
記住我
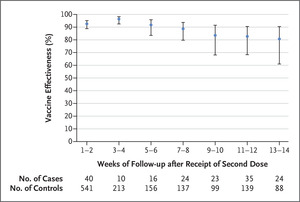
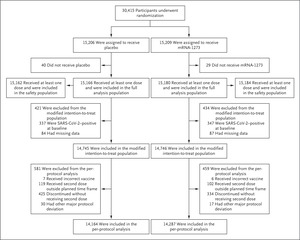
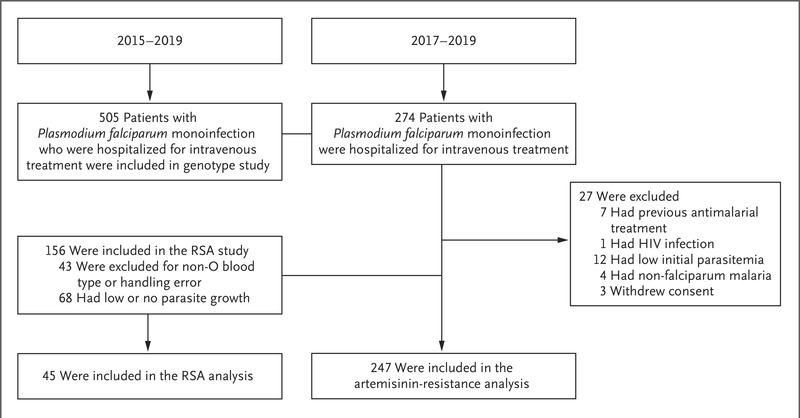

 Figure 1. Randomization and Analysis Populations.
Figure 1. Randomization and Analysis Populations. Eight participants, including six with major protocol deviations and two who erroneously underwent randomization twice, were excluded from the original randomization population (30,423 participants) and from all analysis sets. The full analysis population comprised all participants who had undergone randomization and received at least one injection; the modified intention-to-treat population included participants in the full analysis population who had no immunologic or virologic evidence of previous Covid-19 (i.e., had both a negative nasopharyngeal swab specimen and a negative anti-nucleocapsid antibody test result) at day 1 before the first injection; and the per-protocol population consisted of all participants in the modified intent-to-treat population who received planned injections according to the schedule and had no major protocol deviations that affected key trial data. The safety population included all participants who had undergone randomization and received at least one injection; this population was used for all safety analyses except the analysis for solicited adverse events. For safety analyses, participants were evaluated according to the injection received. Three participants assigned to the mRNA-1273 group received two doses of placebo and were included in the placebo safety population, and seven participants assigned to the placebo group received one or two doses of mRNA-1273 and were included in the mRNA-1273 safety population. The data cutoff date was March 26, 2021.
From July 27 to October 23, 2020, a total of 30,415 participants underwent randomization; 15,206 were assigned to the placebo group and 15,209 to the mRNA-1273 group (Figure 1 and Fig. S2).1 More than 96% of participants (14,727 in the placebo group and 14,635 in the mRNA-1273 group) received second injections. A total of 531 participants (3.5%) in the placebo group and 453 (3.0%) in the mRNA-1273 group did not receive the second injection, mainly owing to confirmed SARS-CoV-2 infection or withdrawal of consent. Trial discontinuations in the placebo group (691 participants [4.5%]) and the mRNA-1273 group (440 participants [2.9%]) were most commonly due to protocol deviations, withdrawal of consent, or loss to follow-up. The imbalance of discontinuations between the placebo and mRNA-1273 groups coincided with the FDA issuance of the EUAs for Covid-19 vaccines and reflected the intent of placebo recipients to receive a vaccine under EUA as it became available (Fig. S3). By the data cutoff date (March 26, 2021), 27,109 participants had been informed of their group assignments at a participant-decision visit, and 1855 had been informed before the participant-decision visit because they intended to receive a vaccine under EUA through their provider. A total of 28,964 participants entered the open-label phase of the trial.
