score above 35 on the Bayley Scales of Infant Development-Second Edition (19); and (iv) residence in one of the three local communities in the capital area that had agreed to implement the program within their preschools. Exclusion criteria were (i) a presence of severe medical conditions that would prevent full participation in the treatment and (ii) parents not able or willing to adhere to their part in the treatment protocol (see Supplement 1).
Autism diagnosis took place at the State Diagnostic and Counselling Centre (SDCC) and was based on interdisciplinary evaluation. The procedures included the Autism Diagnostic Interview, Revised (ADI-R; 20), direct observation of behavior with the Childhood Autism Rating Scale (CARS; 21), developmental tests, neurological evaluation, and clinical observations from team members (22).
Parents of newly diagnosed children, who met the inclusion criteria during the recruitment period (1995 to 1997) for the study, were informed about the IYAP and invited to enroll their child. As a result, six children received EIBI, and 14 eclectic treatment (ET; 23). The children in the ET group were diagnosed at the SDCC during the same time period as the EIBI group and met all the inclusion criteria except for residence.
Participants were followed from intake (time 1) to the age of six years (time 2). The groups were comparable on age and all standardized measures at time 1. Reassessment at time 2 showed that the EIBI group had made significant gains in IQ, and that autism symptoms had decreased significantly, whereas such changes were not found for the ET group. Although statistical differences were not detected between the groups at time 2, effect sizes were large on all variables (Supplement 2). The participants are now in their early twenties (time 3), and the present study gathered data on them at this point in time. Of the original 20 individuals and their parents, 15 agreed to participate, five from the EIBI group and 10 from the ET group. The average age of the participants was 21.9 years (range, 19 to 24 years), and the group comprised 13 male and two female participants.
Measures Symptoms of autismThe Social Communication Questionnaire (SCQ; 24) is a screening instrument that was used to evaluate present symptoms of autism. The SCQ was developed on the basis of the ADI-R and consists of 40 items to which parents or caregivers answer yes or no. Cut-off score of 15 was used, as has been recommended. SCQ is available in lifetime and current behavior versions, and the latter was used in this study.
Attention-deficit hyperactivity disorderThe Attention-deficit Hyperactivity Disorder-Rating Scale (ADHD-RS; 25) screens for symptoms of hyperactivity/impulsiveness and attention deficits. The items are based on the DSM-IV diagnostic criteria of ADHD. Four versions of the questionnaire exist: self-report of symptoms in childhood, self-report of current symptoms in adulthood, informant report of symptoms in childhood and informant report of current symptoms in adulthood. The latter two, or the informant-based versions, were employed in the present study. Items are scored on four parts: hyperactivity/impulsiveness in childhood and at present, and attention deficits in childhood and at present. Scores are then converted into standard scores with the average of 50 and a standard deviation of 10; the cut-off score of 65 is recommended (25, 26).
Adaptive behaviorThe Vineland Adaptive Behavior Scales, Second Edition (VABS-II; 27), a semi-structured interview administered to a parent or caregiver, was used to assess current adaptive behavior. For the age groups involved, the VABS measures three domains of adaptive behavior: communication, daily living skills, and socialization. Items are scored on a scale from 0 to 2, and these are converted into standard scores with the average of 100 and a standard deviation of 15.
Quality of lifeThe Quality of Life Scale (QOLS; 28) was used to assess the participants’ quality of life. The scale is intended to measure general satisfaction with life and contains 16 items that assess the following: material and physical well-being; relationships with other people; social, community and civic activities; personal development and fulfilment; and recreation. Scores range from 16 to 112, where larger values indicate better quality of life.
Functioning and participationThe WHO Disability Assessment Schedule 2.0 (WHODAS 2.0; 29) is a questionnaire that assesses daily functioning and participation of individuals with disability in six areas: understanding and communication skills, activity in life, participation in society, how an individual takes care of himself/herself, how the individual gets around, and how he or she gets along with other people. Scores range from 0 to 100; the higher the score, the higher level of disability and the lower the level of functioning and participation.
