
記住我


Pregnant women with coronavirus disease 2019 (Covid-19) are at increased risk for adverse outcomes, and Covid-19 vaccination is recommended during pregnancy.1,2 However, safety data on Covid-19 vaccination during pregnancy remain limited.3,4
We performed a case–control study with data from Norwegian registries on first-trimester pregnancies, Covid-19 vaccination, background characteristics, and underlying health conditions (Supplementary Methods and Tables S1 through S3 in the Supplementary Appendix, available with the full text of this letter at NEJM.org). We identified all women who were registered between February 15 and August 15, 2021, as having had a miscarriage before 14 weeks of gestation (case patients) and those with a primary care–based confirmation of ongoing pregnancy in the first trimester (controls). In Norway, although vaccination during the first trimester is not recommended except in women with underlying risk conditions, women not yet aware that they were pregnant may still be vaccinated in the first trimester. We estimated odds ratios with 95% confidence intervals for Covid-19 vaccination within 5-week and 3-week windows before a miscarriage or ongoing pregnancy, adjusting for women’s age, country of birth, marital status, educational level, household income, number of children, employment in a health care profession, underlying risk conditions for Covid-19, previous test positive for severe acute respiratory syndrome coronavirus 2, and calendar month.
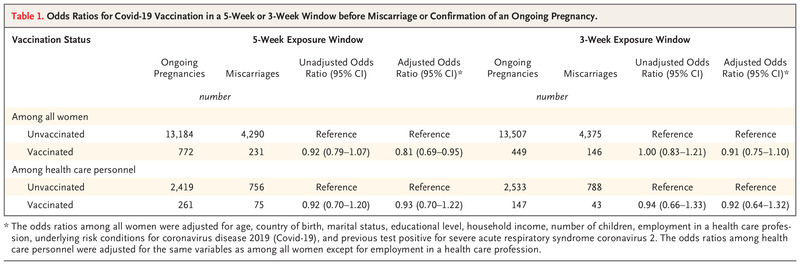
Table 1. Table 1. Odds Ratios for Covid-19 Vaccination in a 5-Week or 3-Week Window before Miscarriage or Confirmation of an Ongoing Pregnancy.
Table 1. Odds Ratios for Covid-19 Vaccination in a 5-Week or 3-Week Window before Miscarriage or Confirmation of an Ongoing Pregnancy. Among 13,956 women with ongoing pregnancies (of whom 5.5% were vaccinated) and 4521 women with miscarriages (of whom 5.1% were vaccinated), the median number of days between vaccination and miscarriage or confirmation of ongoing pregnancy was 19 (Fig. S2). Among women with miscarriages, the adjusted odds ratios for Covid-19 vaccination were 0.91 (95% confidence interval [CI], 0.75 to 1.10) for vaccination in the previous 3 weeks and 0.81 (95% CI, 0.69 to 0.95) for vaccination in the previous 5 weeks (Table 1). The results were similar in an analysis that included all available vaccine types (Table S5), in an analysis stratified according to the number of doses received (one or two) (Table S6), and in sensitivity analyses limited to health care personnel (for whom vaccination was routinely recommended other than in the first trimester) or women with at least 8 weeks of follow-up after confirmed pregnancy (to exclude subsequent pregnancy loss) (Table S7).
A limitation of our report is that the registry lacks information on gestational age at the time of early pregnancy registration, and thus we could not match case patients and controls according to gestational age. However, most recognized miscarriages are known to occur between pregnancy weeks 6 and 10,5 a period that is similar to the gestational ages at which women in Norway consult a physician to confirm pregnancy (Fig. S1). Also, only approximately 40% of women in Norway have a primary care appointment to confirm pregnancy, but the characteristics of these women appear to be similar to those of women who do not have a registered pregnancy confirmation (Table S4). We cannot address associations between vaccination and miscarriages that were not clinically recognized. Although adjustment for potential confounders had minimal effect on our results, the registry does not include information on lifestyle and other factors that might confound our findings (see Supplementary Appendix).
Our study found no evidence of an increased risk for early pregnancy loss after Covid-19 vaccination and adds to the findings from other reports supporting Covid-19 vaccination during pregnancy.3,4
Maria C. Magnus, Ph.D.
Håkon K. Gjessing, Ph.D.
Helena N. Eide, M.D.
Norwegian Institute of Public Health, Oslo, Norway
[email protected]
Allen J. Wilcox, M.D., Ph.D.
National Institute of Environmental Health Sciences, Durham, NC
Deshayne B. Fell, Ph.D.
School of Epidemiology and Public Health, University of Ottawa, Ottawa, ON, Canada
Siri E. Håberg, M.D., Ph.D.
Norwegian Institute of Public Health, Oslo, Norway
Supported in part by the Research Council of Norway (project number, 324312) and through its Centers of Excellence funding scheme (project number, 262700) and by NordForsk (project number, 105545). Dr. Magnus has received funding from the European Research Council under the European Union’s Horizon 2020 research and innovation program (grant agreement number, 947684). The funders had no role in the completion of the research project, the writing of the manuscript for publication, or the decision to submit the manuscript for publication.
Disclosure forms provided by the authors are available with the full text of this letter at NEJM.org.
This letter was published on October 20, 2021, at NEJM.org.
5 References1. Centers for Disease Control and Prevention. COVID-19 vaccines while pregnant or breastfeeding. August 11, 2021 (https://www.cdc.gov/coronavirus/2019-ncov/vaccines/recommendations/pregnancy.html).
2. National Health Service. Pregnancy, breastfeeding, fertility and coronavirus (COVID-19) vaccination. September 2, 2021 (https://www.nhs.uk/conditions/coronavirus-covid-19/coronavirus-vaccination/pregnancy-breastfeeding-fertility-and-coronavirus-covid-19-vaccination/).
3. Zauche LH, Wallace B, Smoots AN, et al. Receipt of mRNA Covid-19 vaccines and risk of spontaneous abortion. N Engl J Med 2021;385:1533-1535.
4. Kharbanda EO, Haapala J, DeSilva M, et al. Spontaneous abortion following COVID-19 vaccination during pregnancy. JAMA 2021 September 8 (Epub ahead of print).
5. Mukherjee S, Velez Edwards DR, Baird DD, Savitz DA, Hartmann KE. Risk of miscarriage among black women and white women in a U.S. prospective cohort study. Am J Epidemiol 2013;177:1271-1278.
留言 (0)