
記住我

The Family Therapy Team (FTT) is part of Child and Adolescent Mental Health Services (CAMHS) in the Capital Region of Denmark. It was established to help families continuing to suffer even after having received regular treatment from CAMHS, the school system and social services. Families are thus referred from other parts of CAMHS when standard treatments are not considered sufficient. The referred child usually suffers from one or more psychiatric diseases, often with unusual or aggravated symptoms. The majority of presenting families have more than one member who suffers from a psychiatric or somatic disease.
The narrative family therapy (NFT) offered is family therapy in a narrative psychiatric context, based on two hypotheses. Whenever a child is suffering from a psychiatric disease, all members of the family are affected, and thus the whole family needs help. When parents’ sense of personal agency is negatively affected by the child’s suffering, helping the parents achieve increased personal agency, especially mastery of their child’s psychiatric disease, is a necessary component of treatment.
Narrative therapy principles were first developed by Michael White and David Epston (1-8). Narrative therapy does not directly aim to reduce symptoms. Instead, it focuses on changing a person’s relationship with the problem and changing their narratives about themselves and their problem. The fundamental aim of narrative therapy is for a person to experience a greater general sense of agency both towards themselves and towards the problem. Narrative therapists ground their work in social constructivist and post-structural theory and consider how the power of stories shapes peoples’ identities and lives.
NFT builds on narrative therapy. The NFT practiced at the CAMHS clinic has a specific engagement with Madsen (9). CAMHS therapists work collaboratively alongside families with an overt expectation that families have the ability to deal with the psychiatric problems in their lives and can experience themselves as having personal agency and power. Our manual for NFT consists of three elements: The therapeutic sessions, network meetings (with the school and municipality), and written documents (most important therapeutic letters after each session and the treatment plan). The parents decide who participates in the different sessions (the parents alone, the parents, and the appointed patient, the whole family, the extended family, the siblings, the patient, friends of the patients). The treatment consists of three phases, a clarification, a working, and a termination phase. Every fifth session in the working phase is a ”taking stock”-session. Externalizing problems, resources, ideals, and hopes are the grammar of the therapeutic language, and the manual demands that the clinical work is based on the four principles: Respect, trust, curiosity, and hope. The therapists ask questions aiming to help the family members build knowledge and wisdom, based on their own hopes and dreams. The statements, the therapists consider most helpful for the family are written on a big paperboard during the session. A detailed description of NFT can be read in our manual1. The considerations of developing the Danish NFT manual have been described in detail elsewhere (10).
Narrative therapy is seldom the subject of quantitative research (11), perhaps because narrative therapy avoids using diagnostic classifications in order to privilege “the voice of those who consult with us … working with their truth and their version of reality” (12). For some, this makes it unsuitable for quantitative research methods. Some narrative therapists are even actively opposed to quantitative methods (13). This relative lack of quantitative evidence for NFT is problematic for practitioners of narrative therapy in public healthcare settings with demands for evidence-based practice. Without robust clinical evidence, NFT risks are marginalized (9,12,14) and will not become a potential treatment available for patients seeking help at CAMHS.
Several studies have sought to show the effectiveness of narrative therapy by conducting it alongside established improvement measurements, typically through quasi-experimental (non-randomized) studies. An NFT intervention aiming to reduce parent/child conflict with six families found five of six families showed improvement in parent/child conflict as rated by parents using a multiple baseline analysis (15). A study of 10 young people with autism, offering five one-hour sessions of individual narrative therapy over 10 weeks found significant improvement according to both psychological distress measured by the Kessler-10 Scale and according to the emotional symptoms of the Strength and Difficulties Questionnaire (16). A school intervention aiming to enhance pupils’ self-esteem used a mixed method approach with a single group repeated measures design. Using the Beck’s Youth Inventory (BYI) scale, it found significant improvement of self-concept between pre- and post-intervention (17). Vroman and Schweitzer (18) studied an adult population with major depressive disorder receiving manualized narrative therapy. They compared each person’s scores against normative results in the evaluation of clinical significance and utilized benchmarking and clinical significance as alternatives to a RCT design. The manual was principle based, and they developed a treatment integrity measure for evaluating adherence and competence. They found 74% of the clients achieving a reliable improvement, 61% achieved a population functional level, and a clinically significant improvement comparable to benchmark research outcomes. The 3-months follow-up showed maintenance of symptoms, but not interpersonal relatedness improvement.