Status and overall outcomeAn interview with parents was designed for the purpose of the study to obtain information about the status and overall outcome of the participants. The interview consists of 17 open-ended questions regarding present residence, occupation/education, services, friendship, hobbies, well-being/mental disorders, and medication. This information was used to rate overall outcome in social functioning and independence as proposed by Howlin et al. (2), where the sum of scores from three domains, that is, employment, friendship, and independent living, are combined into outcome categories (“very good,” “good,” “fair,” “poor,” and “very poor”).
ProcedureAn invitation to participate, with an introduction letter, was sent to the participants and their parents. When informed consent had been given, a date was set for an interview, which took place either at the SDCC, at the participant’s home, or over the phone. Interviews with participants residing outside the capital area took place over the phone, and the questionnaires were sent to their homes. The researcher started with the open interview, and then moved on to the semi-structured interview (VABS-II), and finally asked the participants and/or parents to fill out the questionnaires, that is, QOLS, ADHD-RS, WHODAS 2.0, and SCQ. The participants were asked to fill out two of the questionnaires, the QOLS and the WHODAS 2.0. Nine participants did not have the ability to answer for themselves, and in those cases, the assessment was solely based on information from parents.
Permissions from the Scientific Committee at the SDCC and the National Bioethics Committee of Iceland (VSMb2015090020/03.01) were granted for this study.
Data analysisData were analyzed for the whole group and comparisons were also made between the original EIBI and ET groups. Statistical analysis was performed using SPSS-20. Descriptive statistics were explored, and correlations between variables were computed. Because of the small sample size, statistical significance was is reported. The findings should be treated as preliminary and need to be tested further in future studies.
Results Present symptoms of autism and co-occurring disordersFourteen parents answered the SCQ, with the mean score of 15.79 (standard deviation = 5.56, range: 7 to 26). Nine participants had considerable symptoms of autism and scored above the cutoff score (15 points) on the SCQ. Of the 15 participants, seven had received a co-occurring diagnosis: five with different kinds of anxiety disorders, and of these, two with major depressive disorder. The remaining two participants were diagnosed with ADHD. Some of the others were suspected of having a co-occurring disorder, but without formal diagnosis. Parents of five participants suspected that their child had ADHD, parents of four suspected anxiety disorder and parents of two suspected obsessive-compulsive disorder. The majority (73%) of parents were concerned about the participants’ mental health, most commonly anxiety and depression.
On the ADHD Rating Scale, four participants screened positive for attention-deficit disorder, and three for hyperactivity/impulsivity (T-score over 65). Regarding symptoms in childhood, eight participants screened positive for attention-deficit disorder and three for hyperactivity/impulsivity disorder.
Of the 15 participants, nine were on psychotropic medication, most commonly targeting anxiety.
Adaptive behavior, quality of life, functioning, and participationThe VABS-II interview was administered to parents of all 15 participants. The mean of the adaptive behavior composite score was 58.53 (standard deviation = 26.16, range: 20 to 108). The mean score on the Communication domain was 56.13 (standard deviation = 26.47, range: 21 to 104), the Socialization domain 63.40 (standard deviation = 27.62, range: 20 to 103), and the Daily Living Skills domain 63.33 (standard deviation = 24.90, range: 25 to 112).
Parents of 13 participants answered the QOLS, with a mean score of 78.38 (standard deviation = 13.65, range: 57 to 110), and parents of 14 participants answered the WHODAS 2.0, with a mean score of 32.44 (standard deviation = 19.46, range: 7.64 to 68.06). Six of the participants were able to report on their own quality of life as well as functioning and participation. Their mean score on the QOLS was 83.00 (standard deviation = 19.55, range: 54 to 112), and on the WHODAS 2.0, 23.62 (standard deviation = 16.41, range: 3.47 to 42.92). The mean score of those 6 and the corresponding parents on the QOLS was nearly identical, that is, 83.00 and 81.30, respectively.
