
記住我


The mRNA vaccines have been shown to be highly effective in preventing severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection and associated illness,1,2 although recent reports suggest reduced effectiveness against infection with the B.1.617.2 (or delta) variant.3,4 We assessed the effectiveness of the mRNA-1273 (Moderna) vaccine among incarcerated men during a coronavirus disease 2019 (Covid-19) outbreak that was dominated by transmission of the delta variant.
The Sierra Conservation Center (SCC), in Jamestown, California, is a low-to-medium security prison for men. No SARS-CoV-2 infections were detected among residents between April 23 and July 15, 2021. A substantial outbreak began on July 16, which resulted in 15% of the exposed population becoming infected by August 15, 2021 (Fig. S1 in the Supplementary Appendix, available with the full text of this letter at NEJM.org). The delta variant was identified in all 13 successfully sequenced positive samples that had been obtained from SCC residents from July 16 to July 21, 2021. The delta variant was also identified in all 6 successfully assayed positive samples obtained from SCC staff during this period.
We tracked infections over a 30-day period (July 16 to August 15, 2021) among SCC residents who had close exposure during that time; close exposure was defined as residence in a housing unit in which at least one case had been detected. Our goal was to estimate vaccine effectiveness against SARS-CoV-2 infection (with infection confirmed by means of polymerase-chain-reaction or antigen test) and symptomatic infection, defined as a case involving symptoms observed by prison health care staff or objective signs of fever (a temperature of ≥37.8°C) or hypoxemia (an oxygen saturation of <94%) within 3 days before to 10 days after the collection date of a sample that tested positive.
The mRNA-1273 vaccine accounted for 75% of all vaccines administered to SCC residents as of July 16, 2021. Residents who were fully vaccinated with the mRNA-1273 vaccine (i.e., had received a second dose at least 14 days previously) were matched with unvaccinated controls with the use of propensity scores (details are provided in the Supplementary Appendix). Vaccine effectiveness was calculated as one minus the risk ratio for full vaccination as compared with no vaccination.
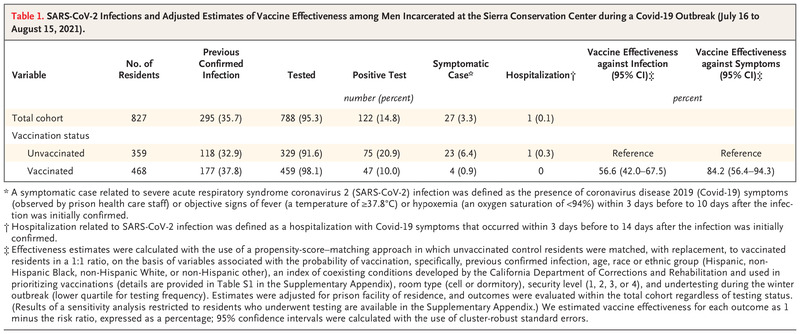
Table 1. Table 1. SARS-CoV-2 Infections and Adjusted Estimates of Vaccine Effectiveness among Men Incarcerated at the Sierra Conservation Center during a Covid-19 Outbreak (July 16 to August 15, 2021).
Table 1. SARS-CoV-2 Infections and Adjusted Estimates of Vaccine Effectiveness among Men Incarcerated at the Sierra Conservation Center during a Covid-19 Outbreak (July 16 to August 15, 2021). One quarter (827 of 3221) of the men residing at SCC in mid-July met eligibility criteria and were included in the study cohort; 468 were fully vaccinated and 359 were unvaccinated (Table 1). Residents in the study cohort underwent testing frequently throughout the study period (median, 3 tests; interquartile range, 2 to 5), and 95% were tested at least once (Fig. S3). There were 122 confirmed infections, including 27 symptomatic infections and 1 hospitalization. The estimated vaccine effectiveness was 56.6% (95% confidence interval [CI], 42.0 to 67.5) against infection and 84.2% (95% CI, 56.4 to 94.3) against symptomatic infection (Table 1). A total of 36% of cohort members had a previous confirmed infection at least 90 days before the study start date (median, 210 days since confirmed infection); among these residents, the estimated vaccine effectiveness against subsequent infection was 80.5% (95% CI, 52.8 to 92.0) (Table S3).