Bargenquast and Schweitzer (19) examined the effectiveness of an innovative, manualized psychotherapy drawing on three principles, one of them narrative therapy. They found adult patients significantly improved on the general outcome of subjective recovery and treatment-specific outcomes of self-reflectivity. This was quantitatively assessed using a single-sample, pre- and post-therapy design and qualitatively assessed using a case-study methodology. A life story intervention for individuals with intellectual disabilities and psychiatric problems was described, and quantitative analyses showed a decrease in total psychiatric complaints from pre- to post-treatment, which was still significant at follow-up (20). Bohlmeijer undertook a quasi-experimental (non-randomized) study to measure effects on an adult population with depression receiving a narrative therapy intervention called “The story of your life” that showed significantly fewer depressive symptoms and higher mastery compared to a waiting list group (21). Similarly, Seo deployed a quasi-experimental design to explore the effectiveness of a “narrative therapy with an emotional approach” program for people with depression (22). This showed significant positive effects on depressive symptoms and cognitive-emotional outcomes through measurements using a self-awareness scale, the Nowotny Hope Scale, the Positive Affect and Negative Affect Scale, and the Center for Epidemiological Studies-Depression Scale.
We developed NFT and called it Collaborative Family Therapy in our manual to honor the hypothesis we learned from William Madsen, here formulated by us: When problems within a family is really complex, helping is a messy business. But a collaborative stance based on narrative theory shows us a way through the messy business and make it possible to offer help that helps.
Aims of the studyThe study aimed to do a quantifiable study of our original hypothesis, by evaluating whether NFT has any measurable and quantifiable effect on the patients’ experience of specific psychiatric symptoms, and parents’ sense of personal agency. We hypothesized that we would observe statistically significant changes in BYI and Parent Activation Measurement (PAM) scores from baseline to follow-up. Thus, the study analyzed how measurements change pre- and post-treatment with NFT.
Method RecruitmentParticipants included in this study were families receiving NFT in the FTT at the Capital Region of Denmark CAMHS, which follows the accreditation standards and regulations of Child and Adolescent Psychiatry in the Capital Region of Denmark. The families were referred because they had continued suffering, despite having received treatments as usual from CAMHS, the school system and social services. All families were referred from other parts of the same CAMHS. None had received any treatment addressing the effects of the psychiatric problems on the family as a whole. The aim was to provide this missing treatment that neither the traditional therapy specific towards the psychiatric disease, nor family therapy specific towards family dynamics address. Parents and children filled out psychometric measurements before and after treatment to evaluate the burden of symptoms. The number of treatment sessions differed from family to family, depending on their needs and wishes. In NFT, families decide the termination date in collaboration with the clinicians and a positive NFT outcome is considered to be when the family feels confident to go on without help from the FTT.
Participants and measurementsFamilies were given full anonymity and the review of data processing was undertaken according to the standard safety regulations of the Capital Region concerning the processing of personal information under the Privacy Act. The families were informed of the study at the initial telephone conversation. They were given written and oral information of the purpose of the project at the initial meeting where they consented to participating in the project when patients and parents also completed the pre-outcome psychometric measurements. Post-outcome psychometric measurements were undertaken just before the final session at the clinic. Children and adolescents aged 8 to 17 filled in the BYI, which measures the perceived burden of common symptoms such as anxiety, depression, anger, disruptive behavior, and self-concept. We chose BYI for the children because they were addressing symptoms across different diagnoses and the Inventory includes both negatively and positively formulated descriptions. Parents evaluated their personal agency in relationship to their child’s psychiatric disorder through the PAM, which measures the parent’s sense of personal activation towards their child’s psychiatric illness (23). We chose PAM as the measurement most closely resembling a positive description of self-agency, since we hoped for a positive effect on the parents’ sense of self-agency towards their child’s illness.