The mean scores of participants and their parents on the WHODAS 2.0 were 23.62 and 20.02, respectively.
Status and overall outcome: interview with parents ServiceIn childhood, the majority (n = 14) of participants had personal support, travel assistance, and special education, and their families received respite care. Seven of the participants were not receiving any service when the interview took place, four of them because the parents claimed they did not need any. The majority (n = 14) of the parents were pleased and grateful for the service their children had received. However, they were displeased with the fact that much of the service terminated after graduation from secondary school at 16 years of age. Many of them said that their child needed more activity, especially social and leisure activities, and challenging enough employment. Lastly, some of the parents and the participants mentioned that there was not enough information available regarding what services they were eligible for, a lack of appropriate residential arrangements, and insufficient support for individuals living alone.
Residence, education, and occupationOf the 15 participants, seven lived with their parents, four in a home for people with disabilities, and four resided independently. A great majority of both participants and parents were satisfied with the current living arrangements. Thirteen participants had graduated from high school and one had received a university diploma, but the majority received substantial support. Six of the participants spent a part of the day at a rehabilitation center where they received individualized training, most often without salaries. Four participants were employed with support, one had a full-time job, and the remaining four were unemployed.
Leisure activities, interests, and friendshipAll the participants had few but intense interests and could spend a lot of their time fulfilling those interests. Movies, cinema, music, sports, cooking, and computers were dominating interests. Eight of the participants had no friends other than family members, and the remaining seven said they had at least one friend they spent some time with. One should bear in mind that some of the participants were not interested in having friends.
Overall social outcomeFive participants were rated as having a “good” outcome, that is, they had friends and acquaintances, worked with or without support, and lived independently, albeit they required a minor degree of support in daily living. Five participants were rated as having a “fair” outcome, that is, worked with support, were mostly living with their parents, needed some degree of support, and had some or no friends. The remaining five participants were rated as having a “poor” outcome, that is, they lived with their parents or in a home for people with disabilities, required considerable or almost complete support in daily living, and had no friends.
Comparison between groups in adulthoodTable 1 shows the mean scores, standard deviations, and ranges for the original EIBI and ET groups at time 3, on the SCQ, the ADHD-RS, the VABS-II, the QOLS, the WHODAS 2.0, and overall social outcome. The differences between the groups were negligible on all measures, but there were considerable variations in scores between individuals on all of them.
TABLE 1.Descriptive statistics for the early intensive behavioural intervention (EIBI) group and the eclectic treatment (ET) group on standardized measures at time 3

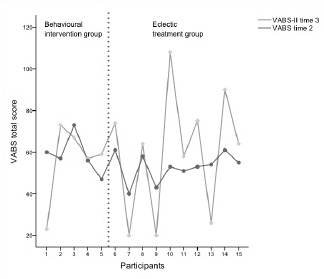
Figure 1 describes the participants’ total scores on adaptive behavior at time 2 (VABS) and 3 (VABS-II), which also show great individual variation, and show 10 participants having higher scores now (time 3) than when they were six years old.
FIGURE 1.Individual comparison on VABS at time 2 and VABS-II at time 3. VABS indicates Vineland Adaptive Behavior Scales.
 Relationship between childhood measures and adult outcomes Childhood cognitive ability
Relationship between childhood measures and adult outcomes Childhood cognitive abilityThe correlation of IQ at time 2 and overall outcome at time 3 was high (rs = −0.76). Thus, three of the four individuals with IQ ≥ 70 at time 2, had “good” overall outcome at time 3, and one of them had “fair” outcome. Three of the four individuals who had IQ ≤ 50 at time 2 had a “poor” outcome at time 3, and one of them a “fair” outcome. IQ at time 2 was also related to VABS-II at time 3 (rs = 0.79).