Our results indicate that the mRNA-1273 vaccine was quite effective against SARS-CoV-2 infection during a delta variant–driven outbreak in this high-risk, congregate setting. Although the effectiveness against infection was substantially lower than that estimated in studies conducted before the emergence of the delta variant,1,2 protection against symptomatic illness remained robust — an outcome consistent with other recent reports.5 Notably, full vaccination also conferred additional substantial protection against infection in men with previous confirmed infections.
Strengths of this study include detailed daily records of participants’ movements and health status coupled with a high rate of testing, which facilitated valid estimation of vaccine effectiveness. Limitations include a lack of comprehensive viral sequencing, a limited sample size, and the observational study design.
Despite the strong vaccine effectiveness we detected, especially against symptomatic infection, the outbreak at the SCC highlights the continuing risks that Covid-19 poses in congregate settings — even in settings that have achieved relatively high levels of vaccine coverage. Efforts to expand coverage for residents and staff, together with ongoing strategic use of nonpharmaceutical interventions (e.g., masking, testing, and reducing population size and density), should remain a high priority for preventing outbreaks and mitigating the spread of infection in this vulnerable population.
Elizabeth T. Chin, B.S.
Stanford University School of Medicine, Stanford, CA
[email protected]
David Leidner, Ph.D.
California Department of Corrections and Rehabilitation, Sacramento, CA
Yifan Zhang, Ph.D.
Elizabeth Long, M.S.
Lea Prince, Ph.D.
Stanford University School of Medicine, Stanford, CA
Ying Li, M.S.
California Correctional Health Care Services, Sacramento, CA
Jason R. Andrews, M.D.
David M. Studdert, L.L.B., Sc.D.
Jeremy D. Goldhaber-Fiebert, Ph.D.
Joshua A. Salomon, Ph.D.
Stanford University School of Medicine, Stanford, CA
Supported in part by the COVID-19 Emergency Response Fund from Stanford University, which was established with a gift from the Horowitz Family Foundation, and by grants from the National Institute on Drug Abuse at the National Institutes of Health (R37-DA15612), the Centers for Disease Control and Prevention (through the Council of State and Territorial Epidemiologists [NU38OT000297-02]), and the National Science Foundation Graduate Research Fellowship Program (DGE-1656518).
Disclosure forms provided by the authors are available with the full text of this letter at NEJM.org.
This letter was published on October 20, 2021, at NEJM.org.
5 References1. Dagan N, Barda N, Kepten E, et al. BNT162b2 mRNA Covid-19 vaccine in a nationwide mass vaccination setting. N Engl J Med 2021;384:1412-1423.
2. Thompson MG, Stenehjem E, Grannis S, et al. Effectiveness of Covid-19 vaccines in ambulatory and inpatient care settings. N Engl J Med 2021;385:1355-1271.
3. Fowlkes A, Gaglani M, Groover K, Thiese MS, Tyner H, Ellingson K. Effectiveness of COVID-19 vaccines in preventing SARS-CoV-2 infection among frontline workers before and during B.1.617.2 (Delta) variant predominance — eight U.S. locations, December 2020–August 2021. MMWR Morb Mortal Wkly Rep 2021;70:1167-1169.
4. Grannis SJ, Rowley EA, Ong TC, et al. Interim estimates of COVID-19 vaccine effectiveness against COVID-19–associated emergency department or urgent care clinic encounters and hospitalizations among adults during SARS-CoV-2 B.1.617.2 (Delta) variant predominance — nine states, June–August 2021. MMWR Morb Mortal Wkly Rep 2021;70:1291-1293.
5. Lopez Bernal J, Andrews N, Gower C, et al. Effectiveness of Covid-19 vaccines against the B.1.617.2 (delta) variant. N Engl J Med 2021;385:585-594.
留言 (0)