The Beck Youth InventoryBYI measures the perceived burden of common symptoms of anxiety, depression, anger, disruptive behavior, and self-concept (24). BYI is characterized by including acceptable psychometric properties and is based on published Danish norms (25, 26). It is a self-report measure that contains questions which are both positively and negatively framed and focus on both problem and non-problem related areas of the child’s life. The BYI consists of five inventories of 20 statements each regarding the thoughts, emotions, and behaviors within the five domains. The child is asked to rate how frequently the statement has been true within the past two weeks. The choice of BYI was based on a review of existing psychometric measures for use in Danish CAMHS in 2013.
The Parent Activation MeasurementPAM measures the parents’ sense of personal activation towards their child’s psychiatric illness (23). It builds on the 13-item PAM, which originally focused on measuring patient activation towards physical conditions as a broad construct. Green (27) developed the PAM-Mental Health (PAM-MH) by adapting the 13-item PAM to specifically assess mental health-related activation. Subsequently a parent activation score was developed by Pennarola (23). We found the PAM to be the most useful measurement available, and we have previously described the process of choosing and implementing these psychometric measurements (28). We translated the PAM assessment (23) into Danish and back-translated it by an independent translator to verify accuracy.
There is still limited research about parental activation on behalf of their children even though the PAM measure is licensed for commercial and research use by its developers. Since the psychometric properties for the PAM measurements have not been researched, there are no norms for PAM (Danish or otherwise), and the measurement is not as rigorous as those we chose for the children (29). The parents’ scores were converted to an activation score from 0 to 100, where any scores below 55.2 show lack of personal confidence and knowledge to take action, or lack of belief that they can take action.
Statistical analysisWe used a single sample, pre- and post-therapy design and descriptive statistics for baseline values, mean ± standard deviation (SD) for parameters that were normally distributed, and median (interquartile range [IQR]) for those that were not. BYI raw scores for each domain were converted into T-scores based on age and sex. A T-score of 55 or less = average score, 55 to 59 = mildly elevated, 60 to 69 = moderately elevated and ≥70 = extremely elevated depression. We compared distribution of patients across these categories before and after treatment. To evaluate differences from baseline to follow-up in PAM and BYI outcomes, as well as differences in distribution across categories, we used Wilcoxon Signed Rank Test for Related Samples, and the Cohen’s d-test.