Vaccine safety was assessed among 30,346 participants in the safety population (Figure 1). The prespecified primary efficacy analysis was performed in the per-protocol population, which included 28,451 participants who were SARS-CoV-2–negative at baseline and had received two doses of vaccine by the final analysis in the blinded phase. The median duration of follow-up from randomization to data cutoff or trial discontinuation was 212 days (interquartile range, 193 to 225), the duration from the second dose to data cutoff or discontinuation was 183 days (interquartile range, 165 to 194), and the duration from randomization to unblinding was 148 days (interquartile range, 131 to 162). Baseline demographic and clinical characteristics were balanced between the placebo group and the mRNA-1273 group (Table S5).1
SafetyAt the end of the blinded phase, the frequencies of solicited local and systemic adverse events were consistent with those reported previously,1 with such events occurring less frequently in the placebo group (in 48% and 43% of participants after the first and second injections, respectively) than in the mRNA-1273 group (88% and 92%) (Fig. S4 and Tables S6 through S13). Women were slightly more likely than men to have grade 3 solicited adverse events after the first and second injections (Table S8). Occurrences of solicited adverse events were generally similar with the two injections, regardless of severe Covid-19 risk status (Table S9), and were less common after both doses among participants with previous SARS-CoV-2 infection than among those without previous SARS-CoV-2 infection, with the exception of systemic adverse events after the first dose of mRNA-1273, which occurred more often in participants previously infected with SARS-CoV-2 (62% vs. 55%, respectively) (Tables S11 and S12). The incidence of local adverse events with delayed onset starting on day 8 after an injection was higher after the first injection (80 participants [0.5%]) than after the second injection (10 participants [<0.1%]), and the most common local adverse event reported on or after day 8 was erythema in the mRNA-1273 group after the first (68 participants [0.4%]) and second (6 [<0.1%]) injections (Table S13).
The frequencies of unsolicited, severe, and serious adverse events reported during the 28 days after either injection were generally similar in the two groups in the overall safety population, regardless of age or risk factors for severe Covid-19 (Tables S14 through S18). The frequency of grade 3 and medically attended adverse events that were considered to be related to injection of placebo or vaccine was lower in the placebo group (0.2% and 0.6%, respectively) than in the mRNA-1273 group (0.5% and 1.3%) (Table S14). Overall, 0.6% of placebo recipients and 0.4% of vaccine recipients had adverse events that resulted in their not receiving the second dose, and less than 0.1% in both groups discontinued trial participation because of adverse events after either injection. Adverse events that were considered to be related to the injections were reported by 8.5% of placebo recipients and 13.9% of mRNA-1273 recipients during the observation period of the study and were generally similar to those reported previously regardless of age (Tables S19 through S21). Serious injection-related adverse events occurred in 4 placebo recipients (<0.1%) and in 12 mRNA-1273 recipients (<0.1%).
Hypersensitivity reactions were reported in 1.8% of placebo recipients and in 2.2% of vaccine recipients, with anaphylaxis occurring in 2 participants (<0.1%) in each group (Table S22). Dermal filler reactions were reported in 14 placebo recipients (<0.1%) and in 20 mRNA-1273 recipients (0.1%) with a history of dermal filler injections (Table S23). Three cases of Bell’s palsy (<0.1%) were reported in the placebo group and 8 in the mRNA-1273 group (<0.1%); no case was considered to be related to the placebo or the vaccine (Table S24). Thromboembolic events were observed in 43 placebo recipients (0.3%) and in 47 mRNA-1273 recipients (0.3%) (Table S25). No cases of myocarditis were reported. Pericarditis events occurred in 2 participants each (<0.1%) in the placebo and mRNA-1273 groups (both events >28 days after the second dose) and were considered serious (Tables S20 and S21). A total of 32 deaths had occurred by completion of the blinded phase, with 16 deaths each (0.1%) in the placebo and mRNA-1273 groups; no deaths were considered to be related to injections of placebo or vaccine, and 4 were attributed to Covid-19 (3 in the placebo group and 1 in the mRNA-1273 group) (Tables S19 and S26). The Covid-19 death in the mRNA-1273 group occurred in a participant who had received only one dose; Covid-19 was diagnosed 119 days after the first dose, and the participant died of complications 56 days after diagnosis.
Efficacy Analyses Figure 2. Figure 2. Efficacy of the mRNA-1273 Vaccine in Preventing Covid-19.
Figure 2. Efficacy of the mRNA-1273 Vaccine in Preventing Covid-19. In Panels A and C, the dashed vertical line denotes the adjudicated assessment beginning at day 42 (14 days after the second injection of vaccine or placebo). Tick marks in all three panels indicate censored data. Vaccine efficacy was defined as 1 minus the hazard ratio (mRNA-1273 vs. placebo), and 95% confidence intervals were estimated with the use of a stratified Cox proportional-hazards model with Efron’s method of tie handling and with treatment group as a covariate, adjusted for stratification factor. The data cutoff date was March 26, 2021.
Figure 3. Figure 3. Vaccine Efficacy for Primary and Secondary End Points.