Childhood autism symptom severityCARS scores at time 2 were correlated to both overall outcome at time 3, (rs = 0.56) and VABS-II at time 3 (rs = −0.54).
Other relationships between time 2 and time 3 variables were moderate or low.
DiscussionThe present study examined the outcome of young adults who were diagnosed with childhood autism at an early age and received different forms of early intervention during the preschool years. The results show a great individual variation in symptoms of autism and co-occurring disorders, and in the form of residence, occupation, friendship, adaptive behavior, and quality of life.
Generally, the long-term outcome of individuals with autism shows diagnostic stability over time, although autism symptoms may decrease (5). In some instances, in the present study, one can assume the same, where reported symptoms of autism had decreased. Six of the participants had lower total scores than the recommended cutoff on the SCQ, but individual differences were substantial.
Most of the parents were concerned about their child’s mental health, and co-occurring disorders were common. Nearly half of the participants had received co-occurring diagnoses, which is a lower rate of comorbidity than has commonly been found among adults with autism (8, 30). Anxiety disorders were most common, with five participants having received a diagnosis of anxiety disorder, and four suspected of having one. In one study, approximately half of the adults with autism had anxiety disorders (8), and in other studies, the range was from 22% to 39% (30). Half of the participants who screened above the cutoff score of symptoms for attention deficit in childhood screened above the cutoff on present symptoms. Regarding hyperactivity/ impulsivity, the same three participants screened above the cutoff in both childhood and adulthood. Previous studies have reported rates of ADHD in young adults with autism as high as 28% (30). For some individuals, co-occurring conditions were so pronounced that they caused considerable difficulty, affected independence, and some of the participants were unable to seek employment due to anxiety and/or depression. Co-occurring disorders can greatly influence outcome, and information about these disorders is important when it comes to services and interventions for young people with autism.
A high proportion of the participants in the present study were on psychotropic medication, which is consistent with other studies on adolescents and adults with autism (31, 32). Moreover, it has been shown that these individuals are likely to continue on medication over time, and the proportion of those who are on medication tends to increase with age (31). We did not collect information on what type of medication the participants were on, but such information may be useful to understand the use and the effectiveness of this medically prescribed treatment.
Adaptive behavior was generally poor among the participants in the present study, and individual variability great. The group mean was more than two standard deviations from general age norms, which suggests that the majority of the participants need support with daily activities. Other studies have also shown individual differences in adaptive behavior, and thus the degree of support needed with daily living. Moreover, they have shown that adaptive functioning among individuals with autism tends to improve with age (5, 33). This was true for 10 of the participants in the present study, although in most instances, the improvement was small. Adult adaptive functioning was reported better in daily living skills and socialization than communication, which differs from other studies where socialization appeared to be the poorest domain (5, 34).
Importantly, the participants reported better quality of life than Icelandic people receiving trans-diagnostic cognitive behavioral group therapy in primary care for depression and/or anxiety, but poorer than university students (35). Billstedt et al. (10) reported similar results, where the quality of life of adult individuals with autism was better than could be expected despite impairments and low level of independence.
The mean score on the WHODAS 2.0 was as high as or higher than almost 12% of the general population (29). In a recent large study (36), the WHODAS 2.0 was used to measure disability among a diverse group of people. The mean score for people with autism was very close to the mean score in our sample (32.44 vs. 33.10), that is, significantly higher than that of people without disability, similar to that of people with schizophrenia and mental retardation, and considerably lower than that of people with dementia and stroke.
Assessment by participants and their corresponding parents regarding quality of life (QOLS) and functioning and participation (WHODAS 2.0) was in most cases similar. This has not been the case in other studies, where parents rate the quality of life of their children lower than the children themselves do, whether or not based on proxy methods (9, 37).
The results show great individual differences regarding the participants’ status, with some of them living independently, having received good education and being employed, whereas others lived in a group home and needed constant support. About a quarter (26.7%) of the participants lived by themselves. This is a higher proportion compared with other studies based on similar autism populations, which have shown that a minority of adults with autism achieve independent living, or only up to 13% (2, 8, 10).