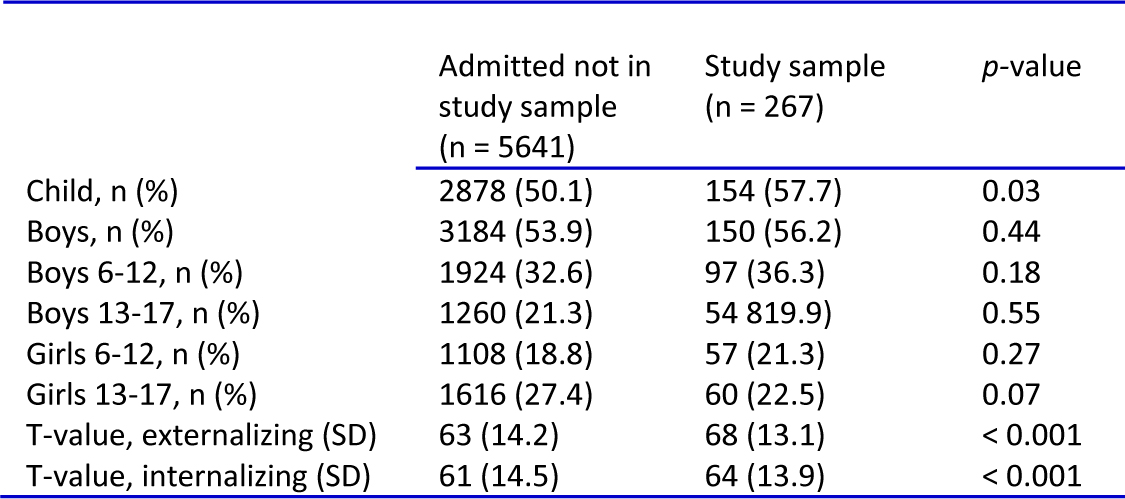
Results Descriptive dataOne hundred and five patients were enrolled during the study period, but complete data are only available for 48 patients. We have found no difference in age, gender, duration of treatment, number of sessions and psychiatric diagnosis between those who filled out questionnaires, and those who did not. We can only suppose that data incompleteness is because data were obtained during the initial NFT manual implementation and training period, which took longer than anticipated (28). Twenty-eight (58.3%) patients were girls and 20 (41.7%) were boys (p = 0.005). Median age at treatment initiation was 13.2 (IQR 11.2 to 14.9) years. Mean ± SD duration of treatment was 368.0 ± 224.4 days. Median number of sessions was 16 (IQR 11 to 29). We excluded three participants: one adolescent did not want family therapy and two adolescents stopped the therapy because they turned 18 and were referred to other treatment in adult psychiatry. We excluded these participants because we would have continued the treatment, if they had not turned 18 (Table 1).
TABLE 1.
There were no significant gender differences across diagnostic categories. Twenty-two patients (45.8%) received psychotropic medication, whereas seven (14.6%) patients were prescribed two or more medications in the intervention period. Forty-one of the patients had secondary diagnoses: seven had one secondary diagnosis, nine had two secondary diagnoses, eight had three secondary diagnoses, seven had four secondary diagnoses (for one patient two of these were somatic diagnoses), three had five secondary diagnoses, four had six secondary diagnoses (for one patient two of these were somatic diagnoses, for two patients one of these was a somatic diagnoses), two had eight secondary diagnoses (for these two patients one of these was a somatic diagnosis) and one patient had nine secondary diagnoses (for this patient two of these were somatic diagnoses).
Pre- and post-measurementsAll measurements showed improvement for both patients and parents, with the biggest statistical significance and highest effect sizes for the patients’ self-concept and the PAM. When the data were analyzed specifically for children who had a pathological score, the p-values increased (see Table 2).
TABLE 2.Change in symptom scores, median (IQR)

We have three main findings:
1. We found that psychiatric symptoms (anxiety, depression, anger, self-concept, and disruptive behavior) measured in pre-therapy BYI test showed improvement after the NFT intervention when tested in post-therapy BYI tests. The changes were statistically significant for self-concept (p = 0.002), and significant for depression (p = 0.030) and disruptive behavior (p = 0.030). The effect sizes were medium to large for self-concept, small to medium for the depression and disruptive behavior, and small for anxiety and anger.
2. Children who had pre-therapy scores demonstrating that they were suffering within the psychopathological range for one or several of the psychiatric symptoms changed more than the group as a whole. The change was highly statistically significant for self-concept (p = 0.001) and depression (p = 0.001), and statistically significant for anxiety (p = 0.011) and anger (p = 0.025). The effect sizes were basically the same as for the whole group. This suggests that NFT does have a specific and positive effect on psychiatric symptoms when they are perceived as pathologically burdensome.
3. The parents’ activation measurement changed from pre-therapy to post-therapy. The effect size was medium to large, indicating that NFT has a positive effect for the parents perceived sense of agency in relationship to the child’s psychiatric problems.