Figure 3. Vaccine Efficacy for Primary and Secondary End Points. Vaccine efficacy was defined as 1 minus the hazard ratio (mRNA-1273 vs. placebo), and 95% confidence intervals were estimated using a stratified Cox proportional-hazards model with Efron’s method of tie handling and with the treatment group as a covariate, adjusted for stratification factor. The P value for the vaccine efficacy against Covid-19 (upper right corner) is P<0.001. The dashed vertical line represents a vaccine efficacy of 30%, based on the null hypothesis that the primary efficacy of the mRNA-1273 vaccine is 30% or less. In the Covid-19 rows, censoring rules for efficacy analyses (Covid-19 cases based on eligible symptoms and positive reverse-transcriptase–polymerase-chain-reaction [RT-PCR] assay within 14 days before the second injection) were applied, except for deaths from Covid-19. If a participant had a positive RT-PCR assay at the visit before the second dose (day 29) without eligible symptoms within the previous 14 days, or a positive anti-nucleocapsid antibody test at a scheduled visit before Covid-19 was diagnosed, the participant’s data were censored at the date of the positive RT-PCR assay or anti-nucleocapsid antibody test. Covid-19 diagnoses were based on adjudication committee assessments. The data for Covid-19 regardless of previous SARS-CoV-2 status were based on the number of participants in the full analysis population (15,166 participants in the placebo group and 15,180 participants in the mRNA-1273 group). Data for the asymptomatic subgroup include data from the participant-decision visit. Asymptomatic was defined as the absence of symptoms (according to either the primary efficacy end point of Covid-19 or the secondary definition of Covid-19 [the Centers for Disease Control and Prevention definition, requiring only one symptom]) and of infection as detected by RT-PCR assay (at scheduled visits) or seroconversion (anti-nucleocapsid antibody test). In the primary approach, documented asymptomatic infection was counted beginning 14 days after the second injection, which required seroconversion at month 2 (day 57 through the participant-decision visit). Asymptomatic seroconversion excludes infections confirmed by RT-PCR assay only and includes infections confirmed by seroconversion and those confirmed by both RT-PCR and seroconversion (Table S28). Vaccine efficacy and 95% confidence intervals for asymptomatic SARS-CoV-2 infection were estimated with Fine and Gray’s subdistribution hazard model, with disease cases as competing events and with treatment group as a covariate, adjusted for stratification factor. Results for additional end points are summarized in Table S27. The data cutoff date was March 26, 2021. NE indicates that the lower bound of the 95% confidence interval could not be estimated.
Figure 4. Figure 4. Efficacy of the mRNA-1273 Vaccine in Preventing Covid-19 in Subgroups.
Figure 4. Efficacy of the mRNA-1273 Vaccine in Preventing Covid-19 in Subgroups. Analysis of the vaccine efficacy of mRNA-1273 in the prevention of Covid-19 in various subgroups in the per-protocol population was based on adjudicated assessments starting 14 days after the second injection. Vaccine efficacy, defined as 1 minus the hazard ratio (mRNA-1273 vs. placebo), and 95% confidence intervals were estimated with the use of a stratified Cox proportional-hazards model with Efron’s method of tie-handling and with the treatment group as a covariate, adjusted for stratification factor if applicable. The total number of events for race includes 38 placebo recipients and 3 mRNA-1273 recipients who were in “Multiple,” “Other,” or not reported or unknown categories, and the total number for ethnicity includes 4 placebo recipients and no mRNA-1273 recipients who were in not reported or unknown categories (not shown). Race and ethnic group were reported by the participant. The body-mass index (BMI) is the weight in kilograms divided by the square of the height in meters. Additional subgroup data are provided in Table S29. The data cutoff date was March 26, 2021. HIV denotes human immunodeficiency virus.
Figure 5. Figure 5. Incidence of Covid-19 According to Time Periods in the Per-Protocol Population.
Figure 5. Incidence of Covid-19 According to Time Periods in the Per-Protocol Population. The incidence rate based on adjudicated Covid-19 cases was defined as the number of participants with an event during the period divided by the number of participants at risk at the beginning of each period and adjusted by person-years (total time at risk) in each treatment group. The dashed vertical line represents a vaccine efficacy of 30% based on the null hypothesis that the primary efficacy of the mRNA-1273 vaccine is 30% or less. The number of person-years was calculated from randomization to the date of onset of Covid-19, the end of each time period, the last date of participation in the trial, or the efficacy data cutoff date, whichever date was the earliest. For the analysis of time intervals starting from 14 days after the first injection, starting from the second injection, and starting 14 days after the second injection, assessed every 2 months, person-years for each time period were defined starting from the beginning of each time interval and truncating at the end of the interval (if there was an ending time). Vaccine efficacy was defined as 1 minus the hazard ratio (mRNA-1273 vs. placebo). The 95% confidence interval for the ratio was calculated with the exact method, conditional on the total number of cases and adjusted for person-years for the time period. The data cutoff date was March 26, 2021.