All the participants had attended mainstream schools where they received support and one had graduated from a university. Generally, there is a great variability in findings on school attendance among individuals with autism, where most of them have either been in special schools or provisions (8, 10), or in regular schools with support (2, 38). Only a few individuals, in comparable longitudinal studies, have attended or graduated from a university (2, 8, 10, 38).
Almost three-quarters (73.7%) of the participants had some kind of work, which was most often in a rehabilitation center. One had supported employment, and one had a full-time job. The employment level of adults with autism varies between studies. Some show results similar to ours (10, 38, 39), whereas others report higher (13.2%) employment participation without support, where the most able individuals were working independently or self-employed (2). Still higher (21.8%) employment rate was reported in a Japanese study, which at that time reflected prosperous economic conditions with high demand for labor (40). Reviews on adults with autism have shown that employment levels are generally disappointing, even for those who are high functioning (30, 41).
Developing friendship is a challenge for many individuals with autism. However, almost half (46.7%) of the participants had at least one friend. In other comparable studies, the rate is somewhat lower, or ranging from 12% to 33% (2, 8, 10), and in one study, friendships were rarely reported (38).
In terms of overall outcome, just over 30% of the participants in the present study were considered as having a “good” outcome, and just over 30% a “poor” outcome. This is a more favorable outcome than that reported in recent reviews (5, 30), where approximately half of the participants were considered to have a “poor/very poor” outcome, and even more favorable compared with the rate (61.9%) reported for samples containing only participants with childhood autism (4).
Both IQ and CARS scores at time 2 were related to overall outcome at time 3. Autism severity, IQ, and verbal functioning in childhood are among the strongest prognostic factors in autism. However, even among individuals with favorable measures in childhood, variations in adulthood have been observed (5, 30). Thus, the individual in our study with the highest IQ (> 100), and the lowest level of autism symptoms, was rated as having a “fair” outcome. In this case, co-occurring disorders, such as depression and anxiety, affected independence and well-being.
The small sample size means that comparisons between the groups should be interpreted with caution. Pre-intervention (time 1), IQ, and symptoms of autism were comparable between the groups, but at post-intervention period (time 2), the participants who had received EIBI showed, on average, more gains than those in the ET group (Supplement 2). Today (time 3), it looks as though the different effects of the early intervention methods have faded out over the years. It is hard to speculate why, as confounding variables are many and 15 years have passed between follow-up measures. The participants have received varied levels of service, different kinds of education, lived in different environments, and now work at different places. Comorbid disorders can play an important part in their outcome, and the question arises as to whether the EIBI group would have maintained their superior progress over the ET group if their specific intervention had been ongoing for a longer period of time.
This pilot study has some important limitations. The sample size was small and only two participants were female. An additional limitation concerns comparison of long-term effects. The instruments used in the first study could not be used in the present one because of lack of funds, with the exception of the VABS. In IYAP, autism symptoms were assessed with the ADI-R and the CARS, but in the present study, the SCQ was used. It would have been preferable to add a direct observation of behavior with a standardized autism spectrum disorder diagnostic instrument. In addition, IQ was not assessed in the present study (time 3), and therefore could not be compared with IQ at times 1 and 2. As a result, an important comparison between the groups could not be made. Finally, the investigator, who collected the data at time 3, was not blind to the group assignment.
However, the study has some strengths. First, the inclusion criteria were precise, where all participants received the same diagnostic procedures, and the same classification (ICD-10/F84.0). Second, outcome measures were comprehensive. Third, there was repeated follow-up of the same individuals.
This is one of the few studies investigating the long-term effect of EIBI. Longitudinal studies on adults who received EIBI and other interventions in childhood are necessary on a larger scale, and with a more rigorous methodology, before definite conclusions can be drawn regarding their long-term effectiveness.
留言 (0)