
記住我


An 82-year-old man presented with a 2-week history of fatigue, lethargy, memory loss, and right sided headache. His past medical history was significant for chronic obstructive pulmonary disease, coronary artery disease, stage 3 chronic kidney disease, and tobacco smoking. Neurologic examination revealed 2+ reflexes on the right upper extremity. Laboratory work-up was non-contributory. A brain MRI revealed a right frontal lobe mass, 4.2 cm in diameter, with thick and irregular peripheral enhancement, associated with marked surrounding edema, mass effect, and leftward 7-mm midline shift. Restricted diffusion in the central nonenhancing portion of the lesion suggested an abscess (Figure 1), but the possibility of a neoplasm could not be excluded.

Imaging and pathologic characteristics of Cladophialophora bantiana brain abscess: Left: Axial T1-weighted gadolinium-enhanced MRI showing a right frontal lesion with irregular peripheral enhancement; Right: Axial apparent diffusion coefficient sequence demonstrating true restricted diffusion in the non-enhancing central portion of the lesion, highly suggestive of an abscess
The patient underwent right stereotactic frontal craniotomy. After an 18-gauge spinal needle was inserted into the mass, purulent material was aspirated and sent to microbiology for culture. The mass was resected and sent to pathology.
The tissue contained a demarcated abscess cavity, 3 × 2.5 × 2 cm, with tan-green purulent material (Figure 2A).

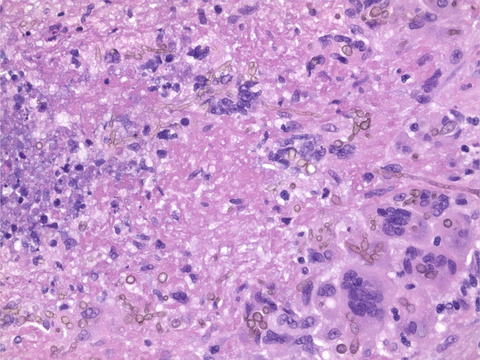
Imaging and pathologic characteristics of Cladophialophora bantiana brain abscess: (A) Macroscopic examination reveals cerebral abscess with purulent tan-green content; (B) Hematoxylin and eosin section reveals necrotizing granulomatous inflammation with peripheral palisading; (C) Fungal microorganisms are highlighted with the Fontana-Masson histochemical stain for melanin; (D) black mold colonies growing on inhibitory mold agar 6 days after inoculation; (E) a cellophane tape direct preparation depicting pigmented fungal hyphae with very long chains of conidia
On H&E section multiple necrotizing granulomas of various sizes were present with epithelioid histiocytes with vague peripheral palisading (Figure 2B). Occasional clusters of pigmented septated fungal hyphae were identified predominantly at the outer periphery of the necrotic areas, which were highlighted by Grocott's methenamine silver (GMS) and Fontana-Masson (Figure 2C).
A diagnosis of dematiaceous fungal brain abscess, pending culture, and typing, was communicated to the clinical team and anti-fungal treatment was started with oral voriconazole 200 mg twice per day, in combination with intravenous liposomal amphotericine B 5mg/kg per day for a week, until reaching therapeutic levels with voriconazole.
At day 6 after culturing on an inhibitory mold agar (IMA) many growing olivaceous-grey, suede-like colonies of mold were present (Figure 2D). A cellophane tape prep revealed dematiaceous hyphae with long chains of dark, oval to spindle-shaped conidia (Figure 2E), suspicious for Cladophialophora bantiana, a diagnosis confirmed by rDNA sequencing.
2 FINAL DIAGNOSISCladophialophora bantiana brain abscess.
3 DISCUSSIONApproximately 8% of brain abscesses are fungal, with a minority caused by melanin-producing dematiaceous fungi, the most common being C. bantiana, a ubiquitous saprophyte of soil plantation [1] and carbon-rich rocks [2], infamous for its ability to infect immunocompetent hosts [1, 2]. Given its natural distribution, over 80% of patients diagnosed with C. bantiana brain abscess report recent contact with soil [1], or occupational exposure from mining [2]. Sporadic cases are found worldwide, the majority in India, followed by the United States. Apart from brain abscesses secondary to direct spore inoculation caused by head trauma, the exact mechanism by which C. bantiana causes brain abscess is unclear, with hypotheses including primary cutaneous or subclinical respiratory tract infection with hematogenous spread to the brain [2]. Whole-genome sequencing of C. bantiana DNA performed by Kuan et al further elucidated its unique pathogenic properties. Having a genome length of 37.1 Mb, with 12155 predicted genes encoding 8444 hypothetical proteins, C. bantiana can produce antioxidant proteins of the superoxide dismutase, catalase, or reductase families in response to thermal stress, facilitating survival in human hosts [3]. The antioxidant properties of melanin may facilitate escape from host antimicrobial immune mechanisms and growth at body temperature, and its neurotropism may be related to its ability to process phenolic compounds, which are abundant in neural tissue [2]. Kantarcioglu et al. reported a predilection of C. bantiana brain abscess for men (>70%) with an average age of 35 years. About 60% of patients were previously healthy, but almost a third were using corticosteroids and a few were solid organ transplant recipients. Incubation time from initial exposure to the development of symptoms varies from a 4 weeks to many years. Most common symptoms include headache, altered mental status, seizures, nausea and vomiting as well as focal neurologic signs or symptoms [2]. As a result of the non-specificity of its presenting symptoms, the diagnosis of this type of infection may be markedly delayed, with some cases being diagnosed only in the post-mortem context [1]. In about half of patients, brain imaging will reveal a solitary ring-enhancing lesion, most frequently involving the frontal lobe. Half of patients have radiologically presented with multiple lesions, and a minority can present concurrent meningitis. Blood or cerebrospinal fluid cultures are usually negative, necessitating examination of an aspirate or a tissue biopsy for accurate diagnosis. Definitive diagnosis of C. bantiana infection requires molecular identification with rDNA sequencing [2]. Susceptibility testing has reported good activity of the triazoles voriconazole, posaconazole, and itraconazole [1]. However, treatment with antifungal med ications only has resulted in a mortality rate of 65%, which lowers to 50% with prior complete neurosurgical resection of the abscess [2]. Although no workplace transmission has been reported to healthcare laboratory workers and the probability of lab-acquired infection is considered as low, C. bantiana has been labeled as a biosafety level 3 agent and the use of appropriate measures, such as a biosafety cabinet, while handling potentially infectious specimens is recommended [2].
ETHICS APPROVALThe authors declare no conflicts of interest related to the present study.
留言 (0)