DiscussionThe purpose of the present study was to examine if it was possible to quantitatively evaluate the effects of NFT on the mental health status of patients admitted to our clinic, using standardized tools.
To the best of our knowledge this is the first study based on a specific manual for NFT for children and adolescents with psychiatric disorders. The manual was developed for a very diverse group of patients, with different diagnoses and a broad age group. In this respect, our manual differs from many others. It does not address specific problems or diagnoses but aims to give families a language for, and ways of placing themselves in, a more powerful position with regard to their different problems.
Our data show a statistically significant increase in BYI self-concept index (p = 0.002), with effect size in the medium to large range, as well as decreases in both depression index and disruptive behavior index (both: p = 0.030), with small to medium effect sizes.
In children with baseline BDI-indices in the pathological range, reflecting clinically significant symptoms (for instance, elevated BDI depression index in patient with symptoms of severe depression), NFT significantly improved these indices. This effect was seen for all indices except disruptive behavior index. Although the effect sizes were small in this restricted sample; our data support the hypothesis that NFT can alleviate clinically relevant symptoms regardless of underlying diagnosis.
Finally, we found a statistically significant increase in PAM. This is also in line with the principles of narrative therapy, in which treatment of the patient involves not only the patient but the entire family. A review of the parental factors influencing on mental problems in children (30) suggests that although parental factors only account for a small amount of variance in child outcomes, “there is increasing evidence that preventative parenting interventions […] have beneficial effects on children’s depression, anxiety, and internalizing problems.” Inviting the entire family into the therapy ensures that parental factors are also addressed. The observed increase in PAM reflects that parents had a higher perceived agency in relationship to the child’s psychiatric problems post-treatment.
While collected data are not normally revealed to patients in trial settings unless they specifically ask for it, it is possible that sharing and discussing this information with patients and their relatives could further aid their understanding of their problems and enhance improvement, while honoring the principle of transparency; an ideal which narrative therapy holds dear. How could we honor the principle of transparency of the treatment, if we ”hide” the scores? This principle might sometimes be juxtaposing and at other times be opposing to the principle of thickening the narratives of preferred stories and not thickening the problematic narratives. We believed, that sharing the BYI and PAM might be thickening the problematic narratives. Our clinicians gave special attention to this, that sharing the psychometric measurement scores may affect patients’ view of their symptomatology or severity, and this may in turn alter their outcomes. So we decided to adhere to the general principle of not showing the results of the measurements to the clinicians or the families unless they asked for it after the treatment. In hindsight, we believe that this might have been wrong. We could have used the results from the pre-measurements as another kind of question, asking if the child’s answers made sense to the parents, asking the child to explain how they answered, and so on. This might have helped the families and clinicians further understand the problems they were dealing with.
We want to share a story to underline this discussion for the readers to reflect on: Only a very few families were interested in seeing the results of their own measurements. But one family specifically asked for them, receiving the results after the last session. Their son had been referred because of an anxiety that tied him to his home. He was diagnosed with infantile autism, and the anxiety was explained as a result of insufficient attention to the autism from the school and the other contexts that the child was living in. This child had an almost normal pre-score for anxiety and a very high post-score for anxiety. Despite this, both he and the family agreed that they felt confident, that the anxiety no longer held him captive. The parents were at first astounded by this, as were we. We came to understand that the child’s autism had made it difficult for him to fully comprehend the questions concerning emotions before the therapy. But the therapy gave him a language for as well as ways of dealing with anxiety that enabled him to recognize, name and deal with anxiety from a powerful position. After therapy he was very aware of, and angry about, the tactics of anxiety and therefore rated them as very stressful in the questionnaire. These measurements are included in the statistics as this was an accidental finding. Nevertheless, this story adds to the calls for us to be transparent about measures and include the patients and families in all kinds of evaluations of our treatments.