A total of 799 adjudicated cases of Covid-19 in the per-protocol population were included in the primary efficacy analysis; 744 cases (5.3%) were in the placebo group and 55 (0.4%) were in the mRNA-1273 group (Figure 2 and Figure 3 and Tables S27 and S28). The vaccine efficacy was 93.2% for the prevention of Covid-19 starting at least 14 days after the second dose, with incidences of 136.6 cases per 1000 person-years (95% confidence interval [CI], 127.0 to 146.8) in the placebo group and 9.6 cases per 1000 person-years (95% CI, 7.2 to 12.5) in the mRNA-1273 group. The vaccine efficacy for adjudicated cases in the modified intention-to-treat population was 92.3% (95% CI, 90.1 to 93.9). Vaccine efficacy in preventing severe Covid-19, a key secondary end point, was 98.2% (95% CI, 92.8 to 99.6) in the per-protocol population, with 106 severe cases in the placebo group and 2 in the mRNA-1273 group. Vaccine efficacy was consistently high in subgroups, including participants 65 years of age or older and 75 years of age or older, those with coexisting conditions, those belonging to various racial and ethnic groups, and those with various categories of occupational risk exposures (Figure 4 and Table S29). When examined by specific time interval since completion of vaccination over the duration of follow-up, the efficacy of the mRNA-1273 vaccine in preventing Covid-19 remained consistent, with efficacy greater than 90% observed 4 months or more after the second injection (Figure 5, Fig. S5, and Table S30). Symptoms most commonly reported in the adjudicated Covid-19 cases in both groups were cough, fatigue, headaches, and nasal congestion; severe obesity and diabetes were contributing risk factors for severe Covid-19 (Tables S31 and S32).
Secondary end points (Figure 3 and Table S27) also included vaccine efficacy according to the secondary definition of Covid-19 (the Centers for Disease Control and Prevention definition, requiring only one symptom) starting 14 days after the second injection in the per-protocol population; according to the secondary definition, the vaccine efficacy was 93.4% (95% CI, 91.4 to 94.9). Among participants who were SARS-CoV-2–negative at baseline, a total of 712 participants (498 in the placebo group and 214 in the mRNA-1273 group) were found to be SARS-CoV-2–positive by RT-PCR assay or anti-nucleocapsid antibody test in the absence of symptoms starting 14 days after the second injection, through and including the participant-decision visit, and were considered to have asymptomatic infection (Figure 3 and Tables S27 and S28). Vaccine efficacy in preventing asymptomatic SARS-CoV-2 infection, based on the hazard ratio using the competing risk method, was 63.0% (95% CI, 56.6 to 68.5). In an analysis of asymptomatic infections after randomization, with data accrued up to and including the participant-decision visit, 157 participants in the placebo group and 153 in the mRNA-1273 group were RT-PCR–positive only; 306 participants in the placebo group and 48 in the mRNA-1273 group showed seroconversion by anti-nucleocapsid antibodies, and 115 participants in the placebo group and 7 in the mRNA-1273 group tested positive in both anti-nucleocapsid antibody testing and RT-PCR assay in the absence of symptoms. Findings for asymptomatic infection were similar in the modified intention-to-treat population (Table S28). For the secondary end point of prevention of SARS-CoV-2 infection (regardless of symptom or severity), the vaccine efficacy was 82.0% (95% CI, 79.5 to 84.2) beginning 14 days after the second injection in the per-protocol population, with 1339 participants in the placebo group and 280 in the mRNA-1273 group who had documented infection, defined as a positive result on RT-PCR assay at 14 days or more after the second injection or seroconversion at day 57 or later, through the participant-decision visit.
For the secondary end point of Covid-19 with onset at least 14 days after the first injection, the vaccine efficacy, based on adjudicated cases of Covid-19 in the per-protocol population among participants who received both injections (769 in the placebo group and 56 in the mRNA-1273 group), was 93.3% (95% CI, 91.1 to 94.9). In an exploratory analysis performed in a modified intention-to-treat subpopulation of 425 participants in the placebo group and 334 in the mRNA-1273 group who had no evidence of SARS-CoV-2 infection at baseline and who received only one injection, adjudicated Covid-19 cases were observed in 45 participants (10.6%) in the placebo group and in 4 participants (1.2%) in the mRNA-1273 group (Table S33). Six severe Covid-19 cases occurred in recipients of a single injection of placebo (1.4%), and one severe case occurred in a recipient of a single injection of the mRNA-1273 vaccine (0.3%).
留言 (0)