We find that our approaches make the results applicable for people working within our field, and we hope this will generate more interest in exploring how to use NFT as a treatment for children and adolescents with psychiatric problems. Since many children have complex psychiatric symptomatology and their problems have profound negative effect on the whole family, we find it imperative that we work diligently to develop treatments that seek to help not only across the diagnostic specters, but also seek to help the entire family. We find that this study shows that this endeavor is indeed possible.
LimitationsThere are several limitations of the present study. First, due to its naturalistic design, the study did not have a placebo group or any randomization, so we cannot compare the outcomes to other treatment options. However, as our participants were referred to us only when treatment as usual (TAU) had failed to alleviate their symptoms, one could speculate that our outcomes were at least better than TAU. We would also have liked to do follow-up measurements.
Second, our treatment manual states that treatment should continue until the families themselves feel that it is no longer necessary, rather than for a pre-specified period of time. So, we did not explore the effect of NFT after a fixed dose of therapy. In a post-hoc analysis, duration of treatment was significantly associated with decrease in BAI (p = 0.042), but not with any other BYI indices.
Third, only 48 patients filled out the questionnaires, and complete datasets were available for 42 (87.5%) patients at baseline and 36 (75%) at follow-up. However, we were still able to find significant changes in BYI outcomes. We believe the low number was due to a team culture that was not strongly focused on research, since data completeness did increase over time and this culture has since been addressed (28).
StrengthsOur relatively large sample, validated instruments and manualized therapy add further strength to the interpretation of our results, and the diversity of our patient group suggests that our protocol is applicable to real-life settings. We believe the biggest strength of this study is that it was carried out in a normal clinical setting, where patients come with very different symptomatology and family-context. This is very similar to other Danish CAMHS-settings, and as such would be easily transferable. Some will argue that our inclusion of patients with every kind of psychiatric problem is a limitation, and that a more homogenous sample might be more desirable. We argue that the diversity of problems reflects the way patients are generally referred to CAMHS. Therefore, this study has implications for clinicians in settings who meet with patients who have complex problems.
In this respect, our manual differs to many other manuals. It does not address specific problems or diagnoses, aiming instead to give families a language and way of positioning themselves more powerfully in regard to their different problems. We consider that this approach is important, as many CAMHS work with children and adolescents who have complex symptomatology. We suggest that NFT might be an alternative choice of treatment for clinicians who find that treatment programs addressing “clear cut” problems have too narrow a focus.
Future researchDespite their limits, our results suggest that psychometric measurements can be used to evaluate the effect of NFT in clinical trials, making it possible to create an evidence base for the use of narrative therapy. The study adds to the growing number measuring the efficacy of narrative therapy. This research is still ongoing, and more studies are needed in this area to examine the qualitative and quantitative effects of narrative therapy.
This study indicates that NFT has direct positive effects on psychopathological symptoms which are measurable by psychometric measurements and therefore it is possible to conduct more rigorous quantitative research on narrative therapy, even though narrative therapy is not directly tailored towards symptom reduction. This suggests it is possible to create more evidence for NFT using quantitative psychometric measurements, thus making NFT available to families seeking help in mental health institutions.
Our study demonstrates how inspiring and important it is for clinicians to work in close collaboration with researchers, not only to produce evidence for NFT, but also to develop our treatments further. We hope this article will inspire more clinicians and researchers to collaborate, and that this might in turn make NFT available to an increasing proportion of children and adolescents with mental health problems.
SummaryThis study investigated measurable and quantifiable effects of NFT on patients’ experience of specific psychiatric symptoms and parents’ sense of personal agency. The results showed statistical significant changes with a good effect size for children with severe symptomatology, across different diagnoses and co-morbidity, as well as positive changes for the parent’s sense of activation towards their child’s disease, indicating that NFT might be a possible choice of treatment for this population of patients and families.
AcknowledgementTrygFonden, Denmark awarded a grant to Nina Tejs Jørring to support this research.
留言 (0)